Rheumatology Examining for Finals Tutor name Tu BS

Rheumatology Examining for Finals Tutor name

Tu. BS attendance • https: //tutorialbooking. com/

Session overview • • Common rheumatological conditions for the OSCE How to present your findings Overview of clinical signs/dermatology Case presentations and viva questions

What is the purpose of an OSCE? “This station tests a student’s ability to perform an appropriate focussed physical examination, demonstrating consideration for the patient, and to report back succinctly describing the relevant findings. It also tests a student’s clinical judgement i. e. the ability to decide the differential diagnosis, choose investigations and formulate a management plan. ”

Presenting your findings • • • What were you asked to do? What were your key positive findings? What were the important negative findings? What does this mean? How would you complete your examination, and what investigations would you do?

What xray changes do you see in rheumatoid arthritis? • • • Subluxation Soft tissue swelling Erosions Deformities Peri-articular osteoporosis Loss of joint space

Rheumatoid Arthritis What is the definition? Symmetrical deforming polyarthritis What % of people with RA are seronegative? ~30% What is rheumatoid factor? Autoantibody, Ig. M against Ig. G What are the features of active synovitis? Redness, swelling, pain What causes the deformity? Rheumatoid tenosynovitis

Extra-articular features on RA What are the extra-articular features of RA? Eyes and mouth – scleritis, episcleritis, sjogrens syndrome Lungs - pulmonary fibrosis/nodules/effusions Heart - pericarditis/effusion, myocarditis Kidneys – amyloid, mesangial glomerulonephritis Haem - Felty’s syndrome, anaemia Skin – nodules, ulcers, Neuro – mononeuritis multiplex, neuropathy, atlanto-axial subluxation Are seronegative more or less likely to have extra articular features? Less likely Why might you order a lateral cervical spine xray pre-operatively in patients with RA? atlanto-axial subluxation

What are the 5 presentations of Psoriatic Arthritis -Asymmetrical Oligoarthritis -DIP disease only -symmetrical polyarthropathy (like RA) -Arthritis Mutilans -Sacroilitis

What are the causes of an acutely Swollen Joint Gout Pseudogout Reactive arthritis Septic arthritis Haemarthrosis

What are the causes of an acutely Swollen Joint What investigations should you do? What other symptoms can be associated with reactive arthritis? Conjunctivitis, rash, balanitis

Case 1

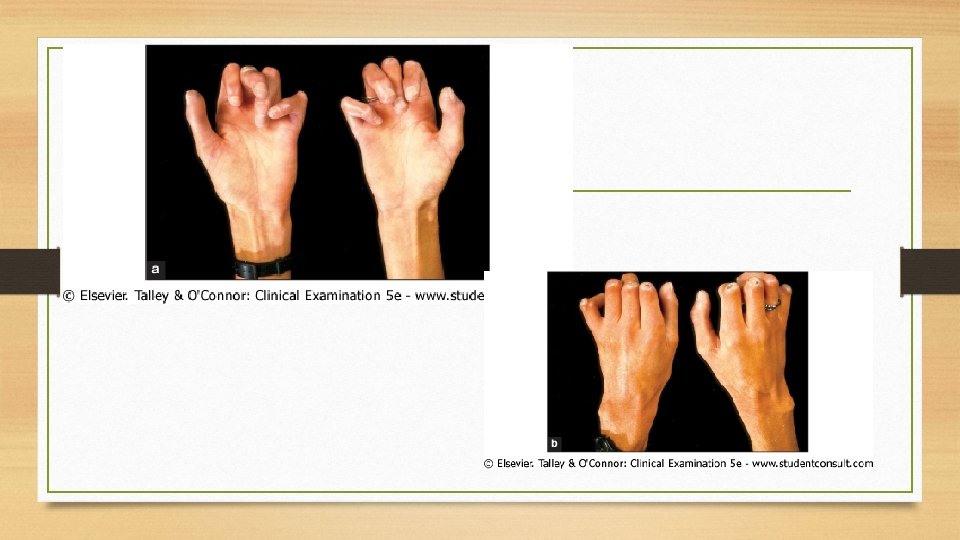
Look • Hard irregular nodules on elbows • Scar over first right MCP joint

Case 1 - feel • Cool joints • No effusion

Case 1 - move • Has difficulty in extending little finger on right • Problems with flexion of fingers • Difficulty with finger abduction on left • Difficulty holding thumb in abduction against force on left

Case 1 - function • Has difficulty doing up small buttons • On direct questioning, she can use a knife and fork

Case 1 - neurovascular status • Intact radial pulses • CRT <2 s • Reduced sensation over left thumb and index and middle fingers Please present your findings.

Would you like to present your findings? • • • Chronic Symmetrical Polyarthropathy Joints affected Active/inactive Seropositive/negative Movement Function Complications – carpal tunnel syndrome Treatments – joint replacement

Case 2

Case 2 - feel • Joints are cool • Fingers are cool • No swelling • No tenderness

Case 2 - move • Fixed flexion deformities of all fingers • Unable to make tight fist • 4+/5 strength, when not limited by deformities • Sensation is normal • Unable to do up small buttons

Case 2 • How would you complete your examination? • Would you like to present your findings?
 • •")
What are the patterns of systemic sclerosis? • Limited cutaneous scleroderma (CREST) • • skin only affected at face, hands & feet Diffuse scleroderma – systemic sclerosis • • skin of trunk and extremities all affected Scleroderma without cutaneous features • skin not affected, but systemic manifestations occur

Case 3

Please present your findings.
,")
Differential for Raynaud’s Phenomenon • Reflex – • • Raynaud’s disease (i. e. idiopathic), vibrating machinery injury, cervical spondylosis CTDs – • scleroderma, mixed CTD, SLE, PAN, RA, polymyositis Arterial disease – • embolism or thrombosis, Buerger’s disease (thromboangiitis obliterans), Trauma Haematological – • polycythaemia, leukaemia, dysproteinaemia, cold agglutinin disease (Ig. M agglutination of RBCs at low temp) • Poisons – • drugs (β-blockers, ergotamine), vinyl chloride

Case 4


Case 4 • • Tender in DIP joints Decreased range of movement Some weakness globally in small muscles of hands Problems doing up buttons Please present your findings.

Case 5



Case 5 - feel and move • • • All digits are tender and swollen Cannot distinguish joint swelling from digit swelling Tender Movement and function is intact, limited by pain only Sensation, peripheral pulses normal Please present your findings.

What are the patterns of arthritis in psoriatic arthropathy? 1. Arthritis mutilans (pencil in cup deformity, telescoping of digits – 3% pts) 2. 3. 4. 5. Asymmetric oligo-arthritis RA-like – symmetrical polyarthritis Ank-spond-like – sacro-iliitis OA-like – distal arthritis involving DIPJ
 Arthritis mutilans – characterised by resorption of phalanges")
DIP joints (nails commonly involved) Arthritis mutilans – characterised by resorption of phalanges

Pencil in cup deformity

Case 6

Please present your findings.

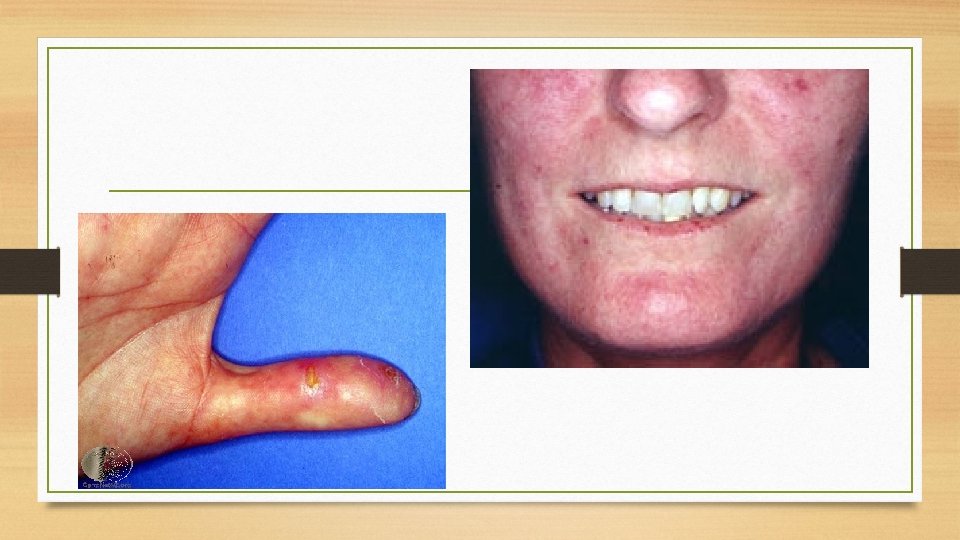
Diagnostic criteria for SLE 4/11 by American College of Rheumatology Discoid rash Renal – proteinuria/casts Oral ulcers ANA Photosensitivity Serositis – pleuritis, pericarditis Arthritis – 2+ joints Haematological (haemolytic Malar rash anaemia, low WCC/Plts) Immunological markers (anti ds. DNA, smooth muscle, antiphospholipid Ab) Neurological changes (seizures, psychosis) (Elevated ESR – not a criterion, but used in monitoring)
 • Hands")
Clinical features of SLE • General – cushingoid, mental state (lupus psychosis) • Hands • • Raynaud’s phenomenon Atrophic skin, bruising (steroids/thrombocytopenia) Rashes – discoid, vasculitic • Palmar erythema Arthropathy Livedo reticularis, purpura Proximal myopathy (active disease/steroids) Face • • • collapse, infection • Abdo - hepatosplenomegaly • Legs • Peripheral oedema secondary to nephrotic syndrome, steroid use • Proximal myopathy, neuropathy, mononeuritis multiplex, cerebellar ataxia Splinter haemorrhages Arms • • • CV – Pulmonary HTN cor pulmonale, pericarditis • Respiratory – pleural effusion, pulmonary fibrosis, Malar/discoid/photosensitive rash Scalp alopecia Eyes – pallor (anaemia), scleritis Mouth – oral ulceration, dry (Sjogren’s) Cervical adenopathy • Other • • Obs – BP (HTN), temperature Urine dip (proteinuria)

Case 7

Case 7 • Can move joints back into position – present.

Jaccoud’s arthropathy • Chronic deforming synovitis • Characterized by ulnar deviation of the second to fifth fingers and subluxation of the metacarpophalangeal (MCP) joints, which are voluntarily correctable by the patients. • Affects up to 50% SLE pts

Dermatology Present what you see!

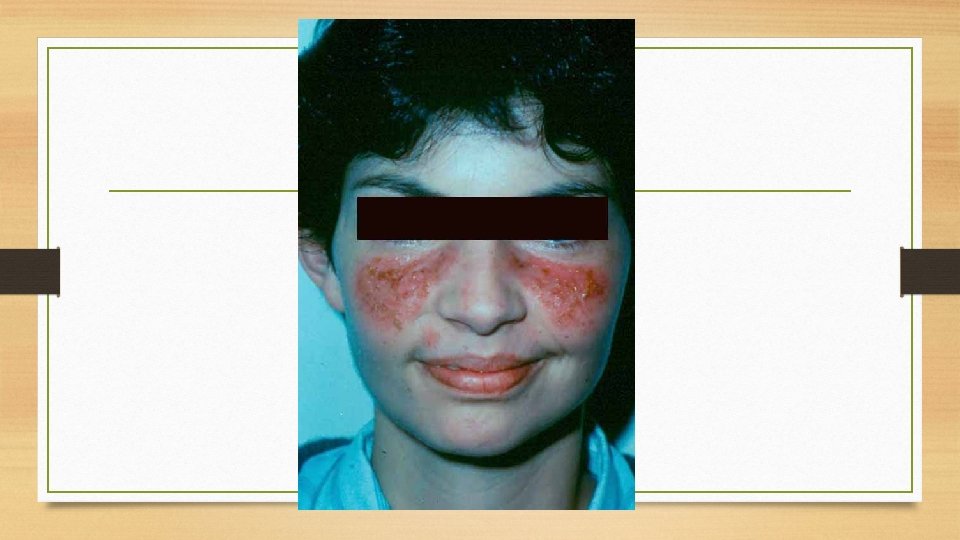
Case 8 Present what you see

Case 8 Discoid lupus – note scarring, alopecia, hyperpigmentation, discoid plaques

Case 9 Present what you see

Case 10 Present what you see

Case 11

Present what you see
 •")
Case 11 Skin signs: • Macular rash (shawl sign – back and shoulders) • Lilac-purple (heliotrope) rash on eyelids, +/- oedema • Nailfold erythema (dilated capillary loops) • Gottron’s papules (roughened red papules over knuckles, elbows, knees • Subcutaneous calcifications • Mechanic’s hands – painful rough skin cracking, affecting tips and lateral aspects of fingers • Alopecia

Case 12

Case 12 Please present your findings.

What do the arrows indicate?

Case 12 • Syndesmophytes

What is this?

Bamboo spine

What are the complications of ankylosing spondylitis? The 7 As: • Anterior uveitis • Apical lung fibrosis • Aortic regurgitation • Aortitis • Achilles tendonitis • Anaemia – normocytic • Amyloidosis – liver, adrenals, kidney

Cases that have previously come up in finals • RA hands, including joint replacements – • Questions on extra-articular disease of rheumatoid, Mx, DMARDs • CREST hands • (including 1 pt – old fistula due to renal involvement, immunosuppressed SCCs, scars on forehead and leg where they have been removed) • OA hands • Psoriatic arthritis • Questions on differential diagnosis, in particular differences between this and RA, and patterns of arthritis in psoriatic arthritis • Ankylosing spondylitis • Paget’s disease • Carpal tunnel syndrome

Session overview • • Common rheumatological conditions for the OSCE How to present your findings Overview of clinical signs/dermatology Case presentations and viva questions

Please complete Tu. BS feedback • Tutor details • For more information on Examining for Finals sessions: • examiningforfinals@gmail. com • www. sefce. net/pulse • With thanks to previous contributors: • Dr Emma Claire Phillips (FY 2) • Dr Kristina Lee (FY 2) • Dr Rachael Kirkbride (FY 2) • Mr Simon Roberts ( Orthopaedic Sp. R)
- Slides: 64