Round worms INTRODUCTION Ascaris lumbricoides is the largest

Round worms

 parasitizing the human intestine. •")
INTRODUCTION • Ascaris lumbricoides is the largest nematode (roundworm) parasitizing the human intestine. • Ascaris lumbricoides is an intestinal worm found in the small intestine of man (mainly in the jejunum and upper part of the ileum). • They are more common in children than in adults • As many as 500 to 5000 adult worms may inhabit a single host.

Common name: - Giant Intestinal round worms. Disease: -Ascariaisis Host : - The human is intermediate and final host. Location in Definitive host : the adult worm: in small intestines. larva: in lung. Infective stage : - embryonated eggs

Geographical distribution • Worldwide • High prevalence in underdeveloped countries that have poor sanitation (parts of Asia, South America and Africa) • Occurs during rainy months, tropical and subtropical countries • Even occurs in rural areas in the United States

MORPHOLOGY • It is a elongated, cylindrical and tapering at both ends. • Sexes areseparate • The female is longer than male 25 – 40 cm long, 4 -6 mm in diameter. • Male is smaller being 15 -30 cm long, 2 -4 mm in diameter. • The posterior end of male is curved ventrally in the form of a hook • The digestive and respiratory organs of the worm float inside the body cavity possessing a toxic fluid known asascaron

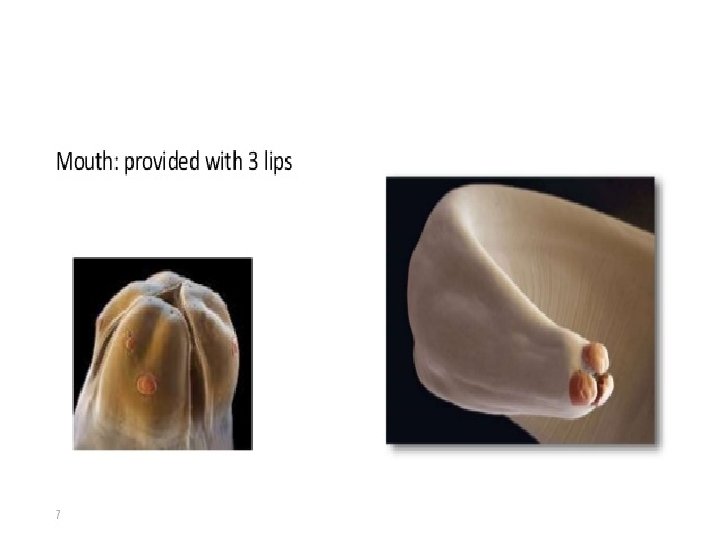
The Mouth Parts • The mouth opens at the anterior end. • It is surrounded by three finely toothed lips. • The lips are one dorsal and two ventrolateral. • These lips bear sensory structures called labial papillae

Adult worms of A. lumbricoides

A mature female A. lumbricoides lays enormous number of eggs (nearly 2, 000 eggs daily) which are passed in the faeces There are two kinds of the eggs. They are fertilized eggs, and unfertilized eggs We usually describe an egg in 5 aspects: size, color, shape, shell and content Decorticated eggs: Both fertilized and unfertilized eggs sometimes may lack their outer albuminous coats and are colorless

Fertilized Egg Broad oval in shape, brown in color, an average size 60× 45µm. The shell is thicker and consists of chitinous layer, and mammillated albuminous coat stained brown by bile. The content is a fertilized ovum. There is a new-moon(crescent) shaped clear space at the each end inside the shell.

Unfertilized egg Narrower and longer and measure 90 µm in length and 55 µm in breadth They are bile stained and brown in colour The chitinous layer and albuminous coat are thinner and irregular than those of the fertilized eggs The content is made of small atrophied ovum suurounded by many refractable granules of various size. Heaviest of all the helminthic eggs

Decorticated eggs Both fertilized and unfertilized eggs sometimes may lack their outer albuminous coats and are colorless.

Modes of transmission • Occurs mainly via ingestion of water or food (raw vegetables or fruits in particular) contaminated with A. lumbricoides eggs. • Occasionally inhalation of contaminated dust • Children playing in contaminated soil may acquire the parasite from their hands • Enhanced by the fact that individuals can be asymptomatically infected and continues to shedeggs for years

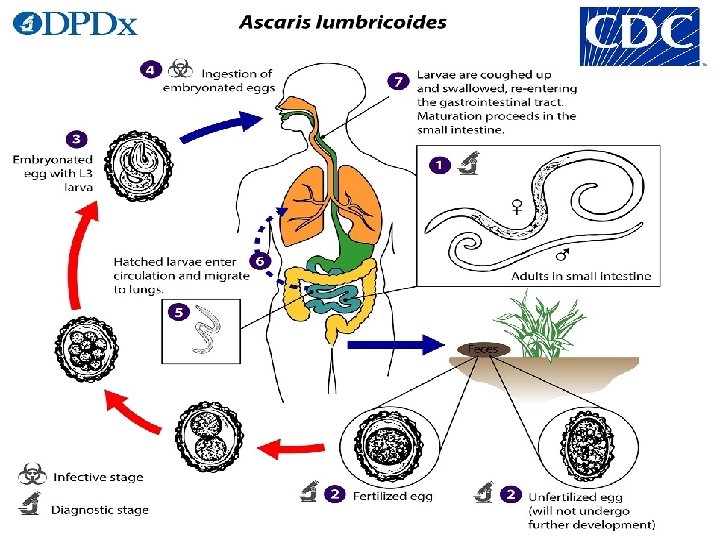
LIFE CYCLE

Stage I: Eggs in faeces Sexually mature female produces as many as 200, 000 eggs per day, which are shed along with faeces in unembryonated form. They are non infective. Stage II: Development in soil Embryonation occurs in soil as optimum temperature of 20 -25 C with sufficient moisture and O 2. Infective larva develops within egg in about 3 -6 weeks. Stage III: Human infection and liberation of larvae Human get infection with ingestion of embryonated egg contaminated food and water Within embryonated state inside egg, first stage larvae develops into second stage larvae. This second stage larvae is known as Rhabtitiform larvae Second stage larvae is stimulated to hatch out by the presence of alkaline p. H in small intestine and solubilization of its outer layer by bile.

Stage IV: migration of larvae through lungs Hatched out larvae penetrates the intestinal wall and carried to liver through portal circulation. It then travels via blood to heart and to lungs by pulmonary circulation within 4 -7 days of infection. The larvae in lungs molds twice, enlarge and breaks into alveoli.

Stage V: Re-entry to stomach and small intestine From alveoli, the Larvae then pass up through bronchi and into trachea and then swallowed. The larvae passes down the oesophagus to the stomach and reached into small intestine once again. Small intestine is the normal habitat of Ascaris and it colonises here. Within intestine parasite molds twice and mature into adult worm. Sexual maturation occurs with 6 -10 weeks and the mature female discharges its eggs in intestinal lumen and excreted along with faeces, continuing the life cycle. The life span of parasite is 12 -18 months

Pathogenesis Infection of A. lumbricoides in man is known as Ascariasis. There are two phase in ascariasis. Phase I: migrating larvae The migrating larvae causes pathological lesions. The severity of lesions depends upon the sensitivity of host, nutritional status of host and number of migrating larvae. During migration and molding through lungs, larvae may causes pneumonia with low grade fever, cough and other allergic symptoms.

Phase II: Adult worm Few worm in intestine produce no major symptoms and but some time give abdominal pain especially in children. The adult worm produce trauma in host tissue and the wandering adults may block the appendical lumen or common bile duct and even small intestine. Large number of adult worms affects the nutritional status of host by robbing the nutrition leading to malnutrition and growth retardation in children. The metabolites of living or dead worm are toxic and immunogenic. lumbricoides also produces various allergic toxin, which manifests fever, conjunctivitis and irritation.

Clinical manifestation: Most of the Ascaris infection is asymptomatic. Symptomatic ascariasis; two types: Intestinal Ascariasis Pulmonary Ascariasis 1. Intestinal ascariasis; Nausea Vomiting Colicky abdominal pain Abdominal distention Weight loss and diarrhea Malbasorption of nutrition Growth retardation Heavy worm in children leads to intussusception and total obstruction Complications: Appendicitis, Biliary colic and perforation of bile duct, Hepatomegaly 2. Pulmonary ascariasis; Transient eosinophilic pneumonitis (loeffler’s disease); elevated Ig. E Bronchospasm Dyspnea and wheezing Fever Non-productive cough and chest pain
 Demonstration of adult worm")
Laboratory diagnosis Done by following methods 1. Parasitic diagnosis a) Demonstration of adult worm b) Demonstration of eggs c) Demonstration of larvae 2. Serodiagnosis 3. Eosinophilia and Ultrasonography and CT scan

Demonstration of adult worms Worm may be passed through anus, mouth, nose and rarely through ear Barium meal may occasionally reveal the presence of adult worms in the small intestine Demonstration of eggs Eggs may be detected in stool or duodenal bile aspirate by direct microscopy or after concentration of faeces Eggs may not be seen if only male worms are present

Demonstraion of larvae Ascaris larvae may be detected in the sputum during the stage of migration 2. Serodiagnosis Ascaris antibody can be detected by indirect haemagglutination (IHA) And immunofluorescence antibody (IFA)test These tests are useful for the diagnosis of extraintestinal – ascariasis like Loeffler’s syndrome 3. Eosinophilia It is seen in larval invasionstage

Treatment • Pyrantel pamoate, in a single dose of 11 mg per kilogram body weight (maximum 1 gm) • Mebendazole in a dose of 100 mg twice daily for 3 days, and piperazine citrate in a dose of 75 mg per kg body weight daily for 2 days

PREVENTION • Keeping good sanitation conditions is the only way to prevent the infection of Ascaris. • Pollution of soil with human faeces should be avoided. • Vegetable should be thoroughly washed in a mild solution of Pottasium permanganate and properly cooked before use. • Finger nails should be regularly cut to avoid the collection of dirt and eggs below them. • Hands should be properly washed with some antiseptic soap before touching edibles or eating.

Prophylaxis Ascariasis can be prevented by • Proper disposal of human faeces • Avoidance of eating raw vegetables and salads • Periodic treatment with an effective anthelminthic, in communities that lack sanitary facilities

Larva Migrans • This is a term used to describe human infections with helminth larvae, which are not adapted to human beings • The condition is usually caused by animal parasites, man being an abnormal host, these larvae are not able to reach the normal habitat and keep wandering in the abnormal host (man), hence, known as larva migrans
 Cutaneous larva migrans (CLM) also known as creeping eruption")
Divided into 2 types 1) Cutaneous larva migrans (CLM) also known as creeping eruption 2) Visceral larva migrans (VLM)

Common points between CLM and VLM • Man always acquires the infection as an accidental host • The causative agents are usually zoophilic helminths • The host mounts an inflammatory response directed against somatic antigens of parasites • Both diseases affect primarily the children • Both are widespread in tropical and temperate countries of the world
- Slides: 31