Rh Alloimmunization By M AbdelRahman Nomenclature Exposure to

Rh Alloimmunization By M. Abdel-Rahman

Nomenclature �Exposure to foreign red cell Ag results in production of antibodies in a process known as red cell alloimmunization (formerly termed isoim munization).

Nomenclature �Before the advent of obstetrical ultrasound, the perinatal effects of maternal red cell allo immunization could be recognized only after birth in the affected neonate. Thus, the neonatal consequences of maternal red cell alloimmunization came to be known as hemolytic disease of the newborn (HDN).

Nomenclature �Because the periph eral bloodsmear of these infants demonstrated a large percentage of circulating immature red cells known as erythroblasts, the newborn entity was also known as erythroblastosis fetalis.

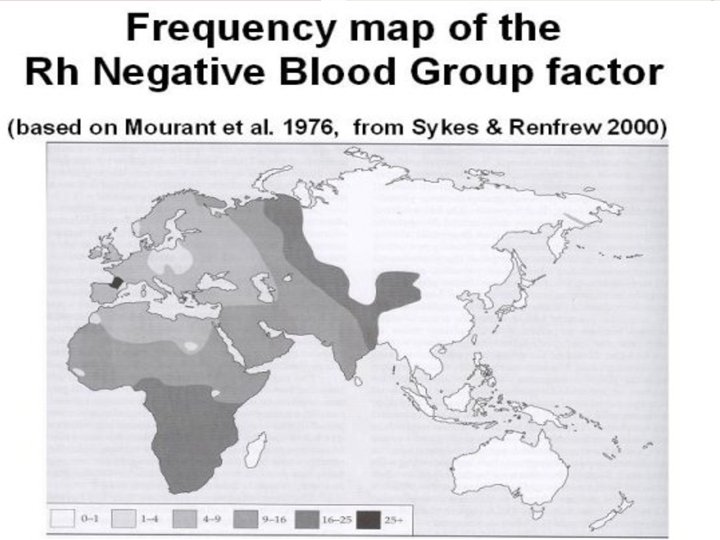
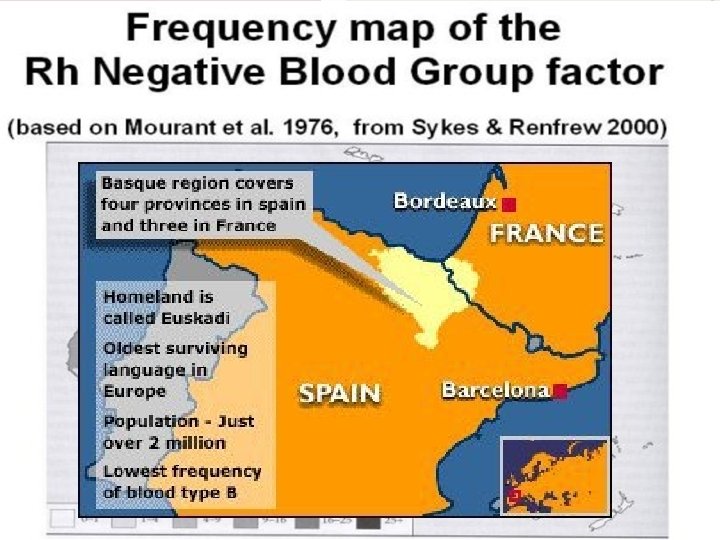
Genetics
 � 75 % during")
Pathogenesis �Exposure to foreign RBC antigens: 1. Pregnancy (FM hge) � 75 % during pregnancy/ delivery � 20 25 % at surgical evacuation of miscarriage � 1 % in spontaneous miscarriage 2. Blood transfusion �Second common cause overall � 1 st common cause of sensitization due to uncomon antigens

Pathogenesis

Pathogenesis � 18 – 27 % of Rh-negative women will become sensitized after their first pregnancy if not given Anti. D. �Each subsequent pregnancy probably accounts for a similar proportion of cases �Maternal fetal ABO incompatibility reduces the risk of D alloimmunization from 16 % to 2 %.

Pathogenesis �The primary immune response to the D antigen occurs over 6 weeks to 12 months. �It is usually weak, consisting predominantly of Ig. M �A second antigen challenge → generates an response is rapid and almost exclusively Ig. G. �the anti D–coated fetal RBCs are destroyed by the RES at an increased rate. �Extramedullary hematopoiesis → liver and spleen are enlarged

Pathogenesis Haemolysis Anaemia Hydrops

presentation �It can range in severity from being vdetectable only in laboratory tests vthrough to severe fetal anaemia resulting in hydrops, stillbirth, or vthe birth of babies with severe anemia and jaundice.

Prevention �Routine testing for Rh type & antibody screen: 1. 2. Booking 28 weeks

Prevention Identify at risk women: �Rh phenotype of the partner ( with counselling regarding paternity if suitable) �Rh genotype of the partner if Rh positive �Rh genotype of the fetus: 1. invasive 2. Non invasive: ff. DNA
: 1. 2. 28 weeks (ACOG, NICE) 34 weeks")
Prevention �Routine antenatal prophylaxis (500 IU): 1. 2. 28 weeks (ACOG, NICE) 34 weeks (NICE) �Routine Postnatal prophylaxis (500 IU): within 72 h (some protection up to 13 days and possibly up to 28 days after delivery. )

Prevention �Give Anti-D in any sensitizing event: 1. 2. 3. 4. 5. 6. 7. 8. 9. Spontaneous miscarriage Induced abortion Ectopic pregnancy Hydatidiform mole Amniocentesis , CVS, Fetal blood sampling Placenta previa with bleeding, Suspected abruption IUFD Blunt trauma to the abdomen External cephalic version

Dose �During pregnancy: �< 20 weeks: 250 IU �> 20 weeks: 500 IU �At delivery: 500 IU + test 1. 2. 3. 4. 5. for large FM hge: traumatic deliveries including C. S. manual removal of the placenta twins stillbirths unexplained hydrops fetalis.

Kleihauer Betke test Source: William Haematology, 8 th ed.

Kleihauer Petke test Number of Fetal cells Estimated FMH= × Number of maternal cells maternal blood volume (85 m. L/ kg). • 99 % have FMH < 4 ml at delivery → 500 IU Anti D • 99. 7 % have FMH < 15 ml at delivery→ 1500 IU Anti D

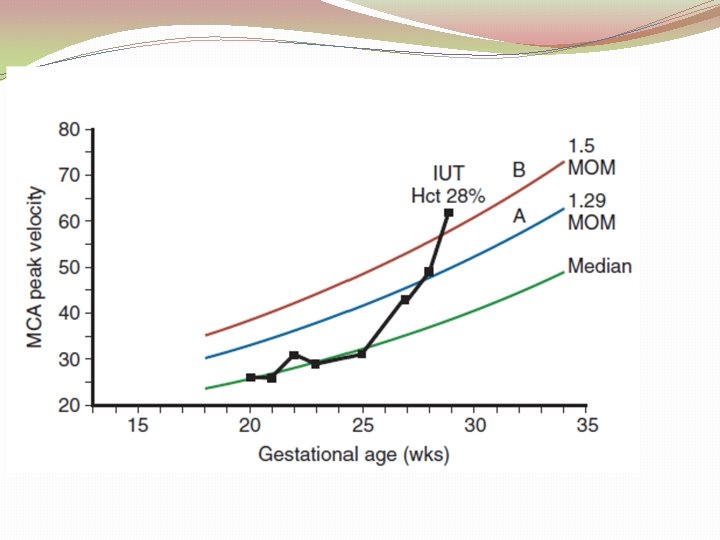
Management of sensitized women Antibody titer: �>4 IU/m. L refer to fetal medicine unit �Repeat the antiglobulin test / 2 weeks �A critical titer is defined as the anti red cell titer associated with a significant risk for hydrops fetalis. �This is 15 IU/ml is used as a cut of level for testing the MCA PSV. �If there is history of previously affected pregnancy → doppler test at 18 weeks

Management of sensitized women The ΔOD 450 is an outdated tool and should be performed only when there is no access to middle cerebral artery (MCA) Doppler because: 1. ΔOD 450 is inferior in accuracy and 2. ΔOD 450 is more dangerous for mother and child.

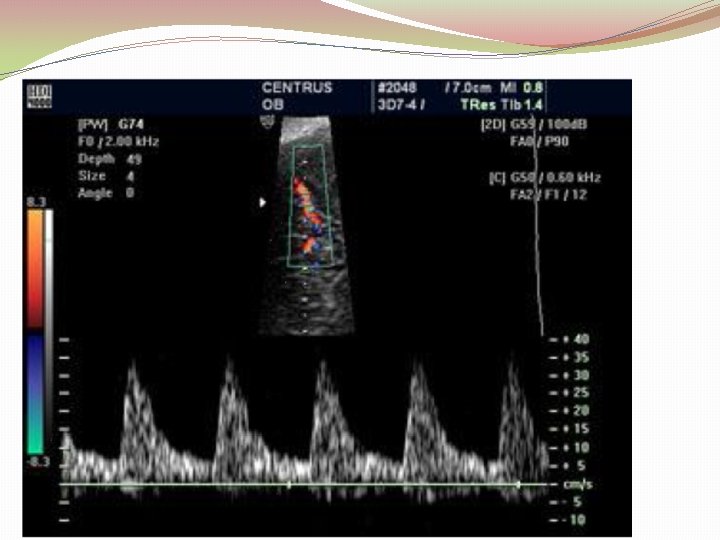
Management of sensitized women � Weekly MCA PSV �MCA PSV > 1. 5 MOM is indication for fetal blood sampling ± transfusion � 100% sensitivity and a false positive rate of 12%. This method of monitoring should be used with caution after 36 weeks as the sensitivity decreases.
: 1. Non invasive 2. Wide")
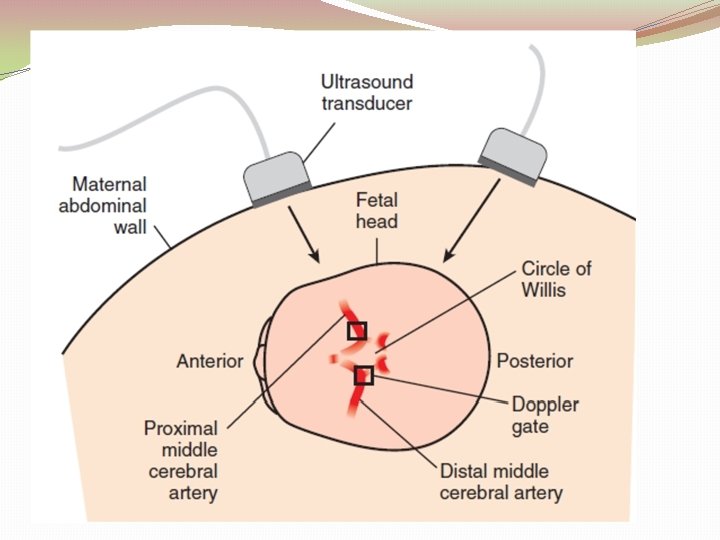
Middle Cerebral Artery �Principle: “brain sparing” �Advantage (over amniocentesis): 1. Non invasive 2. Wide range of disease severity for a given ΔOD 450 3. More sensitive than ΔOD 450 4. Can be used with other red cell alloimmunization: ΔOD 450 system is modeled on anti D alloimmunization. 5. No laboratory errors


Fetal blood sampling & transfusion �Transfuse the fetus if Hct is less than 30 %. �O negative, CMV negative blood that has been cross matched with a maternal blood sample is used for fetal transfusion. �Donor cells are packed to a volume of 75%– 90% to prevent volume overload, and they are irradiated to minimize the risk of graft versus host disease. �The two common sites used are the intrahepatic vein or the umbilical vein at the placental cord insertion site.

Fetal blood sampling & transfusion �The procedure related perinatal loss rate was 1. 6% per procedure. �Complications: PROM, PTL, infection, emergency C. S, and perinatal death. Emergency C. S and perinatal death are the commonest complications. �Emergency C. S : In a low risk population the risk is approximately 1. 5%– 3% but, if the fetus is hydropic, the risk is substantially increased (20%).

Fetal blood sampling & transfusion �Usually, an interval of 3 to 5 W is the norm before the next transfusion. Weekly MCA monitoring is essential. �With careful monitoring and appropriate timing of transfusions, delivery should be anticipated at 37– 38 W.

Fetal blood sampling & transfusion �At delivery, cord blood should be collected for analyses of Hb, Hct, and bilirubin, and for a direct coombs test. �The mode of delivery is dependent on standard obstetric grounds. Prior intrauterine therapy is not an indication for an C. S. �The overall survival is 84% 1. Nonhydropic fetuses : 92% 2. hydropic fetuses: 70%.

Optical density

Liley curve Liley AWJ: Scanning Spectrophotometry. Obstet. Gynecol. 1961; 82: 1359

�Amniocentesis is repeated at 1 to 2 week intervals, depending on the gestational age, the zone of the ΔOD 450, and the change from the preceding sample. �A fetal blood sample is performed when either the ΔOD 450 is in zone 3 or serial amniotic fluid specimens reveal a progressive and rapid rise of the ΔOD 450 into the upper 80% of zone 2.

Queenan curve Scott F. , Chan F. Y. : Assessment of the Clinical Usefulness of the ‘Queenan’ Chart Vs the ‘Liley’ Chart in Predicting Severity of Rh Iso Immunization. Prenat. Diagn. 18: 1143 1148

Thank You
- Slides: 37