SALIVARY GLAND DISEASES ORAL MEDICINE AND RADIOLOGY FORMAT












 per 24 hours.")


")
")
 • • • FINE NEEDLE ASPIRATION CYTOLOGY OR BIOPSY MINOR OR")










































 Reccurence : removal of gland along")









")

 • POST PUBERTIAL MALE-ORCHITIS(2050 %) EPIDIDYMITIS")




 • Seen adults and children-mostly seen in dehydrated")


 -INCREASED SALIVAT")






 INCREASED SALIVATION")
 Excess salivation Etiology Medications-expectorant mixture Foreign body in mouth -dentures Rabies clinical sign")






- Slides: 97
SALIVARY GLAND DISEASES ORAL MEDICINE AND RADIOLOGY
FORMAT OF PRESENTATI ON • • • INTRODUCTION ANATOMY PHYSIOLOGY FUNCTIONS SALIVA-COMPOSITION DIAGNOSTIC TESTS CLASSIFICATION INDIVIDUAL DISEASE CONCLUSION
PAROTID MAJOR SALIVARY GLANDS SUBMANDIBULAR SUBLINGU AL MINOR SALIVARY GLANDS-
ANATOM Y PAROTID GLAND
ANATOM Y SUBMANDIBU LAR SALIVARYGLA ND
PAROTID GLAND q LARGEST OF SALIVARY GLANDS q LOCATION: q STENSONS DUCT q SEROUS IN NATURE
SUBMANDIBULAR SALIVARY GLAND MIXED SALIVA-BOTH SEROUS & MUCOUS LOCATION-FLOOR OF THE MOUTH WHARTSONS DUCT
SUBLINGUAL SALIVARY GLAND MUCOUS SALIVA LOCATION-FLOOR OF THE MOUTH LINGUAL FRENUM
MINOR SALIVARY GLANDS LABIAL BUCCAL INCISIVE LINGUAL PALATINE
PHYSIOLOGY OF SALIVARY GLANDS • SALIVA… • SECRETION • COMPOSITION • FUNCTIONS
• SALIVARY SECRETION…. PHYSIOLOG Y • CONTROLLED BY CNS SALIVARY GLAND • SYMPHATHETIC STIMULATIO • PARASYMPHATHETIC
Saliva • 600 to 700 ml (up to 1. 5 L) per 24 hours. • PH is 6. 7 (6. 2 – 7. 6) • Contribution of various glands: • Parotid: - 60 – 65% • Submandibular: - 20 – 30% • Sublingual: - 2 – 5% • Minor glands: - 6 – 7%
FACTORS INFLUENCING SALIVARY SECRETION • Taste and smell • Mechanical stimulation of oral mucosa and gingiva • Mastication of food • Chemical irritation of oral mucosa & stomach • Distension / irritation of oesophagus • Pregnancy
COMPOSITION OF SALIVA – Water : - 94. 0 – 99. 5% – Solids : - 6. 0% (un stimulated), 0. 5% (stimulated) • Organic constituents: -urea, uric acid, glucose, aminoacid, lactate, fatty acids, proteins like amylase, peroxidase, lysosyme, Ig. A, Ig. M, Ig. G. • Inorganic constituents: - Ca, Mg, F, HCO 3, K, Na, Cl, NH 4. • Gases: - CO 2, N 2, O 2. • constituents from oral cavity: - desquamative
FUNCTIONS OF SALIVA • Inhibition of dental caries –Water balance • Digestion (Amylase, Lipase) –Buffering action • Antibacterial (Lysozyme, Ig. A, Peroxidase, FLOW) –Hygienic action • Mineralization –Lubrication action –Taste of food • Protective Pellicle
INVESTIGATIONS IN SALIVARY GLAND DISEASE (DIAGNOSTIC APPROACH)
INVESTIGATIONS (DIAGNOSTIC APPROACH) • • • FINE NEEDLE ASPIRATION CYTOLOGY OR BIOPSY MINOR OR MAJOR SALIVARY GLAND BIOPSY SIALOCHEMESTRY SIALOENDOSCOPY SALIVARY GLAND IMAGING RADIOGRAPHS SIALOGRAPHY SALIVARY SCINTIGRAPHY CT MRI, ULTRA SOUND…
SIALO CHEMISTRY… q LAB ANALYSIS OF SALIVA q HELPS IN DETECTING PATHOLOGY EXAMPLE: v SJOGRENS SYNDROME – Ig. A , Ig. G Elevated v OBSTRUCTIVE PAROTITIS- Sodium , Potassium, Chloride re v SIALADENOSIS – phosphorus elevated.
SIALO ENDOSCOPY v Minimally invasive procedure v Diagnosis and treatment v Diagnosis of radiolucent calculi v Treatment of other diseases. Chronic sialadenitis
SALIVARY GLAND IMAGING
RADIOGRAPH-IOPA
RADIOGRAPH-MANDIBULAR OCCLUSAL
RADIOGRAPH……. EXTRA ORAL-LATERAL OBLIQUE
SIALOGRAPHY. . OLDEST PROCEDURE 1902 - Carpy Infusion of radio opaque contrast agent before imag
SALIVARY SCINTIGRAPHY… Provides functional study of salivary glands 99 m TC PERTECHNECTATE is injected IV Concentrated and excreted by glandular structures. ADV: Major salivary glands visualized at a time DIS ADV: Demonstrates little morphology(low image resolution) RADIONUCLEID SALIVARY GLAND
CT & MRI Displays both hard & soft tissues Better images of soft tissues Axial &coronal sections taken Less artifacts
ULTRASOUND SOLID MASS INEXPENSIVE WIDELY AVAILABLE PAINLESS NON INVASIVE CYSTIC MASS
CLASSIFICATION OF SALIVARY GLAND DISORDERS BASED ON ETIOLOGY
A. DEVELOPMENTAL DISORDERS APLASIA HYPOPLASIA ACCESSORY Salivary Gland And Ducts ABERRANT Salivary Glands DIVERTICULI
B. OBSTRUCTIVE DISORDERS MAJOR SALIVARY GLAND SIALOLITHIASIS MINOR SALIVARY GLAND MUCOCELE EXTRAVASATION RETENTION RANULA AND FOREIGN
FUNCTIONAL DISORDERS XEROSTOMIA PTYLASM
C. INFLAMMATORY & REACTIVE DISORDERS NECROTISING SIALOMETAPLASIA RADIATION INDUCED SIALADINITIS ALLERGIC SIALADENITIS
D. INFECTIOUS DISORDERS - OF SALIVARY GLAND q VIRAL INFECTIONS q BACTERIAL INFECTION
VIRAL DISEASES MUMPS q VIRAL INFECTIONS : HCV INFECTION HIV INFECTIONS CYTOMEGALOVIRUS INFECTION
BACTERIAL DISEASES ACUTE BACTERIAL SIALADENITIS CHRONIC OR RECURRENT SIALADENITIS
E. SYSTEMIC CONDITIONS WITH SALIVARY GLAND INVOLVEMENT METABOLIC CONDITIONS : Diabetes mellitus anorexia Bulimia Alcoholism
F. AUTOIMMUNE DISEASES: SJOGERNS SYNDROME MICKULIZ DISEASE
G. GRANULOMATOUS DISEASES: TUBERCULOSIS SARCOIDOSIS
SALIVARY GLAND TUMOURS : BENIGN PLEOMORPHIC ADENOMA WARTHINS TUMOUR MONOMORPHIC ADENOMA ONCOCYTOMA MALIGNANT MUCO EPIDERMOID CARCINOMA ADENOID CYSTIC CARCINOMA ACINIC CELL CARCINOMA BASAL CELL ADENOMAS ADENOCARCINOMA CANALICULAR ADENOMA LYMPHOMA CARCINOMA EX PLEOMORHIC ADENOMA
Classification of salivary gland neoplasms by the World health organization : Epithelial tumours Adenomas Pleomorphic adenoma Monomorphic adenoma Adenolymphoma Oxyphilic adenoma others Mucoepidermoid tumour Acinic cell tumour Carcinomas Adenoid cystic carcinoma Undifferentiated carcinoma Carcinoma in pleomorphic adenoma
NON INFLAMMATORY, NON NEOPLASTIC TUMORS Benign lymphoepithelial lesion Sialosis or SIALADENOSIS
DEVELOPMENTAL DISORDERS APLASIA of Salivary Gland HYPOPLASIA ACESSORY Salivary Ducts ABERRANT Salivary Glands DIVERTICULI MELKERSON ROSENTHAL SYNDROME
OBSTRUCTIVE DISORDERS q SIALOLITHIASIS q MUCOCELE q RANULA
SIALOLITHIASIS
SIALOLITHIASIS § sialolithiasis Major salivary gland – common Minor salivary gland - rare COMPOSITION Organic &inorganic substances
Submandibular gland commonly involved : 80 -90% PAROTID : 5 -15% SUBLINGUAL : 2 -5% ETHIOLOGY Predisposing factors for sialolith v Inflammation v Ductal irregularities v Anticholinergic drugs
CLINICAL PRESENTATION: Acute PAIN : O/E : Painful DURING MASTICATION Ductal orifice inflammed Bimanual palpation COMPLICATIONS : Due to stasis of saliva Infections Fibrosis Intermittent Swelling
OTHER COMPLICATIONS : DIAGNOSIS: Radiographic examination Plain film radiography Sialendoscopy Ultrasonography CT imaging Acute sialadenitis
DIFFERENTIAL DIAGNOSIS: Calcified lymph node Evulsed or embedded tooth Foreign body phlebolith TREATMENT: Acute phase : supportive measures Superficial calculi : manipulation Recurrent infection : surgical removal duct & gland
Lithotripsy : § Non invasive Complications Extracorporeal lithotripsy Intraductal lithotripsy
MUCOCELE
Def of mucocele: TYPES : Extravasation Retention EXTRAVASATION MUCOCELE Trauma – Minor salivary gland duct Commonest form Location : Lower lips Tongue Buccal mucosa Floor of mouth & retromolar region
RETENTION MUCOCELE Obstruction of duct by calculi § Accumulation of saliva & dilation of duct Contraction of scar tissue : injured minor salivary gland duct Location : Floor of the mouth
Superficial mucocele Deep mucocele Reccurent ones DIAGNOSIS: History Clinical exam Investigations Histo path : Histo path areas of spilled mucin Inflammation : Numerous foamy histiocytes
DIFFERENTIAL DIAGNOSIS: Salivary gland neoplasm Soft tissue neoplasm Vascular malformations Vesiculobullous lesions
TREATMENT : Surgical excision -New mucoceles Removal of gland to prevent reccurence Intra lesional steroids
RANUL A
Large mucocele – floor of the mouth Types : Extravasation Retention Risk factors : Trauma Obstruction üAssociated with sublingual salivary gland
Clinical presentation : RANULA – Swollen abdomen of frog Painless , slow growing Soft & Movable mass – Floor of mouth One side of lingual frenum Plunging ranula: Deep lesion herniation
TREATMENT : Surgical excision ( marsupialization procedure ) Reccurence : removal of gland along with the duct Intralesional steroids
INFLAMMATORY & REACTIVE LESIONS q NECROTIZING SIALOMETAPLASIA q RADIATION INDUCED PATHOLOGY q ALLERGIC SIALADENITIS
NECROTIZING SIALOMETAPLASIA
Benign self limiting reactive inflammatory disorder Mimics malignacy Initiated by local ischemic event CLINICAL PRESENTATION o Rapid onset o Palate Erythematous nodule Other sites : Males 50 yrs Lower lip retromolar area Mucosa breaks BM Deep ulceration
RISK FACTORS Trauma v ADMINISTRATION OF LOCAL ANAE v DENTAL PROCEDURES v BULIMIA
DIAGNOSIS v History v Clinical exam DIFFERENTIAL DIAGNOSIS ü Malignancy ü Gumma of tertiary syphlis Histopath findings Necrosis of salivary gland Pseudoepitheliomatous hyperplasia : mucosal epith Sq. metaplasia of salivary ducts § No malignant cells § Lobular architecture is preserved
TREATMENT Self limiting Heals by sec intention – 6 weeks Debridement & saline rinses
INFECTIONS VIRAL INFECTIONS : HIV INFECTIONS MUMPS HCV INFECTION CYTOMEGALOVIRUS INFECTION
MUMPS NON SUPPURATIVE PAROTITIS OR EPIDEMIC PAROTITIS
MUMPS
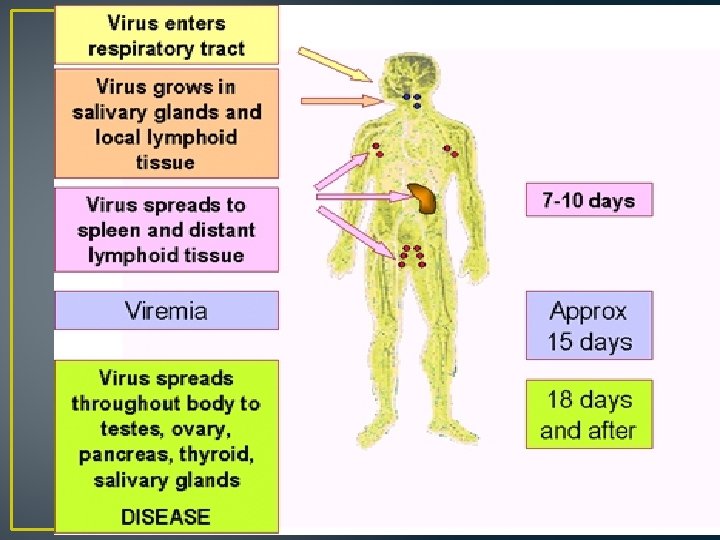
MUMPS NON SUPPURATIVE PAROTITIS EPIDEMIC PAROTITIS RISK FACTORS : RNA VIRUS ( Paramyxovirus ) Direct contact ; salivary droplets
Clinical presentation Children 4 -6 yrs Parotid –majority Adults diagnosis difficult Subman – 10% Incubation ; 2 -3 wks Preauricular pain Fever , malaise trismus Diffuse swelling Bilateral Edematous & tender -palp Duct inflammed
COMPLICATIONS OF MUMPS • CNS-MENINGITIS, ENCEPHALITIS (15% CASES) • POST PUBERTIAL MALE-ORCHITIS(2050 %) EPIDIDYMITIS • POST PUBERTIAL FEMALEOOPHPRITIS • PACREATITIS(2 -5 %) , THYROIDITIS • MYOCARDITIS • DEAFNESS( 1 IN 20, 000)
DIAGNOSIS NON SUPPURATIVE NATURE OF DISEASE NEGATIVE HISTORY OF MUMPS OR MUMPS VACCIN ACUTE PHASE OF THE DISEASE –SERUM AMYLASE LEVEL IS FOUR FOLD INCREASE IN ANTIBODY TITRE TO NORMAL S
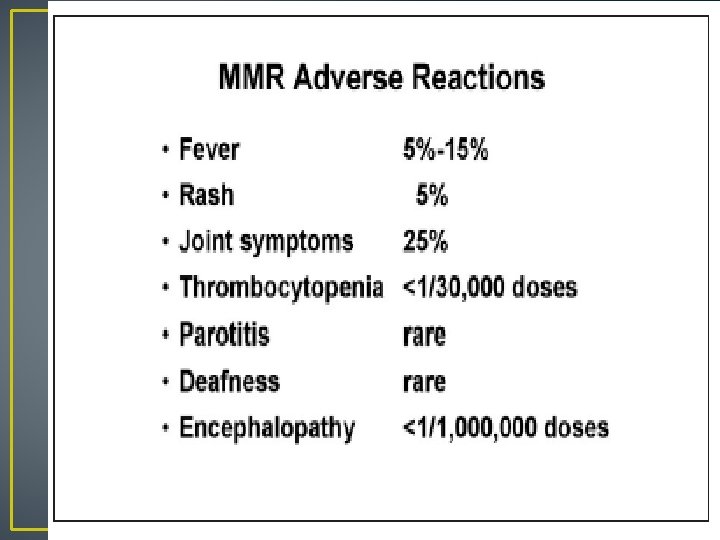
TREATMENT • SUPPORTIVE- IV FLUIDS BALANCED DIET BED REST • SYMPTAMATIC- ANTI INFLAMATORY DRUGS ANTIPYRETICS • PREVENTIVE- MMR VACCINE
MUMPS VACCINE MMR VACCINE Children 12 Months Or Above LIVE ATTENUATED VACCINE CDC RECOMMENDATIONS 1980 Severly immunocompromised : not recommended
BACTERIAL INFECTIONS ACUTE BACTERIAL SIALADENITIS CHRONIC OR RECURRENT SIALADENI
ACUTE BACTERIAL SIALADENITIS (ACUTE SUPPURATIVE PAROTITIS) • Seen adults and children-mostly seen in dehydrated and debilitated patients. • Caused by-Pencilline resistant staphylococcous aureus • Pre disposing factors • • • Dehydrated patients Poor oral hygiene Post surgical patients Chronic diseases Patient is on Drugs like- Antihistamines, sedatives tranquilizers
ACUTE BACTERIAL SIALADENITIS • Clinical features • Usually unilateral, sudden onset of pain at the angle of jaw • Difficulty in opening the mouth and speaking • Tender enlarged involved gland , overlying skin is red & warm • Purulent discharge from the duct on milking the gland • General symptoms like fever and malaise • Diagnosis- history and examination • purulent discharge from the duct • culture of purulent material • Treatment-high dose of antibiotics , fluid and
CHRONIC/recurrent BACTERIAL SIALADENITIS • Seen in young children and adults , many cases disappear at puberty • Etiology • idiopathic • ductal obstruction • congenital stenosis • h/o viral infection • Caused by-streptococcous viridans, E-coli • Sudden in onset, mild pain chronic, purulent discharge, unilateral • Symptoms lasts for a few week to month • After several episodes results in fibrosis of gland
FUNCTIONAL DISIRDERS OF SALIVARY GLAND XEROSTOMIA -DRY MOUTH SIALORRHEA (PTYLISM) -INCREASED SALIVAT
XEROSTOMIA -DRY MOUTH
XEROSTOMIA OR DRY MOUTH • Physiological • Agenesis of the gland • Mouth breathing • Aging factors • Fever and respiratory • Salivary gland disease • Auto immune disease • Post radiotherapy • Uncontrolled diabetes • Dehydration status • Drug induced sedatives , atropine,
XEROSTOMIA-PHYSIOLOGICAL CAUSE • • EXCESSIVE SPEAKING EXERCISE EXTREME EMOTIONS MOUTH BREATHING NASAL OBSRUCTION ENLARGED ADENOIDS DEVIATED NASAL SEPTUM NASAL POLYP MALOCCLUSION-CLASS-II Division-I
XEROSTOMIA –ETIOLOGY CAN BE CLASSIFIED Local factors : v Smoking v Mouth breathing : Systemic diseases v Sjogerns syndrome v Diabetes mellitus v Sarcoidosis & HIV
Clinical features : Dry mucosa & inflammation of oral mucosa, Residual saliva : thick and ropey Patient c/o diff in mastication & swallowing q INABILITY TO WEAR DENTUTR q. INCREASED INCIDANCE OF CARIES & ORAL CANDIDISIS History Diagnosis : Clinical examination Investigations
Treatment : TREAT THE CAUSE, FREQUENT SIPPING OF WATER Preventive: Candidiasis-candid mouth pain Caries- Oral prophylaxix - Fluoride mouth wash Hydration Symptomatic : Discontinue the drugs Artificial saliva-METHYL CELLULOSE 1% mouth Chewing gums Sialogogues: pilocarpine
SIALORRHEA(PTYLISM) INCREASED SALIVATION
SIALORRHEA(PTYLISM) Excess salivation Etiology Medications-expectorant mixture Foreign body in mouth -dentures Rabies clinical sign Heavy metal poisoning Local irritations –RAU, periodontal disease Mentally retarded pts Gastrointestinal reflux disease
Clinical features : Constant soiling of clothes DROOLING OF SALIVA Past medical history Diagnostic tests – salivary flow rate. Diagnosis : Treatment: Speech therapy Medications Injection : Surgical intervention: : Antihistamine : Atropine, belladona BOTULINUM TOXIN- PAROTID salivary gland excision (permanent relief) salivary duct ligation
AUTOIMMUNE DISEASES: SJOGRENS SYNDROME HENRIK SJOGREN : 1933 TYPES : PRIMARY & SECONDARY Exocrine glands EXOCRINE+ CT disorders CLINICAL TRIAD : Xerostomia , Xeropthalmia AND Rheumatoid arthritis
Predisposing factors : Auto immunity HLA antigen clinical features : 40 – 60 yrs Females Parotid involvement Xerostomia Xeropthalmia Miscellaneous features
Diagnosis : History &Exam Investigations: Opthalmologic test Salivary gland function test Connective tissue disorder test Opthalmologic test: v. Schirmers test v. Break up time test (BUT) v. Rose Bengal Dye test
Salivary flow rate Salivary gland function test: Salivary gland biopsy Lymphocytic infiltration Scintigraphy & Sialography Destruction of acinar units Connective tissue disorder test: +ve antisalivary antibody +ve rheumatoid factor Treatment : Xeropthalmia , xerostomia , CT disorders
AUTOIMMUNE DISEASES: MIKULIEZS DISEASE Benign lymphoepithelial lesion Middle aged woman Unilateral/bilateral swelling RISK FACTORS : Autoimmune Diagnosis : q Salivary gland biopsy üLymphocytic infiltration Genetic Viral Treatment : observation üDestruction of acini üEpimyoepithelial islands