Rowing and OMT American College of Osteopathic Pediatricians

















































- Slides: 57
Rowing and OMT American College of Osteopathic Pediatricians Shannon Moore, DO Robert Hostoffer, DO
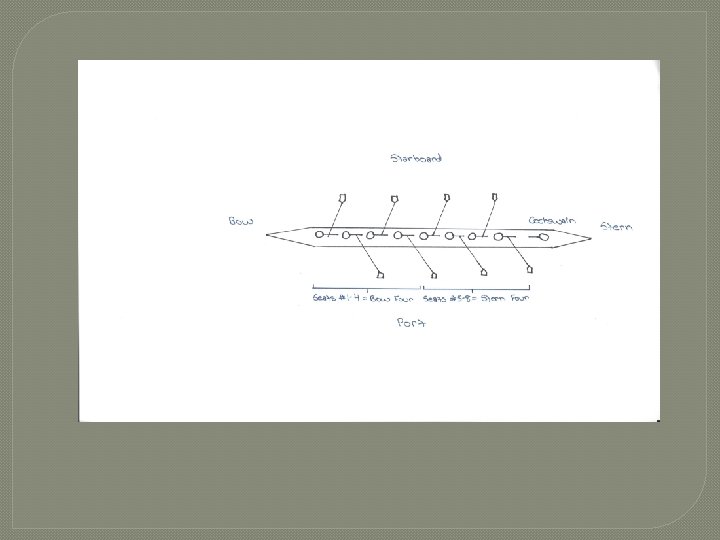
� The basic rowing action is a coordinated muscle action that requires application of force in a repetitive, maximal and smooth manner. Every large muscle group will contribute to this action. The rowing action has been divided into the following sequence: � The Catch � The Drive • Leg emphasis • Body swing emphasis • Arm pull through emphasis � The Finish Recovery
Catch � The erector spinae muscles of the back are relaxed to allow for trunk flexion, which is provided by the abdominals. � The psoas major and minor and the iliacus flex the pelvis and hips. � The sartorius muscle rotates the thighs. � The hamstrings and gastrocnemius are contracting while the knees are in flexion. � The quadriceps are elongated and stretched, yet the rectus femoris is contributing to hip flexion. � The ankles are dorsiflexed by the tibialis anterior. � The elbows are extended by the triceps brachii. � The grip on the handle is accomplished by the flexor muscles of the fingers and thumb.
The Drive � Legs Emphasis � The quadriceps extend the knee. � The feet are plantar flexed by the soleus and gastrocnemius muscles. � A number of stabilizing muscles aid in supporting the lower back. � All the muscles of the shoulder are contracting. These include the supra and infraspinatus, subscapularis, teres major and minor, and the biceps brachii. � The scapula is stabilized by the serratus anterior and trapezius muscles.
Body Swing �As the knees are finishing their extension, the hip is also extending by the contraction of the gluteus and hamstring muscles. Back extension is occurring by contraction of the erector spinae. �In the upper body, elbow flexion is occurring via the biceps, brachialis, and the brachioradialis muscles.
Arm pull through emphasis � � � � � The knees are maximally extended, and the ankles are plantar flexed. In addition, hip and back extension are being completed. The upper body musculature is contracting with high force to finish the drive. The elbow flexors are dominant. The flexor and extensor carpi ulnaris muscles of the forearm contract to stabilize and adduct the wrist. The shoulder is extended and adducted. The upper arm is internally rotated by the latissimus dorsi and pectoralis major. The teres minor, posterior deltoid, and long head of the biceps are acting on the shoulder joint. The scapula is rotated downward by the pectoralis minor and then drawn backward by the trapezius and rhomboid muscles.
The finish �The knees and ankles remain constant as the hips complete a full extension. � The back extensors are continually contracting, and the upper arms are internally rotated by the contracting latissimus dorsi. �The triceps are extending the elbows slightly.
The Recovery � The arms are pushed forward and away from the body by the triceps until the elbows reach full extension. � The anterior deltoids contract along with the coracobrachialis and biceps, and the upper arms raise slightly as they pass over the extended knees. � The abdominals flex the torso, and once the hands have cleared the extended knees, the slide begins its forward motion through ankle dorsiflexion and hip and knee flexion.
Rowing injuries � � low back, mainly due to excessive hyperflexion and twisting, and can include specific injuries such as spondylolysis, sacroiliac joint dysfunction and disc herniation Rib stress fractures account for the most time lost from on-water training and competition. • costochondritis, • costovertebral joint subluxation • and intercostal muscle strains � � � Shoulder pain is quite common in rowers and can be the result of overuse, poor technique, or tension in the upper body. Injuries concerning the forearm and wrist are also common, and can include exertional compartment syndrome, lateral epicondylitis, de. Quervain's and intersection syndrome, and tenosynovitis of the wrist extensors Am J Sports Med. 2009 Jun; 37(6): 1193 -9. Epub 2009 Mar 19.
�generalised patellofemoral pain due to abnormal patellar tracking �iliotibial band friction syndrome �Bilateral atraumatic medial meniscal tears �blisters and abrasions �BMJ Case Rep. 2009; 2009. pii: bcr 11. 2008. 1258. Epub 2009 May 17.
Case records of the Massachusetts General Hospital. Case 10 -2007. A 55 -year-old man impaled in a rowing accident. N Engl J Med. 2007 Mar 29; 356(13): 1353 -60
Caused by �overuse, �poor technique, �or tension in the upper body
12 month study prospective cohort of injuries in international rowers � 20 rowers �Greatest numbers of injuries was to lumber spine • Half of the injuries �Followed by knees �Followed by cervical spine �Br J Sports Med. 2010 Feb; 44(3): 207 -14. Epub 2008 Aug 21.
RIB OMT
A. Pump handle motion = upper ribs B. Bucket handle motion= lower ribs
Ribs 1 -5
Ribs 6 -10
Caliper motion ribs 11 -12
Rib Evaulation • Place the fingertips of the anterior hand against the costochondral junction, and those of the posterior hand at the rib head of the same rib. Palpate along the region for tissue texture changes and somatic dysfunction in the individual ribs based on respiratory motion. •
Terminology – For Board Review �Think “somatic dysfunction does” and name the dysfunction for what it likes to do: • Exhalation dysfunction: the ribs do not rise with inhalation but move easily with exhalation • Inhalation dysfunction: the ribs rise easily with inhalation but do not lower with exhalation
More Terminology – For Board Review �Exhalation dysfunction: • Pump handle: ribs are stuck down in the front and up in the back • Bucket handle: ribs are stuck down and in • Caliper: ribs are stuck pincing in �Inhalation dysfunction: • Pump handle: ribs are stuck up in the front and down in the back • Bucket handle: ribs are stuck up and out • Caliper: ribs are stuck pincing out
Which is the ‘key rib’? �When Treating Groups of Ribs: • Exhalation dysfunction: treat the upper rib in the group (frees up all ribs below it) • Inhalation dysfunction: treat the lower rib of the group (this rib is holding all ribs above it in an inhaled position) �Using Functional Methods Diagnosis: • This approach will lead to the key rib because you are comparing each rib with the one above and the one below. You are finding the one that doesn’t move.
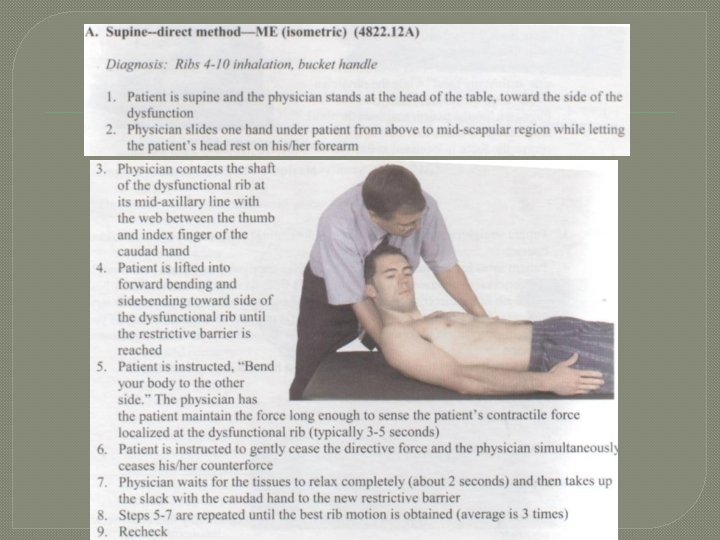
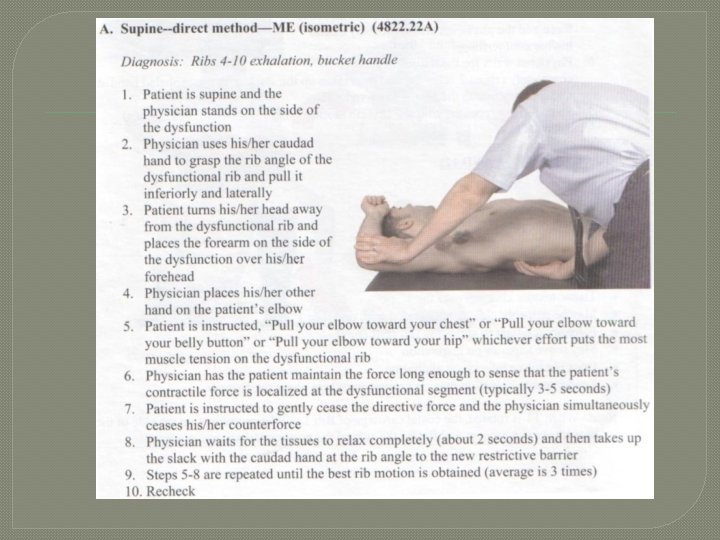
Treatments � Techniques: • Muscle Energy • Rib raising • Respiratory diaphragm facilitation/release • Soft tissue techniques • HVLA (consider patient’s age and history) � With all techniques used, one must determine the patient’s condition/medical stability and to which techniques their body will best respond
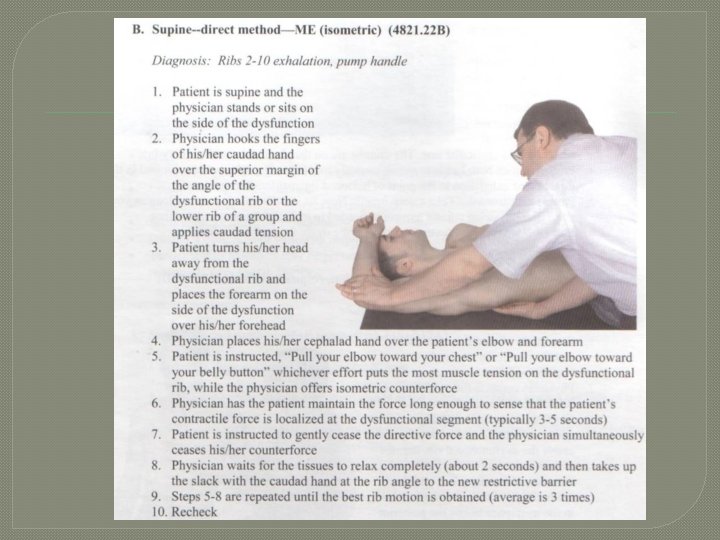
Muscle Energy �Easy to do for your hospitalized patient on bed rest/limited activity �Know which muscle groups you want to activate depending on the dysfunctional ribs involved • Pectoralis minor muscle for upper ribs (3 -5) • Serratus anterior muscle for middle ribs (4 -9) • Latissimus dorsi muscle for lower ribs (7 -12)
Rib-Raising
Demonstrate the procedure on patient in front of director
Thumb Pressure
Demonstrate the procedure on patient in front of director
Thoracic myofacial
Demonstrate the procedure on patient in front of director
Lateral Recumbent under the shoulder
Demonstrate the procedure on patient in front of director
OMT Lumbar Spine
Myofascial Stretching �Patient is prone. Place thumb onto paraspinal muscles adjacent to the vertebral spinous process. In a bowing like motion stretch the muscles away from you and release. Perform slowly.
Demonstrate the procedure on patient in front of director
Lumbar rotation technique �Patient is supine. Have the patient lace fingers behind head. Standing to the side of the patient grab the patient’s contra lateral upper arm and pull toward you and caudally.
Demonstrate the procedure on patient in front of director
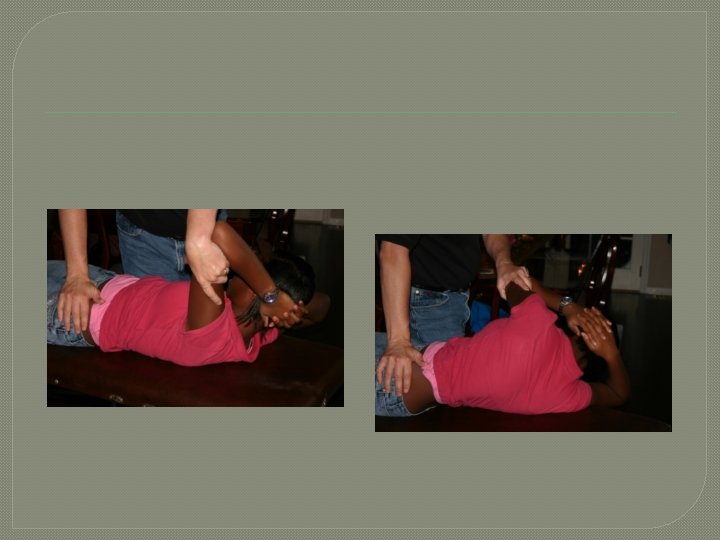
Lumbar Mobilization � The patient is in the lateral recumbent position. The side that the dysfunctional vertebra is rotated towards is up (eg, for a left rotated lumbar, the patient is lying on their RIGHT side). The patients upper most leg is dropped over the side of the table. The patients upper elbow is flexed. The lower elbow is also flexed and the arm is tucked under the head. Stand to the side of the patient with his/her face to you. Your one arm should be placed onto the upper elbow and the other arm placed on the upper hip. A twisting motion is performed by moving the patients elbow backward and the patient’s upper hip forwards, carrying the dysfunctional vertebra into correct position
Demonstrate the procedure on patient in front of director
Innervation Table Organ/System EENT Parasympathetic Sympathetic Ant. Chapman's Post. Chapman's T 1 -T 4 T 1 -4, 2 nd ICS Suboccipital Heart Cr Nerves (III, VII, IX, X) Vagus (CN X) T 1 -T 4 T 3 sp process Respiratory Vagus (CN X) T 2 -T 7 T 1 -4 on L, T 23 rd 3 & 4 th ICS Esophagus Vagus (CN X) T 2 -T 8 --- T 3 -5 sp process --- Foregut Vagus (CN X) T 5 -T 9 (Greater Splanchnic) --- Stomach Vagus (CN X) T 5 -T 9 (Greater Splanchnic) T 6 -7 on L Liver Vagus (CN X) T 5 -T 9 (Greater Splanchnic) 5 th-6 th ICS on L Rib 5 on R Gallbladder Vagus (CN X) T 5 -T 9 (Greater Splanchnic) Rib 6 on R T 6 Spleen Vagus (CN X) T 5 -T 9 (Greater Splanchnic) Rib 7 on L T 7 Pancreas Vagus (CN X) Rib 7 on R T 7 Midgut Vagus (CN X) T 5 -T 9 (Greater Splanchnic), T 9 T 12 (Lesser Splanchnic) Thoracic Splanchnics (Lesser) Small Intestine Vagus (CN X) T 9 -T 11 (Lesser Splanchnic) Ribs 9 -11 T 8 -10 Appendix T 12 Tip of 12 th Rib T 11 -12 on R Hindgut Lumbar (Least) Splanchnics Ascending Colon Pelvic Splanchnics (S 24) Vagus (CN X) Transverse Colon Vagus (CN X) Descending Colon & Rectum T 9 -T 11 (Lesser Splanchnic) T 5 -6 --- --- --T 10 -11 T 9 -T 11 (Lesser Splanchnic) R Femur @ hip Near Knees Pelvic Splanchnic (S 2 -4) Least Splanchnic L Femur @ hip T 12 -L 2 Pelvic Splanchnics (S 24) T 8 -L 2 --- ---
Questions � 1. The most common injury that rowers experience occurs to what structure: • • • A. Knees B. Neck C. Lumbar spine D. Elbows E. Thoracic spine
Questions � 2. The bucket handle motion occurs in what rib set: • • • A. rib 1 -5 B. rib 6 -10 C. rib 11 -12 D. floating ribs E. cervical ribs
Questions � 3. Shoulder pain in a rower is usually from all of the above except: • • A. poor technique B. overuse C. tension in the upper body D. idiot for a coxman
Ready…Row