S U O I T C TO E




















- Slides: 21
S U O I T C TO E F N I N O I T M ) C A 1 S U ( D S E O E. W R S T A DR N I ISE F. D RO P S A L E M
1 - UPPER RESPIRATORY INFECTIONS: Common Cold, Sinusitis, Pharyngitis, Epiglottitis and Laryngotracheitis
ETIOLOGY v Most upper respiratory infections are of viral etiology. v Epiglottitis and laryngotracheitis are exceptions with severe cases likely caused by Haemophilus influenzae type b. Bacterial pharyngitis is often caused by Streptococcus pyogenes.
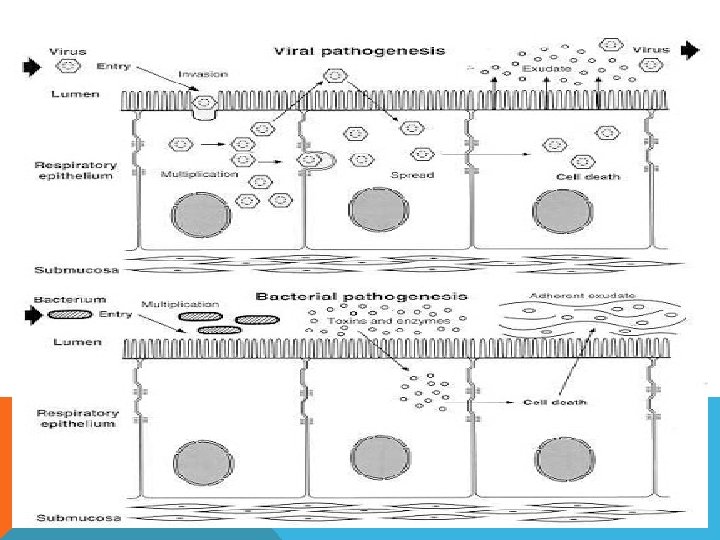
PATHOGENESIS v Organisms gain entry to the respiratory tract by inhalation of droplets and invade the mucosa. v Epithelial destruction may ensue, along with redness, edema, hemorrhage and sometimes an exudate.
CLINICAL MANIFESTATIONS v Initial symptoms of a cold are runny, stuffy nose and sneezing, usually without fever. v Other upper respiratory infections may have fever. Children with epiglottitis may have difficulty in breathing, muffled speech, drooling and stridor. v Children with serious laryngotracheitis (croup) may also have tachypnea, stridor and cyanosis.
MICROBIOLOGIC DIAGNOSIS: v Common colds can usually be recognized clinically. v Bacterial and viral cultures of throat swab specimens are used for pharyngitis, epiglottitis and laryngotracheitis. v Blood cultures are also obtained in cases of
PREVENTION AND TREATMENT: v Viral infections are treated symptomatically. v Streptococcal pharyngitis and epiglottitis caused by H. influenzae are treated with antibacterials. v Haemophilus influenzae type b vaccine is commercially available and is now a basic component of childhood immunization program.
2 - LOWER RESPIRATORY INFECTIONS Bronchitis. Bronchiolitis and Pneumonia.
ETIOLOGY: v Causative agents of lower respiratory infections are viral or bacterial. v Viruses cause most cases of bronchitis and bronchiolitis. v The most common bacterial agent is Streptococcus pneumoniae. v Atypical pneumonias are cause by Mycoplasma pneumoniae, Chlamydia spp, Legionella, Coxiella burnetti and viruses. v Nosocomial pneumonias and pneumonias in immunosuppressed patients have etiology with gram-negative organisms and Staphylococci.
PATHOGENESIS: v Organisms enter the distal airway by inhalation, aspiration or by hematogenous seeding. v The pathogen multiplies in or on the epithelium, causing inflammation, increased mucus secretion, and impaired mucociliary function! v other lung functions may also be affected. In severe bronchiolitis, inflammation and necrosis of the epithelium may block small airways
CLINICAL MANIFESTATIONS: v Symptoms include cough, fever, chest pain, tachypnea and sputum production. v Patients with pneumonia may also exhibit non-respiratory symptoms such as confusion, headache, myalgia, abdominal pain, nausea, vomiting and diarrhea.
MICROBIOLOGIC DIAGNOSIS: v Sputum specimens are cultured for bacteria, fungi and viruses. v Culture of nasal washings is usually sufficient in infants with bronchiolitis. Fluorescent staining technic can be used for legionellosis. v Blood cultures and/or serologic methods are used for viruses, rickettsiae, fungi and many bacteria. v Enzyme-linked immunoassay methods can be used for detections of microbial antigens as well as antibodies. v Detection of nucleotide fragments specific for the microbial antigen in question by DNA probe or polymerase chain reaction can offer a rapid diagnosis.
PREVENTION AND TREATMENT: v Symptomatic treatment is used for most viral infections. Bacterial pneumonias are treated with antibacterials. v. A polysaccharide vaccine against 23 serotypes of Streptococcus pneumoniae is recommended for individuals at high risk.
UPPER RESPIRATORY INFECTIONS. v Infections of the respiratory tract are grouped according to their symptomatology and anatomic involvement. Acute upper respiratory infections (URI) include the common cold, pharyngitis, epiglottitis, and laryngotracheitis. v Etiologic agents associated with URI include viruses, bacteria, mycoplasma and fungi. Respiratory infections are more common in the fall and winter when school starts and indoor crowding facilitates transmission.
UPPER AND LOWER RESPIRATORY TRACT INFECTIONS.
COMMON COLD Most colds are caused by viruses. Rhinoviruses with more than 100 serotypes are the most common pathogens. Coronaviruses may be responsible for more than 10% of cases. Adenoviruses and influenza viruses have all been linked to the common cold syndrome.
PATHOGENESIS. The viruses appear to act through direct invasion of epithelial cells of the respiratory mucosa, but whethere is actual destruction and sloughing of these cells or loss of ciliary activity depends on the specific organism involved. There is an increase in both leukocyte infiltration and nasal secretions, including large amounts of protein and immunoglobulin, suggesting that cytokines and immune mechanisms may be responsible for some of the manifestations of the common cold.
CLINICAL MANIFESTATIONS. After an incubation period of 48– 72 hours, classic symptoms of nasal discharge and obstruction, sneezing, sore throat and cough occur in both adults and children. Myalgia and headache may also be present. Fever is rare. The duration of symptoms and of viral shedding varies with the pathogen and the age of the patient. Sinusitis and otitis media may follow.
MICROBIOLOGIC DIAGNOSIS. The diagnosis of a common cold is usually based on the symptoms (lack of fever combined with symptoms of localization to the nasopharynx). Unlike allergic rhinitis, eosinophils are absent in nasal secretions. Although it is possible to isolate the viruses for definitive diagnosis, that is rarely warranted.
PREVENTION AND TREATMENT. Treatment of the uncomplicated common cold is generally symptomatic. Decongestants, antipyretics, fluids and bed rest usually suffice. Restriction of activities to avoid infecting others, along with good hand washing, are the best measures to prevent spread of the disease. No vaccine is commercially available for cold prophylaxis.