ROBOTASSISTED LAPAROSCOPIC SURGERY WITH ZEUS SYSTEM PRELIMINARY RESULTS

ROBOT-ASSISTED LAPAROSCOPIC SURGERY WITH ZEUS SYSTEM : PRELIMINARY RESULTS AND TECHNICAL ASPECTS Hurng-Sheng Wu Department of Surgery, Show-Chwan Memorial Hospital, Changhua, Taiwan, R. O. C



Difficulties of laparoscopic surgery Unstable camera platform Loss of degrees of freedom Two-dimentional imaging Poor ergonomics for the surgeon Ballantyne G. H. Surgical laparoscopy, endoscopy Percutaneous techniques Vol. 12, No. 1, pp. 1 -5, 2002



Decades of Changes in Surgical Education <1950 1960 1970 1980 1990 2000 Operating room theaters Experimental surgery and motion picture films Industry-research laboratories Endoscopic surgery Laparoscopy Robotics Alberto Peracchia, Annals of Surgery Vol. 234, No. 6, 709 -712, 2001

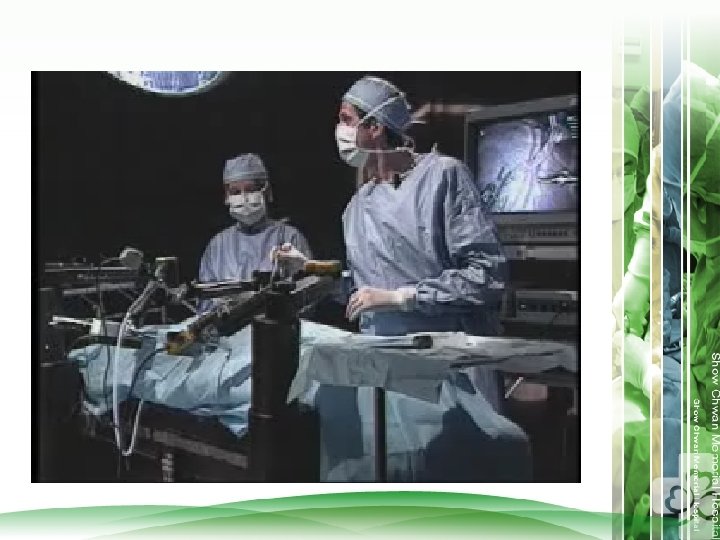
Space Medicine ZEUS da Vinci Master-slave manipulator Simplicity Lightness Range of freedom Motion scaling Real-time high-resolution 3 D vision Physiological tremor elimination


The key component of the Zeus Surgical System is the microwrist technology. It allows the surgeon to roll, pitch, yaw and grip laparoscopic tools. It also provideds a real benefit for the surgeon with a 3 -D view of the operative field. Microwrist

What is about space medicine?

ROBOT: computer-enhanced humanistic device

Zeus Robotic System AESOP HERMIS SOCRATES Surgeon Console& Three Roboyic Arms


LIMITATIONS OF ROBOTIC SURGERY Ports and/or robotic arms placement eg: lithotomy position Cosmetic Depth perception No haptic feed back eg: needle and suture breaks Size Set up

Robotic Surgery in Show Chwan Memorial Hospital BETWEEN MARCH, 2002 AND NOVEMBER, 2004 Dept. General Surgery Cardiovascular Surgery Obstetrics & Gynecology Operation Total Robotic assisted Nissen fundoplication 4 Robotic assisted gastric band for obesity Robotic assisted laparoscopic cholecystectomy Robotic assisted repair of PPU Robotic assisted Choledocholithotomy with T-tube Robotic assisted laparoscopic appendectomy Robotic assisted laparoscopic adrenectomy Robotic assisted oophorectomy 3 71 3 28 1 3 1 Robotic assisted laparoscopic unroofing of intraabdominal cyst Total Zeus IMA take down 2 Robotic ACAB 3 6 Robotic assisted salpino-oophrectomy 2

Endo-ACAB Definition : A less invasive bypass procedure on the beating heart where all steps are performed endoscopically with the exception of a manual anastomosis.

Technique of Endo-ACAB Endoscopic IMA Harvest voice-activated robotic-assisted and a 5 mm thoracoscope under single lung ventilation and CO 2 insufflation


Technique of Endo-ACAB Atrumatic Thoracotomy

Technique of Endo-ACAB Direct vision anastomosis

Robotic-Assisted Laparoscopic Surgery in Difficult Common Bile Duct Stone: Preliminary Results in Show Chwan Memorial Hospital Hurng-Sheng Wu Department of Surgery, Show Chwan Memorial Hospital, Changhua. Taiwan
 in patients with")
Background Common bile duct stones are a frequent problem (10 -15%) in patients with symptomatic cholecystolithiasis Laparoscopic techniques have expanded the options for their treatment Difficulty in laparoscopic surgery

Aims Compare the results in patients with CBD stones by Laparoscopic to robotic-assisted CBD exploration

Patients Between January 2000 and November 2003 919 patients with GB stones and/or CBD stone 772 patients(84%) – LC (including 55 robotic-assisted ) 55 patients(6% )- Open Cholecystectomies 92 patients(10%) with CBD stone IHS excluded 42 patients(45%) – open CBDE 22 patients(24%) – LCBDE 28 patients(31%) – Robotic-assisted
 (n=28) Big stone (>1")
Criteria of difficult common bile duct stone LCBDE Robotic-Assisted (n=25) (n=28) Big stone (>1 cm) 9 10 multiple stones 10 2 4 9 4 5 2 1 2 25 1 28 Impacted CBD stone ERC failed s/p Billroth II resection duodenal diverticulum uncooperative behavior Intolerance Total

Mr. Ker. 43/yrs male C. C. : RUQ pain tea-color urine Lab. : GPT: 65 Alk-P: 368

 Variables LCBDE Robotic-Assisted P value No. of patients 22 28 No. (%) of")
Results(1) Variables LCBDE Robotic-Assisted P value No. of patients 22 28 No. (%) of conversion 3 (12%) 3(10%) NP Mean age( years old) 58 (range 23~83) 59 (range 41 -84) NP Sex= M : F 8: 14 11: 14 NP ≦ 2 (mg/dl) 13 7 0. 031 2 ~ 10 (mg/dl) 9 18 Mean caliber of CBD (cm) 1. 43 (range 0. 8~2. 2) 1. 6 (range 1. 2~2. 5) NP No. (%) of complication 2 (9%) 2 (8%) NP No. (%) of retained stone 2 (9%) 2 (8%) NP No. of recurrent stone 1 0 NP Follow-up( months ) 3~39 1 -20 Total Bilirubin level
 LCBDE Robotic-Assisted P CBD diameter (cm) 1. 45± 0. 36 (17.")
Result (2 ) LCBDE Robotic-Assisted P CBD diameter (cm) 1. 45± 0. 36 (17. 2) 1. 6± 0. 3 (1. 2 -2. 5) NP Suture stitches 2. 05± 0. 56(1 -3) 3. 84± 0. 90(3 -6) <0. 001 Time to liquid (days) 2. 55± 0. 78 (2 -5) 2. 32± 0. 97 (1 -4) NP 6. 6± 0. 36 (4 -11) NP Postoperative hospital stay (days) 6. 8± 3. 1 (5 -14)

 Mortality Conversion to open LCBDE Robotic-Assisted 0 0 3 Conversion to LCBDE")
Result (3) Mortality Conversion to open LCBDE Robotic-Assisted 0 0 3 Conversion to LCBDE Complications: Acute hepatitis 0 1 Wound infection 1 1 Bile leakage Retained stone(s) T-tube Dislodge 2 2 1 0 2 0
 Person Robot Set time (min) Person Robot Suture Time")
(min) Person Robot Set time (min) Person Robot Suture Time

OP TIME & Learning Curve Time Person
 LCBDE suture=24. 65± 10. 82 min")
ZEUS suture=37. 76± 24. 33 min (stitches=3. 84) LCBDE suture=24. 65± 10. 82 min (stitches=2. 05)

THE FUTURE OF ROBOTIC SURGERY


CIMIT Center for Integration of Medicine and Innovative Technology Founding Members: CIMIT facility in Cambridge, Massachusetts

- Slides: 42