Rickets What are Rickets Disease of growing bones

Rickets

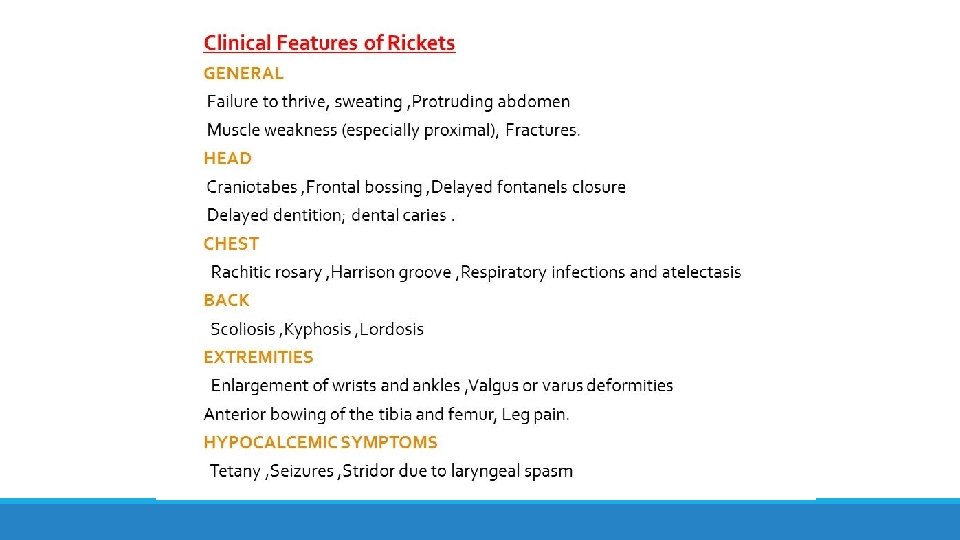
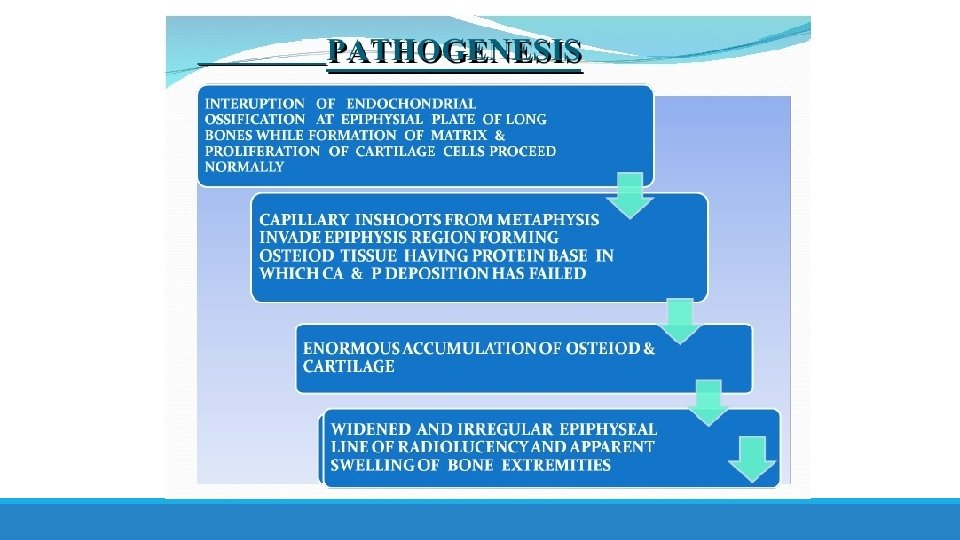
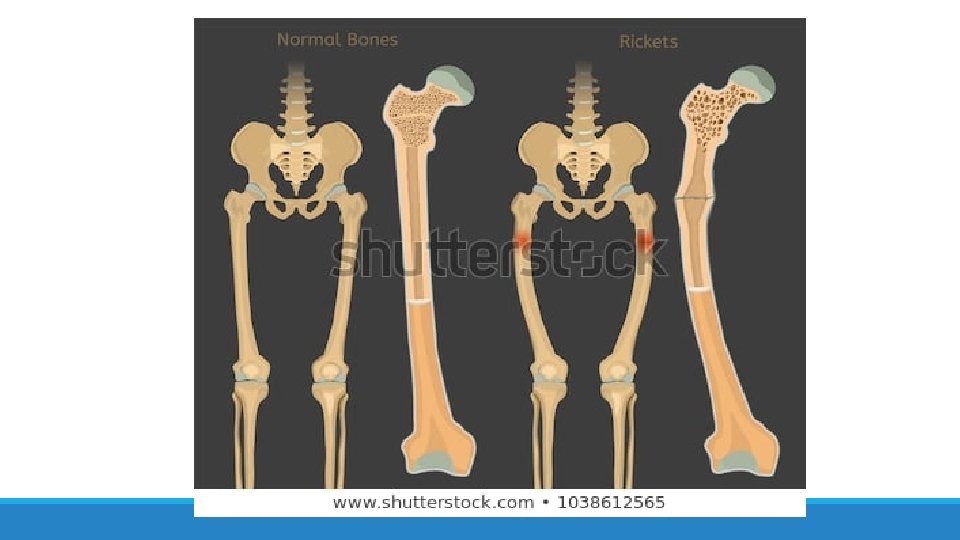
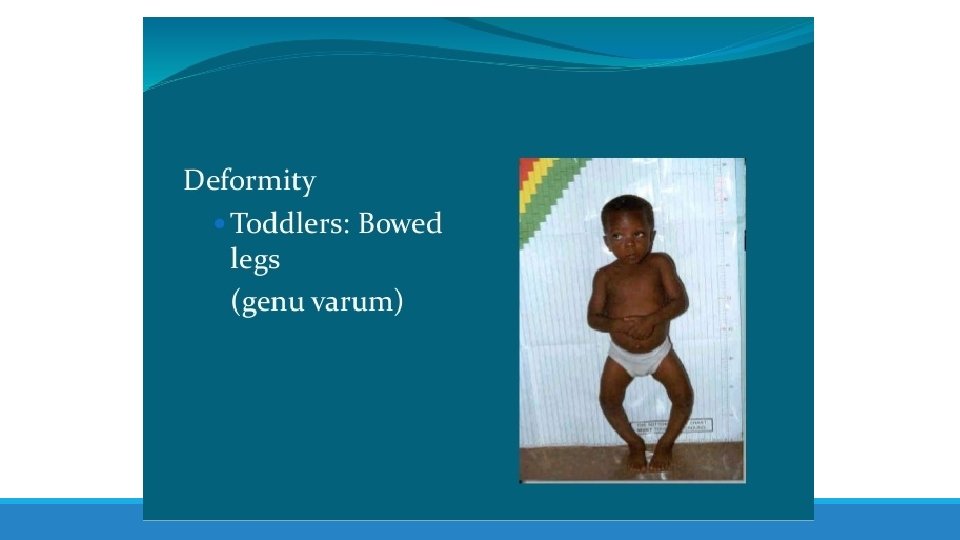
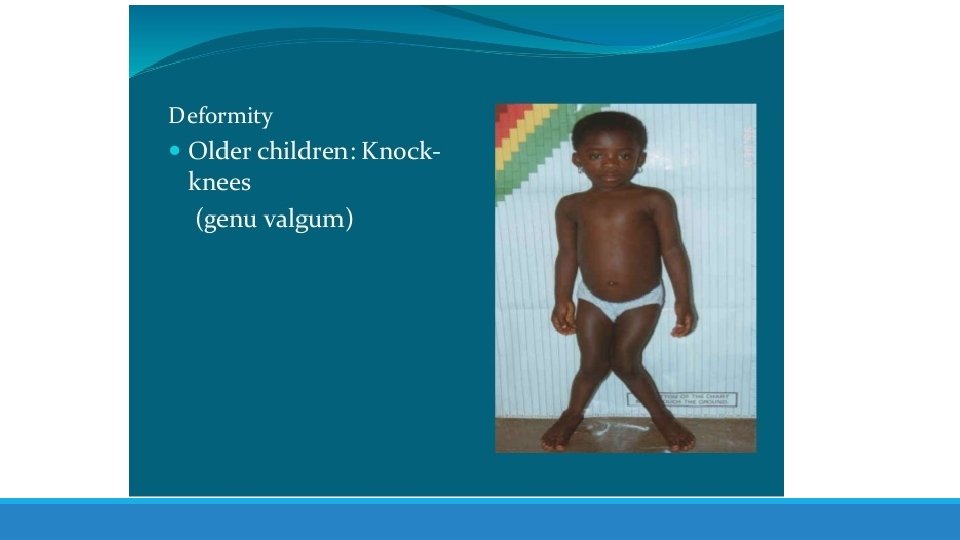
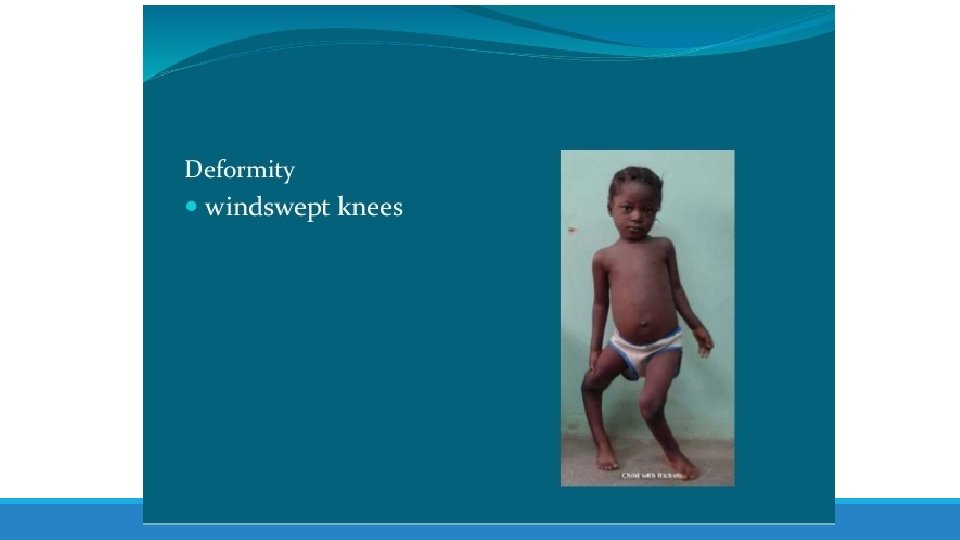
What are Rickets Disease of growing bones in which defective mineralization occurs in both bone and cartilage of epiphyseal growth plate, associated with: – Growth retardation – Skeletal deformities

“English disease” is another name of the rickets ØThe term rickets is likely derived from the Old English wrickken, meaning to twist. ØThe term has also been associated with the Greek rachitis, referring to the spine ØEarly reports of bone deformities resembling rickets are attributed to physicians Soranus and Galen from the first and second centuries AD ØThe first detailed description was published by Glisson et al in a medical treatise from England in 1650 ØAn earlier brief monograph on rickets published in 1645 identified delayed tooth eruption associated with rachitic skeletal disease ØBetween 1918 and 1928, scientists determined that rickets was caused by a deficiency in an “anti-rachitic substance, ” and eventually named this substance Vitamin D.

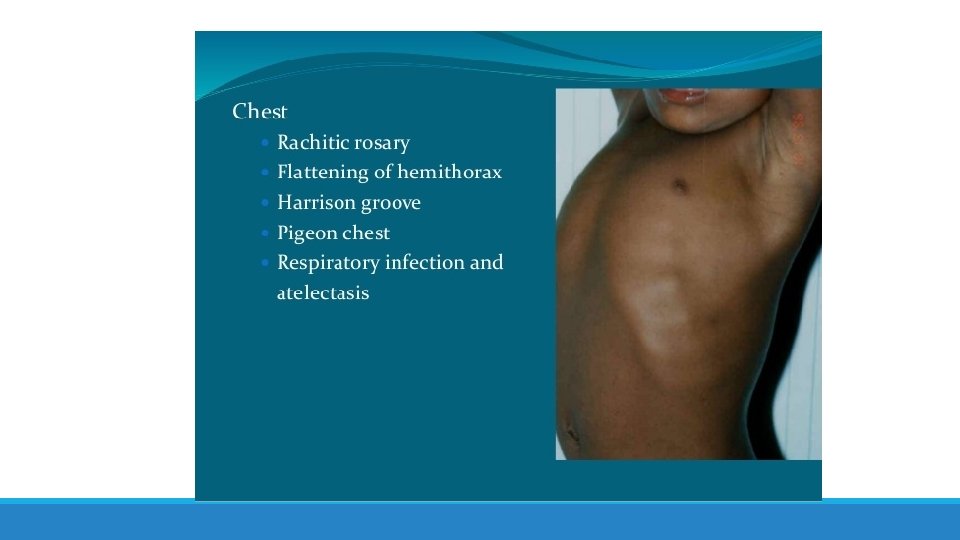
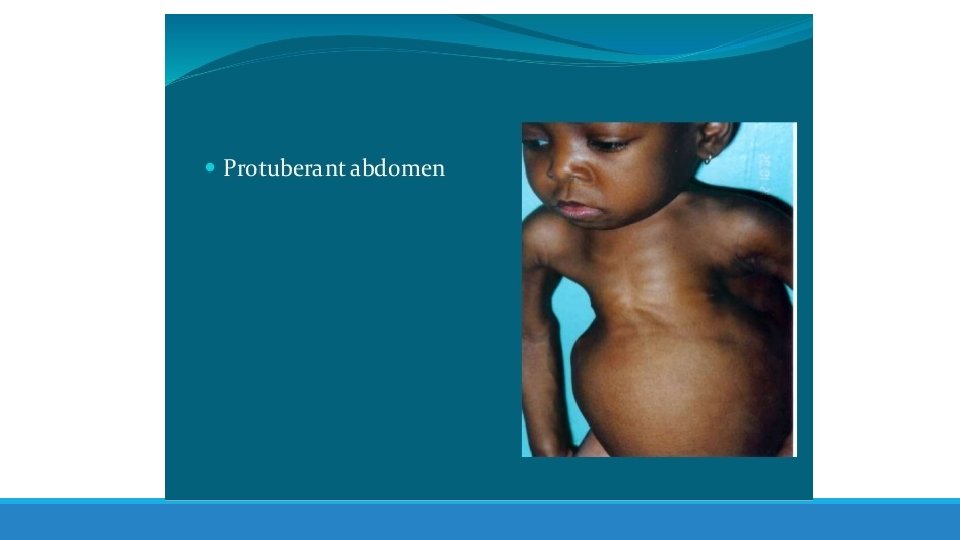
Michelangelo Merisi da Caravaggio Bagnacavallo Madonna oil painting by Albrecht Dürer • • • Olympian forehead (protruding forehead ) Protruding abdomen Enlarged epiphysis of wrist and ankle Curved radius and ulna Harrison’s groove

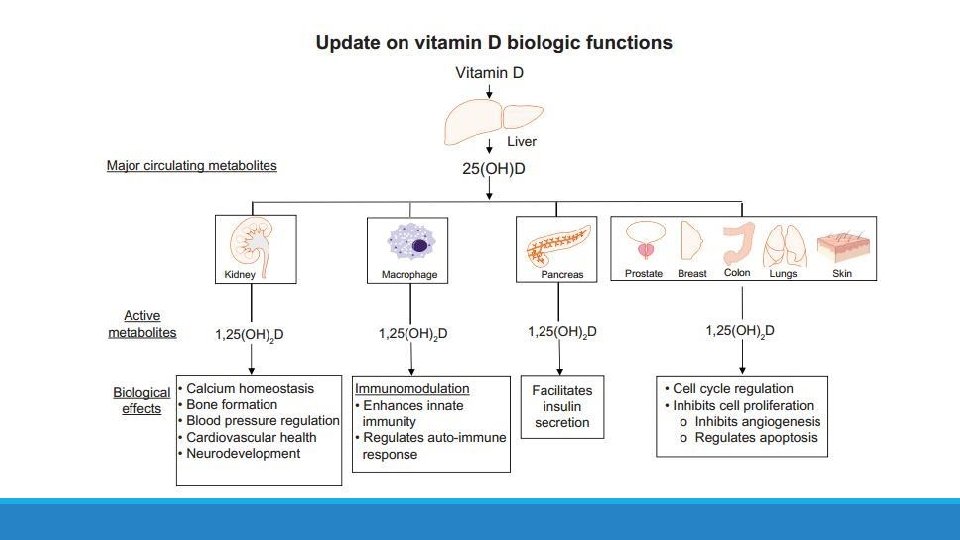
Vitamin D Metabolism

Types of rickets • Nutritional rickets or vitamin D deficient rickets • Vitamin D dependent rickets • Type 1 (Deficiency of renal 25(OH) D 3– 1 -α- hydroxylase, Autosomal recessive. ) • Type 2 (Defective interaction between calcitriol and receptor, Autosomal recessive) • Vitamin D resistant rickets • Secondary rickets

• The incidence of nutritional rickets is rising globally, and hospitalisation is increasing even in high income countries • The prevalence of osteomalacia histologically at postmortem in adult Europeans is as high as 25%. • The true burden of subclinical rickets and osteomalacia remains unidentified • Vitamin D deficiency is pandemic in Europe, in winter affecting nearly 18% of the population, but with 3– 71 times higher risk in dark-skinned ethnic minority groups

Exposure to sunlight ◦ A Caucasian infants Vitamin D requirement are met by exposure to sunlight for 30 minutes per week, clothed only in a diaper, or for 2 hours per week fully clothed with no hat. ◦ Asians require approximately threefold long periods and Africans need six times the same exposure.

Maternal risk factors of Rickets • Mother`s age <17 and >35 years of age • Toxicosis of pregnancy • Extragenital diseases (metabolic diseases, pathology of digestive system, pathology of kidney) • Nutritional defects during pregnancy and breast feeding • Lack exposure to sunlight, physical inactivity • Unfavourable social and living conditions • Short time period between pregnancies üMaternal vitamin D deficiency ü Intrauterine growth retardation, premature labor, low birth weight

Child risk factors of Rickets • Child was born in period from July • Physical inactivity to December • Pathology of liver, kidney and skin • Premature • Obesity • Birthweight over 4 kg • Rapid weight gain • Early feeding of larger volumes of formula milk • Lack exposure to sunlight • Malabsorbtion üSmall bowel enteropathy (e. g. coeliac disease) üPancreatic insufficiency (e. g. cystic fibrosis) üCholestatic liver disease üHigh phytic acids in diet (e. g. chapattis)

CHRONIC LIVER DISEASE • Cirrhosis reduces 25 -hydroxylation of vitamin D • Biliary obstruction: – Prevents absorption of fat soluble vitamin D – Interrupts its enterohepatic circulation CHRONIC RENAL FAILURE • Reduces 1 α hydroxylation of 25 -hydroxy vitamin D leads to low concentration of 1, 25 -di hydroxy vitamin D • Consequently impair calcium absorption from the gut








BIOCHEMICAL FINDINGS OF RICKETS VITAMIN D DEFICIENCY RICKETS – Low-normal serum calcium level – Normal –low phosphate level – Increased secretion of PTH (secondary hyperparathyroidism) to compensate for low calcium – Hyperparathyroidism will increase renal excretion of phosphate, leads to low serum phosphate level – Elevated alkaline phosphatase enzyme – Reduced urinary calcium level – Low level of both calcidiol and calcotriol

The prevalence of dental anomalies in children with rickets 75% 80% Enamel hypoplasia 70% 60% Missing teeth 50% Bilat. Missing mand. Second 40% premolars 37, 50% 25% Bilat. Missing max. 1 st premolars, 20% max. canines, mand. 2 nd premolars 30% 6, 25% 10% 0% Dental anomalies Bilat. Missing mand. Decidios incisor

Crown Mineralization of Primary Teeth Tooth Central incisor Beginning of Crown Mineralization 3– 4 intrauterine months End of Crown Mineralization 4– 5 months Lateral incisor 3– 4 intrauterine months 4– 5 months Canine 5 intrauterine months 9 months First molar 5 intrauterine months 6 months Second molar 6 intrauterine months 10– 12 months Crown Mineralization of Permanent Teeth Tooth Beginning of Crown Mineralization End of Crown Mineralization Central incisor 3– 4 months 4– 5 years Lateral incisor 3– 4 months 4– 5 years Canine 4– 5 months 6– 7 years First premolar 1. 5 – 2 years 5– 6 years Second premolar 2– 2. 5 years 6– 7 years First molar Birth 2. 5– 3 years Second molar 2. 5 – 3 years 7– 8 years Third molar 7– 10 years 12– 16 years

A, Intraoral photograph showing severe defects on upper and lower incisors and canines and slight defects on the first upper bicuspid (arrows). B, Upper jaw. Note the severe enamel hypoplasia on the first permanent molars, whereas the bicuspids are only lightly (first biscuspid) or not (second biscuspid) affected. C, Lower jaw. Note that the second primary right molar is as severely affected as the first permanent molars. Only the bicuspids appear to be healthy. D, Panoramic radiograph showing healthy second and third permanent molars. 12 -year old girl
. B, Upper")
A, Intraoral photograph showing slight defects on upper and lower incisors (arrows). B, Upper jaw. Note the severe decay on the first permanent molars and the presence of the second left primary molar. C, Lower jaw. Note the severe decay on the first permanent molars and the eruption of the second permanent right molar. D, Panoramic radiograph showing deep lesions on the first permanent molars. 11 -year old boy

Other dental findings üSpontaneous gingival and dental abscesses occurring without history of trauma and caries. üRadiographic examinations revealed: ü large pulp chambers ü short roots ü poorly defined lamina dura ü and hypoplastic alveolar ridge

Periodontal disease Calcitriol helps to regulate the immune system and protects against inflammation, so some have suggested that low vitamin D status increases periodontal disease by increasing gingivitis.

Vitamin D-resistant rickets § X-linked dominant metabolic disorder § It is characterized by persistent hypophosphatemia and hyperphosphaturea associated with decreased renal tubular reabsorption of inorganic phosphates §Dental manifistation Vitamin D-resistant rickets • The basic dental defects in vitamin D-resistant rickets seem to be manifested in dentin. • Enamel is usually reported to be normal. • Spontaneous gingival and dental abscesses occur without history of trauma or caries, and radiographic evidence of enlarged pulp chambers with pulpal horns extending beyond the dentino-enamel junction are most important oral findings.

Vitamin D-resistant rickets Clinical examinations revealed fistula at the periapical region of primary maxillary left lateral incisor Periapical radiography showed pulp chambers enlarged with pulp horns extending to the dentino-enamel junctio
- Slides: 49