Role of Atherectomy Devices in Peripheral Vascular Procedures





")






























 and up")

















- Slides: 68
Role of Atherectomy Devices in Peripheral Vascular Procedures D. Chris Metzger MD, FACC, FSCAI Wellmont CVA Heart Institute Kingsport, TN, USA
D. Christopher Metzger, MD Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Affiliation/Financial Relationship Company • Consulting: • Hands- On PV and CAS Courses: • National Co-PI: • CEC Committee • Abbott, Cordis, IDEV, Medtronic • Abbott, Pathway, Medtronic • SAPPHIRE WW CAS (Cordis) • Covidien(DEFINITIVE)
Potential Arguments Against Atherectomy Device Use • • • Increased Cost Increased Procedural Time (? ) Increased contrast Larger Sheaths Distal Embolization No clear cut evidence of benefit compared to more conventional therapy (RCT’s)
Existing “p Values” & Basic Principals ♥ The primary patency for lesions treated with POBA @ 1 yr is ~ 33%; P = Pretty bad! ♥ Primary patency for long SFA lesions with contemporary stenting @ 1 year is 55%-58% (VIBRANT interim data) ♥ Stent fracture rates for long lesions is potentially high (up to 40%!); P= Pretty scary ♥ FDA-approved SFA stents: Intracoil, Viabahn, Lifestream ♥ Bare metal stents and POBA have high restenosis rates for infrapopliteal interventions; DES are “off label”
Atherectomy: Some “p Values”/ Facts – All 4 major atherectomy devices DO have multi-center , adjudicated trial data – All 4 atherectomy devices ARE FDAapproved and “on label” for PV intervention – Atherectomy data @ 6 -12 months compares well w/ POBA & stenting published results – Many PV devices are widely accepted without randomized data (e. g. embolic protection devices in CAS)
Potential Advantages of Atherectomy – – – – Avoid long stent lengths (and fractures) Potentially less dissection, esp. in “no stent zones” Preserves options for future interventions Plaque modification: → stent delivery/apposition “Deals with” calcium, thrombus, etc. Assists in challenging infrapopliteal anatomy Allows treatment of challenging cases which otherwise may be undoable – Can be coupled with embolic protection (& DCBs? )
So When and Where Do I Use Atherectomy Devices? Selectively, when: The advantages of the device offer improvements in outcome compared with stenting ♥ Nondilatable lesions ♥ “No stent zones” ♥ Heavy calcium ♥ Thrombotic lesions ♥ Long bulky disease ♥ Otherwise “undoable” lesions ♥ Infrapopliteal long lesions
The Increasingly Complex Disease We Treat….
… Sometimes Calls for More Tools
Proper Technique is Essential! • Devices will perform poorly if used incorrectly OR in the wrong patients or lesions • In general, SLOW advancement of devices • Devices work better in the true lumen (CTO’s) • Sizing of device and “speeds” (rotational, “blades up”, rates, fluence, etc. ) • Need experience from others during learning curve • CASE SELECTION !!
Embolic Protection Use • I have ~low threshold for EPD use: use if lesion has embolic risk OR if BTK disease • Spider recent FDA approval, rest “off label” • I prefer independent wire EPD (NAV 6) with XC length wire- ↓basket movement • CSI- can use 0. 017 tip Viper wire w NAV 6
CSI Orbital Atherectomy • Most useful for heavy, relatively focal calcified femoro-popliteal or BTK Ca++ dz • Does have risk of distal embolization, especially when used w long disease • If use EPD (“off label”), use Viper wire (0. 017 tip) in combination with NAV 6
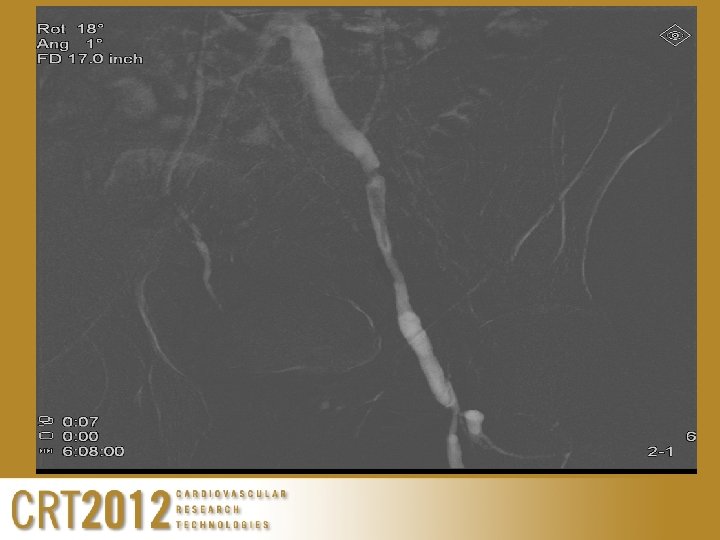
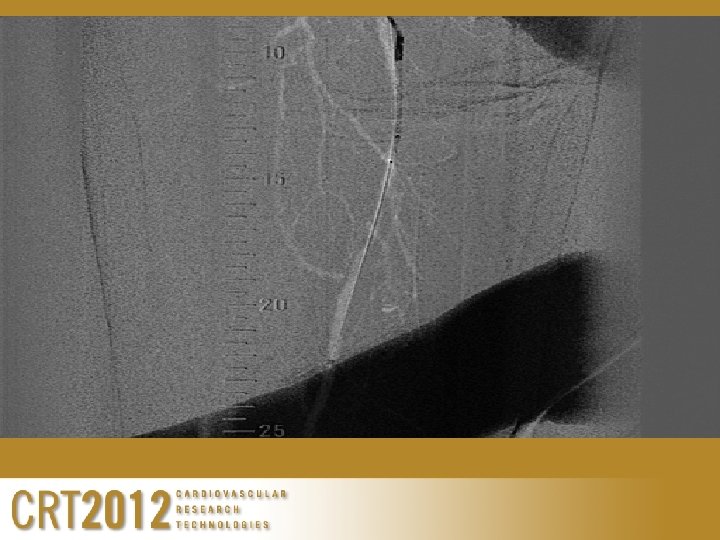
Calcified L SFA disease
Calcified “Non-dilatable” Bifurcation
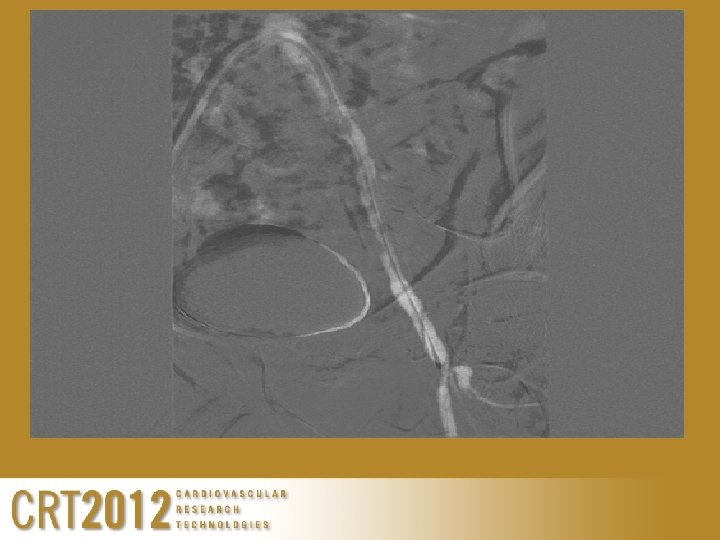
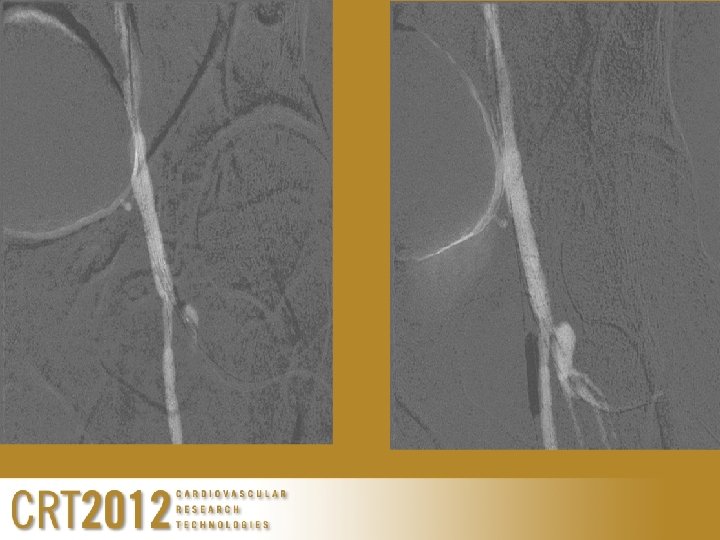
1. 75, 2. 25 crowns SFA
1. 75, 2. 25 crowns PFA
Pathway Jetstream Atherectomy • Probably most versatile, works well with thrombus AND up to heavy calcium • Incorporates active aspiration w/ atherectomy • Newer devices available for BTK vessels, although caution needed
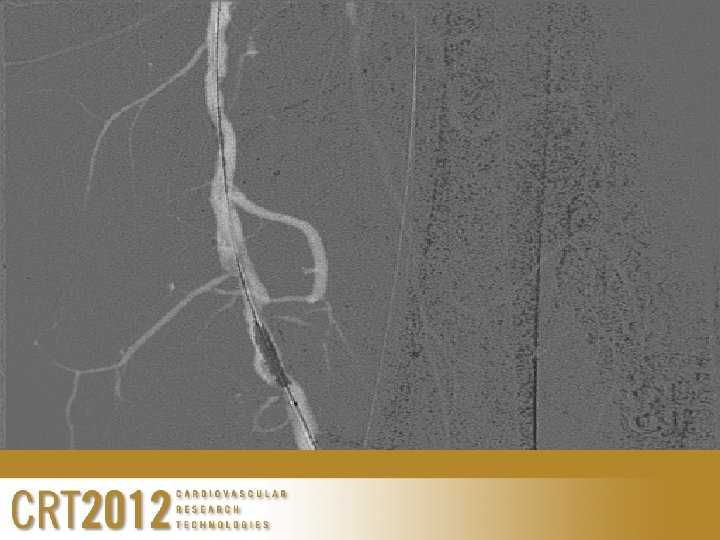
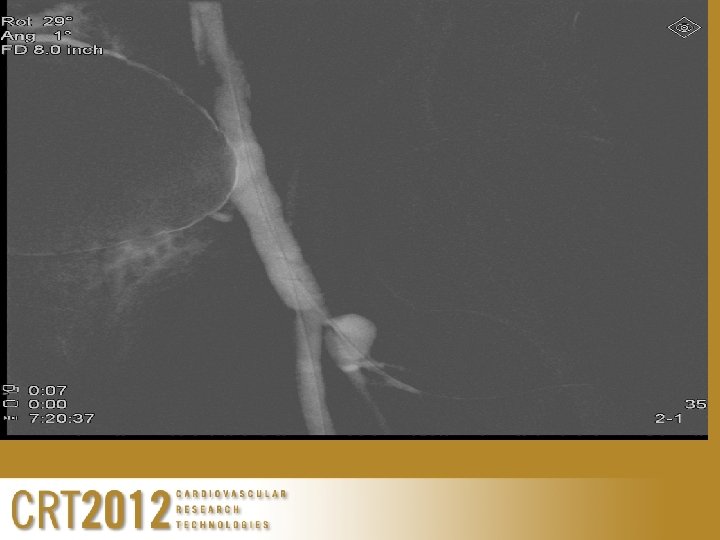
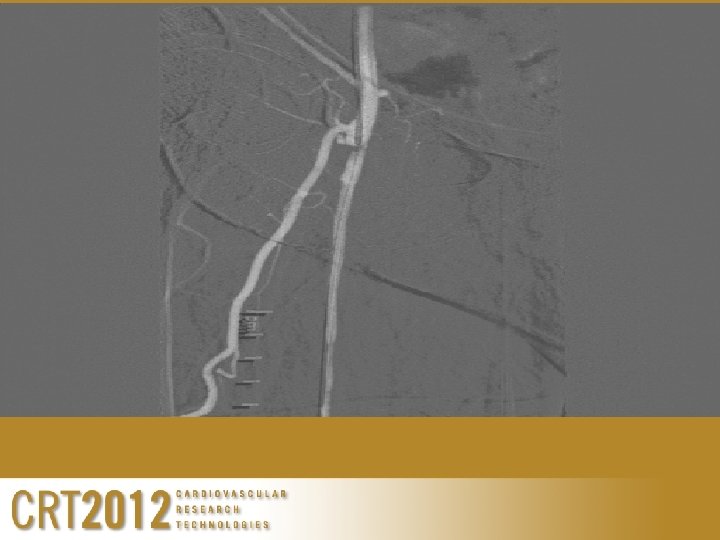
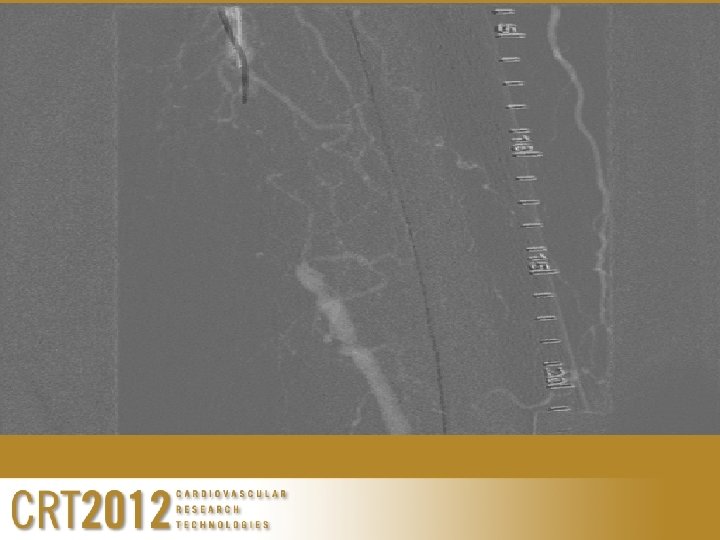
Pathway-Acute L leg after 2 yr claudication
Pathway -severe CFA & SFA ISR
Laser Advantages/ Disadvantages • Works very well for thrombus (new and old) and up to moderate calcium-versatile • Can do long runs, multiple sizes available, devices small enough to go into foot • ~Good for ISR with Turbo tandem (“off label”); relatively low embolization rates • Excellent for crossing recalcitrant CTO’s • Disadvantages: Not good for heavy Ca++, requires console
Laser Turbo Tandem ISR/CTO
Laser Step by Step for CTO’s
Silver. Hawk Advantages/ Disadvantages • Effective plaque excision, may offer most effective debulking • Potential “stand-alone” results CFA & pop • Well- studied, studies ongoing • No console • Works for ISR carefully (off-label!) • Disadvantages: Not effective for thrombus, previously not for heavy Ca++, frequent device removals, embolization; highly recommend EPD
More Silver Hawk
CONCLUSIONS • Selective use of atherectomy devices may offer advantages when the benefit of the device use justifies the cost of the device • Experience with proper use of adjunctive PVI devices may increase the number of patients we can treat effectively with endovascular therapy • Device selection is individualized • Future trials in combination with DCB’s may lead to an expanded role
Thank You for Your Attention!