SALIVARY GLAND DISEASES Developmental anomalies Sialadenitis Obstructive and

SALIVARY GLAND DISEASES -Developmental anomalies -Sialadenitis -Obstructive and traumatic lesions -Sjogren syndrome -Salivary gland tumours

Developmental anomalies u Aplasia u Atresia u Heterotopic salivary tissue

Sialadenitis Inflammatory disorders of the major salivary glands are usually the result of bacterial or viral infection but occasionally sialadenitis is due to other causes, such as trauma, irradiation, and allergic reactions

Acute bacterial sialadenitis Uncommon disorder principally involves the parotid gland. Acute parotitis is an ascending infection, that is, the bacteria reach the gland from the mouth by ascending the ductal system, the main organisms involved being Streptococcus pyogenes and Staphylococcus aureus. It was once a common postoperative complication in debilitated and dehydrated patients particularly following abdominal surgery, but is a rare complication nowadays.

Reduced salivary flow is the major predisposing factor and acute parotitis occurs in patients with Sjogren syndrome or following the use of drugs with xerostomic side effects. Acute infection may also arise in immunocompromised patients or as a result of acute exacerbation in a previously chronic sialadenitis. The latter is usually the cause when acute sialadenitis involves the submandibular gland.

The onset of acute sialadenitis is rapid. Clinically, it presents as swelling of the involved gland accompanied by pain, fever, malaise, and redness of the overlying skin. Pus may be expressed from the affected duct.

Acute bacterial sialadenitis

Chronic bacterial sialadenitis Chronic sialadenitis of the major salivary glands is usually a non-specific inflammatory disease associated with duct obstruction, and low-grade ascending infection. The submandibular gland is much more commonly involved than the parotid gland.

In cases where no cause of obstruction can be identified, the predisposing factor may be a disorder of secretion resulting in decreased salivary flow. The sialadenitis is usually unilateral, and the symptoms of recurrent tender swelling of the affected gland are mainly related to the associated obstruction
 may be demonstrated")
The duct obstruction, destruction of glandular tissue, and duct dilatation (sialectasia) may be demonstrated by sialography. In the submandibular gland, progressive chronic inflammation may result eventually in almost complete replacement of the parenchyma by fibrous tissue producing a firm mass that may be mistaken clinically for a neoplasm. This type of inflammatory reaction may be referred to as chronic sclerosing sialadenitis.

Chronic bacterial sialadenitis

Recurrent parotitis u is a rare disorder which can affect children or adults. Rarely the adult form may follow on from the childhood type, but in most cases it is probably due to persistence of factors, such as calculi or duct strictures, leading to recurrent attacks of low grade ascending infection.

The condition may be unilateral or bilateral and is associated with recurrent painful swelling of the gland. Pus may be expressed from the duct orifice. In most cases the condition resolves spontaneously by the time the patient reaches early adult life, but repeated infection may result in irreversible damage to the main duct predisposing to duct obstruction. This may lead to further episodes of ascending infection and damage and to recurrent parotitis in adult life.
 is an acute, contagious infection which often occurs in")
Viral sialadenitis Mumps (epidemic parotitis) is an acute, contagious infection which often occurs in minor epidemics and is caused by a paramyxovirus. It is the commonest cause of parotid enlarge mentand the commonest of all the salivary gland diseases. Although infection can occur at any age, it is most common in childhood.

The virus is transmitted by direct contact with infected saliva and by droplet spread, and has an incubation period of 2 3 weeks. Non specific prodromal symptoms of fever and malaise are followed by painful swelling of sudden onset involving one or more salivary glands.

The parotid glands are almost always involved, bilaterally in about 70 per cent of cases, and occasionally the submandibular and sublingual glands may be affected, but rarely without parotid involvement also. The salivary gland enlargement gradually subsides over a period of about 7 days. The virus is present in the saliva 2 3 days before the onset of sialadenitis and for about 6 days afterwards.

Occasionally in adults other internal organs are involved, such as testes, ovaries, central nervous system, and pancreas. Orchitis is the most common complication, occurring in about 20 per cent of cases of mumps in adult males. The diagnosis of mumps is usually made on clinical ground, after an attack immunity is long lasting and so recurrent infection is rare.

Obstructive and traumatic lesions Duct obstruction and trauma are important factors in the etiology of a number of salivary gland diseases, such as chronic sialadenitis in major glands and mucoceles in minor glands. Duct obstruction may be due to a blockage within the lumen or result from disease in or around the duct wall, such as fibrosis or neoplasia. Obstruction to the duct orifice is usually due to chronic trauma, for example from sharp cusps or overextended dentures, resulting in fibrosis and stenosis.

Obstructive and traumatic lesions u. Salivary calculi u. Mucocele u. Necrotizing sialometaplasia
 cause obstruction within the duct lumen and can occur at any")
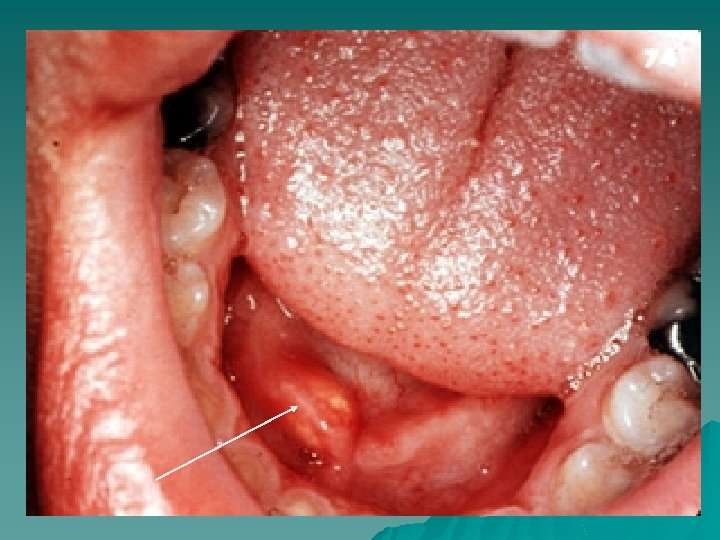
Salivary calculi (sialoliths) cause obstruction within the duct lumen and can occur at any age, but are most common in middle aged adults. Calculi may form in ducts within the gland or in the main excretory duct. Data on their distribution vary considerably but the submandibular gland is most frequently involved, accounting for about 70 90% of cases.

The parotid gland is the next most commonly involved, whereas sialolithiasis in sublingual and minor glands is uncommon and generally accounts for only about 2% of cases. Calculi are usually unilateral, although multiple stones in the same gland are not uncommon.

The typical signs and symptoms of calculi associated with major glands are pain and sudden enlargement of the gland, especially at meal times when salivary secretion is stimulated. The reduction in salivary flow predisposes to ascending infection and chronic sialadenitis.

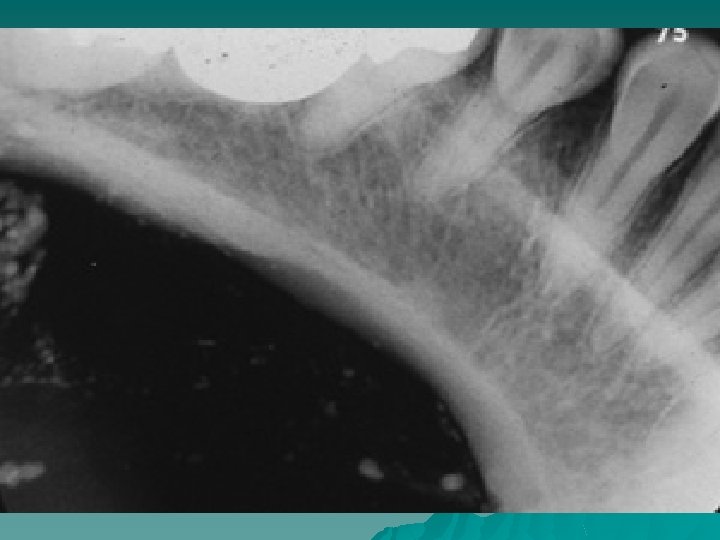
The calculi may be detected by palpation and on radiographs, and may be round or ovoid, rough or smooth, and vary considerably in size. They are usually yellowish in color and comprise mainly calcium phosphates with smaller amounts of carbonates. On section, they may be homogeneous but many have a lamellated structure.



MUCOCELE

MUCOCELE




Necrotizing sialometaplasia

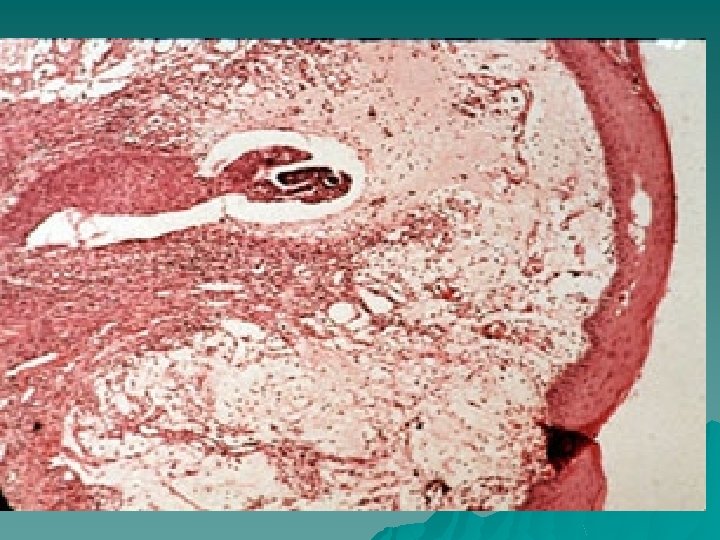
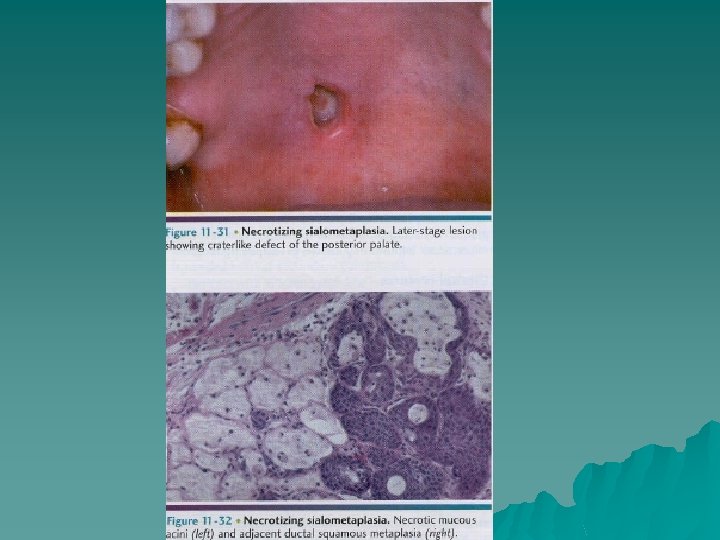
Necrotising sialometaplasia is a relatively uncommon disorder which clinically and on histological examination may be mistaken for malignant disease. It occurs most frequently on the hard plate. It presents most commonly as a deep crater like ulcer which may mimic a malignant ulcer and which may take up to eight weeks to heal.

Histopathological examination shows lobular necrosis of salivary glands, squamous metaplasia of ducts and acini, mucous extravasations, and prominent inflammatory cell infiltration. The surrounding palatal mucosa shows pseudoepitheliomatous hyperplasia and the histopathological features may be mistaken for either squamous cell carcinoma or mucoepidermoid carcinoma.

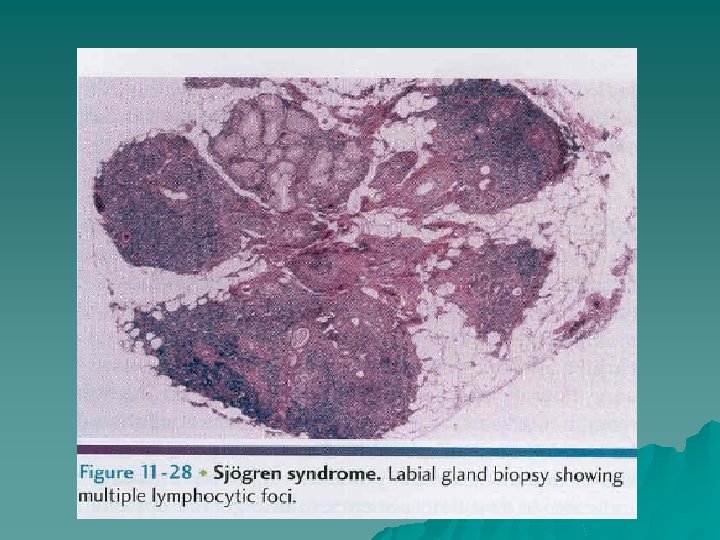
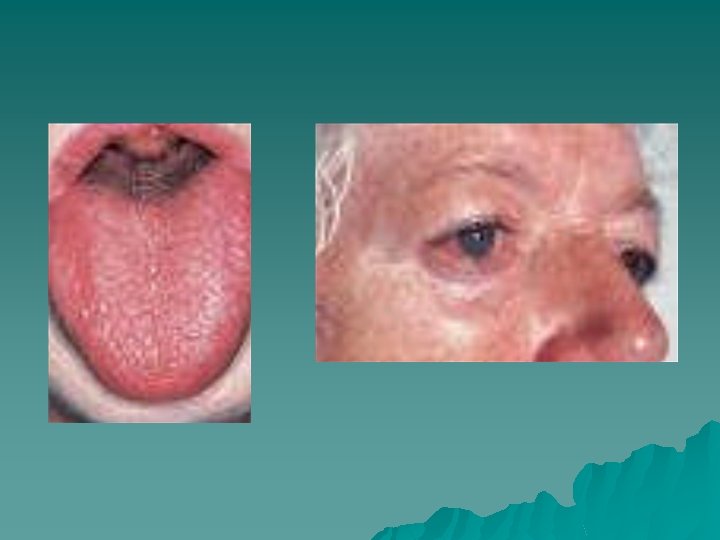
Sjogren syndrome is an immune mediated chronic inflammatory disease characterized by lymphocytic infiltration and acinar destruction of lacrimal and salivary glands.

Sjogren syndrome is classified into two groups: Primary Sjogren syndrome—the association of dry mouth (xerostomia) and dry eyes (xerophthalmia or keratoconjuctivitis sicca). Secondary Sjogren syndrome—the triad of xerostomia, xerophthalmia, and the connective tissue disease (usually rheumatoid arthritis)

Oral manifestations of Sjogren syndrome xerostomia predisposing to: candidosis caries sialadenitis oral dysfunction


Sjogren syndrome - investigations Labial gland biopsy to assess focal lymphocytic sialadenitis. u Autoantibody screen, especially for anti Ro and anti La antibodies. u Assessment of salivary gland involvement sialography or scintiscanning. u Assessment of salivary gland function salivary flow rates, sialochemical studies. u Ophthalmic opinion to assess ocular signs. u

- Slides: 48