Role of Osteotomy in ACL and PCL Deficient






")

































: 376 -82. • Ten")

: 961 -7. • 10")
: 9 -16 • 26 Patients")
: 431 -7 29 patients (30")



: 185 -93. •")
- Slides: 51
Role of Osteotomy in ACL and PCL Deficient Patients Satyam Patel Feb. 2007 mod. from Cole Beavis Nov. 2002
Outline • Natural history of ACL and PCL deficient patients • Principles of osteotomy in management of knee instability and malalignment • Management of combined knee instability and malalignment • Not discussed / deferred to future talk : role of osteotomies in management of
Natural History of ACL/PCL Deficient Knee • Literature somewhat difficult to interpret – Variety of factors influence natural history • • Meniscal tears Chondral damage from original injury Heterogeneous population (grades I-III) Types of conservative treatments – Outcome measures often difficult to measure • “return to sport” • “return to previous function”
Natural History of ACL Deficient Knee • Generally agreed upon principles – Gait altered • “quadriceps avoidance” – Repeated episodes of subluxation • Meniscal and chondral damage – Degenerative changes present in most patients within 6 -10 years of injury • Worst in subset of patients with meniscal injury • Medial compartment > lateral compartment
Natural History of ACL Deficient Knee • Dejour - from Fu Knee Surgery “…osteophyte and superficial destruction of cartilage are likely to develop within 10 years in knees with ACL rupture. Significant arthrosis develops after longer periods (20 -30 years). An additional meniscal lesion or meniscectomy constitutes a turning point in the evolution of arthrosis. The meniscal factor is not the main factor; it is a contributory factor in the evolution of arthrosis in the ACL deficient
Natural History of PCL Deficient Knee • Commonly reported in the literature that the natural history of isolated PCL deficiency is benign • Controversial • Cadaveric and clinical studies have shown high incidence of patellofemoral joint and medial compartment arthrosis
Natural History of PCL Deficient Knee • Miller, Bergfeld, Fowler, Harner, Noyes (ICL 99) “…degenerative change is probably inevitable, and that current surgical techniques cannot forestall it. PCL injuries may not be as benign as we previously thought, especially with advanced (grade 3) injuries. ”
Principles of Tibial Osteotomy
Principles of Tibial Osteotomy • Coventry – established high tibial osteotomy as a treatment for unicompartmental OA • Goal of osteotomy – to transfer joint forces from the arthritic compartment to the more normal compartment
Principles of Tibial Osteotomy • Mechanical axis • line drawn from the center of hip rotation through the center of the knee to the center of the ankle mortise • a normal axis is a straight line • Anatomic axis (tibiofemoral angle) • obtained by the intersection of the lines drawn along the shaft of the femur and tibia • normally 5 -7 degrees of valgus
Principles of Tibial Osteotomy • Anatomic – Comparison of femoral and tibial shafts – 5 - 7º valgus • Mechanical – Line of ground reaction force transmission – 0 - 1º varus
Principles of Tibial Osteotomy • Mechanical Axis – Location determines percentage of load carried in each compartment – In the normal knee 60% of weight bearing is through the medial compartment
Principles of Tibial Osteotomy • Type of osteotomy – Medial compartment OA with varus deformity • valgus-producing osteotomy – Lateral compartment OA with valgus deformity • varus-producing osteotomy – Alteration in tibial slope for ligamentous deficiency • Extension type for ACL deficient
Principles of Tibial Osteotomy • Type of osteotomy Extension Valgus
Principles of Valgus Tibial Osteotomy • Indications for valgus osteotomy – pain unresponsive to conservative measures – isolated medial compartment OA – age < 60 – no more than 10 -15 of varus on WB film – pre-op ROM > 90 – <15 of flexion contracture
Principles of Valgus Tibial Osteotomy • Contraindications: – – – – – narrowing of the lateral compartment lateral tibial subluxation > 1 cm flexion contracture > 15 degrees ROM < 90 degrees > 20 degrees of correction needed large varus thrust inflammatory arthritis tricompartmental arthritis severe patellofemoral disease
Principles of Valgus Tibial Osteotomy • Aim for mechanical axis to pass through medial 1/3 of lateral compartment • Determine amount of correction – Multiple recommendations for post-op valgus anatomic alignment • • Fu Vainionppa Insall Keene 5 - 13º > 7º 10º 7 - 13º – Most common reason for failure of osteotomy is undercorrection
Principles of Tibial Osteotomy • Technique – Preop plan with long leg weight bearing xrays – Calculate size of wedge using bone width and trigonometry – Traditionally, 1 mm for 1º correction • Only valid for a
Principles of Tibial Osteotomy • Level of Tibial Osteotomy – Above the tubercle (most common) • High healing rates • Limited degree of correction – Below the tubercle • Greater range of correction • More bone proximally for fixation • Lower healing rates
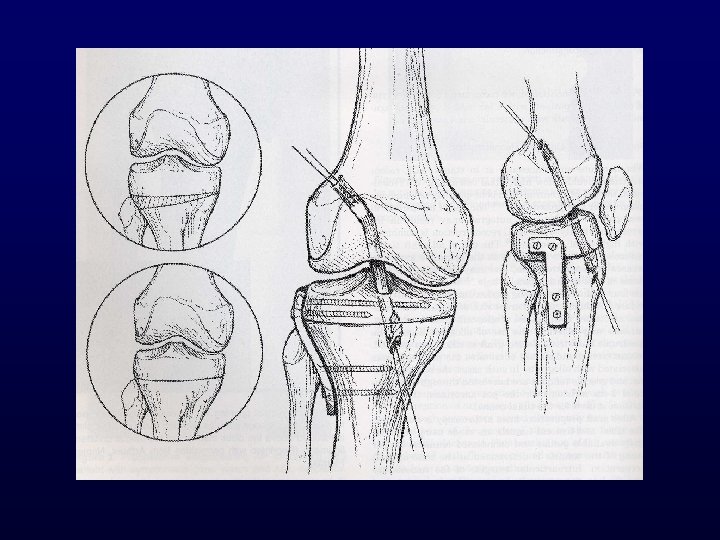
Valgus Closing Wedge
Valgus Closing Wedge • Lateral wedge resection • Hinge on medial cortex • Can resect more bone anteriorly to decrease tibial slope (extension type osteotomy) – ACL deficiency
Valgus Closing Wedge • Benefits – – – Can compress across osteotomy Quadriceps pull compresses osteotomy No bone graft harvest site No risk of bone graft shifting Inherently more stable • Drawbacks – Shortens quads mechanism and leg – Infrapatellar scarring – Can unmask MCL laxity
Valgus Opening Wedge
Valgus Opening Wedge • Medially based wedge • Multiple variations in techniques • Can incorporate anterior opening wedge – Increases tibial slope (PCL deficiency)
Valgus Opening Wedge • Advantages – Useful with medial bone loss or MCL laxity – Tensions MCL • Drawbacks – Limited compression – Bone graft donor site morbidity
Fixation of Osteotomies • Cast • Staples • Plate – Compression, buttress • External fixator
Osteotomies and ACL / PCL Deficient Knees
Osteotomy and ACL Deficient Knees • Valgus osteotomy described in treatment of unicompartmental arthrosis associated with ACL deficiency – Shift mechanical axis laterally and decrease force through diseased medial compartment
Osteotomy and ACL Deficient Knees • Osteotomy has been used in treatment of instability – Extension type to decrease tibial slope and anterior tibial translation
Osteotomy and ACL Deficient Knees • Osteotomy has been used in treatment of instability – Extension type to decrease tibial slope and anterior tibial translation
Osteotomy and ACL Deficient Knees • Approach – Patients with arthritic, ACL deficient knee and failing conservative treatment • 3 groups of patients 1. Primary symptom is instability 2. Primary symptom is pain 3. Both pain and instability
Osteotomy and ACL Deficient Knees • Primarily instability Pain + Malalignment - ACL Reconstruction Pain - Malalignment + Reconstruction Pain - Malalignment Pain + Malalignment + Reconstruction Osteotomy and ACL Reconstruction Osteotomy and
Osteotomy and ACL Deficient Knees • Primarily pain Instability + Reconstruction Instability debridement Instability + Reconstruction Malalignment - ACL Malalignment + Malalignment - Osteotomy ? Arthroscopic Malalignment + Osteotomy and
Osteotomy and ACL Deficient Knees • Technique – Preoperative planning aiming for 8 -10° of valgus – Initial arthroscopy • Assess articular surfaces • Address meniscal pathology – High tibial osteotomy • Lateral closing wedge for most • Medial opening wedge for MCL laxity • Ensure fixation does not cross region of future tunnels
Osteotomy and ACL Deficient Knees • Technique con’t – ACL reconstruction follows osteotomy • Staged or as part of same procedure • Bone patellar tendon bone, hamstring and allograft have all been reported – Increased risk of patella baja with BTB
Osteotomy and ACL Deficient Knees • Technique contd – Postop combined procedure • CPM immediately postop • Hinge brace locked in extension x 4 weeks; touch WB • Brace unlocked and WB progressed from 4 -8 weeks • At 8 weeks postop brace discontinued and aggressive ACL rehab program x 3 -6 months – Staged • ACL follows 6 months after osteotomy • Osteotomy hardware removed at time of ACL
Osteotomy and ACL Deficient Knees • Outcomes – Return to pre-injury level is rare • Few reports of patients returning jumping, pivoting sports – Those with severe pain should expect improvement • 80 -92% patient satisfaction – Maximal benefit obtained in patients wishing to return to light athletic activities • 30 -78% return to sports
Osteotomy and PCL Deficient Knees • Few reports in literature – Similar indications as for ACL with symptomatic varus malalignment and unicompartmental disease • PCL deficiency medial and patellofemoral arthrosis – Must select patients carefully – Also described as treatment of posterolateral instability with varus thrust in absence of arthrosis • Correct mechanical axis prior to ligament
Osteotomy and PCL Deficient Knees • Increasing tibial slope has been shown to decrease tibial translation (sag) – Anterior opening wedge osteotomy – Anteromedial opening wedge to address tibial slope and varus malalignment
Osteotomy and PCL Deficient Knees • Increasing slope by 50% resulted in shift of resting position of knee between 3 -5 mm (reduced posterior sag) • Few reports and no long term results for this technique – Additional studies required
Biomechanical studies • Am J Sports Med. 2004 Mar; 32(2): 376 -82. • Ten cadaveric knees were studied using a robotic testing system using three loading conditions: – (1) 200 N axial compression – (2) 134 N A-P tibial load – (3) combined 200 N axial and 134 N A-P loads • Tibial slope was increased from 8. 8 +/- 1. 8 deg. to 13. 2 +/2. 1 degrees, – anterior shift of tibia relative to femur (3. 6 +/- 1. 4 mm). – Under axial compression, the osteotomy caused a significant anterior tibial translation up to 1. 9 +/- 2. 5 mm (90 degrees ). – Under A-P and combined loads, no differences were detected in AP translation or in situ forces in the cruciates (intact versus
Biomechanical studies • Results suggest that small increases in tibial slope do not affect A-P translations or in situ forces in the cruciate ligaments. • However, increasing slope causes an anterior shift in tibial resting position that is accentuated under axial loads. • This suggests that increasing tibial slope may be beneficial in reducing tibial sag in a PCLdeficient knee, whereas decreasing slope may be protective in an ACL-deficient knee.
Biomechanical studies • Am J Sports Med. 2006 Jun; 34(6): 961 -7. • 10 cadaveric knees: valgus HTO + anatomic double bundle ACL reconstruction • Anterior tibial translation and internal rotation decreased by 2 mm and 2 degrees at low flexion angles vs. ACL intact knees • In-situ forces in posterolateral graft became 56 -200% higher than those in the posterolateral bundle of the intact ACL • N. B. - may overconstrain knee and result in high
Clinical studies • J Knee Surg. 2003 Jan; 16(1): 9 -16 • 26 Patients with ACL insufficiency, symptomatic medial OA, varus – 14/26 recreational athletes - minimum 2 year follow-up • 12 valgus HTO alone ACLR • No change in instability 11/13 • No ROM deficit vs. 14 valgus HTO + vs. grade 1 lachman negative pivot 12/13 same
Clinical studies • • • Knee 2004 Dec; 11(6): 431 -7 29 patients (30 knees) retrospectively reviewed Previous single-stage ACLR + valgus HTO 19/30 had previous medial meniscectomy 2/30 major complications --> stiffness 12 yr f/u (6 -16) – – 5/30 had progressed one arthritis grade 14/30 returned to intensive sports 11/30 played moderate sports Avg. difference in anterior tibial translation (vs. Normal side) was 3 mm
Osteotomy and ACL Deficient Knees • Summary – Active patients with ACL deficiency and unicompartmental arthritis may benefit from ACL reconstruction, osteotomy or combination with improved pain and return to recreational activities – Radiographic (& clinical) progression of OA may be delayed or may be unchanged.
Osteotomy and PCL deficient knees • Long-term data regarding the outcome of PCL deficiency vs. PCL reconstruction & osteotomy is lacking. • Short term follow-up reveals better knee scores and less subjective sense of instability. Am J Sports Med 1996; 24: 415 -426 • In the presence of varus deformity and decreased tibial slope correcting the varus deformity and increasing the tibial slope (e. g. anteromedial opening wedge) decreases the amount of posterior tibial sag. • This should theoretically decrease the amount of quads force required to pull tibia anteriorly and thereby decrease
References • Dejour et al, ACL reconstruction combined with valgus tibial osteotomy. Clin Ortho 1994 299: 220 -228 • De. Lee JC ed. Orthopaedic Sports Medicine. Pg 1401 -1441 • Fu F ed. Knee Surgery. Pg 859 -876 • Larson et al, PCl reconstruction: associated extra-articular procedures. Tech Ortho 2001 16(2): 148 -156 • Noyes et al, High tibial osteotomy in ligament reconstruction for varus angulated ACL deficient knees. Am J Sports Med 2000 28(3): 282 -296 • O’Neil and James, Valgus osteotomy with ACL laxity. Clin Ortho 1992 278: 153 -9 • Vogrin et al, Biomechanics of PCL deficient knee. Tech Ortho 2001 16(2): 109 -118 • Williams et al, Management of unicompartmental arthritis in the ACL deficient knee. Am J Sports Med 2000 28(5); 749 -760
Clinical studies • Z Orthop Ihre Grenzgeb. 2002 Mar. Apr; 140(2): 185 -93. • Simultaneous arthroscopic cruciate reconstruction and closing wedge osteotomy – – – 4/96 - 12/00 58 patients (avg. 33 y. o. ) 49 ACL , 7 PCL, 2 ACL & PCL Avg. 7 deg correction (mean malalignment 5 deg) 13 patients also had osteochondral allograft 2 had implantable collagen meniscus Lysholm score (66 --> 81 --> 87 --> 93)