Review of Antidepressants a look at the newest


 • Monoamine Oxidase Inhibitors (MAOIs)")


 Safe in CV disease; good efficacy data")
 • Agitation, Insomnia,")
 Lower sexual dysfunction")
 Least sexual dysfunction")

 • acute, continuation,")







")







- Slides: 39
Review of Antidepressants & a look at the newest agent Vortioxetine
Outline • Pharmacology • Review new agent Vortioxetine • Clinical Pearls – what’s the difference between the agents • Review evidence of older agents and vortioxetine
• Tricyclic Antidepressants (TCA’s) • Monoamine Oxidase Inhibitors (MAOIs)
SSRIs, SNRIs, NDRIs and TCAs are re-uptake inhibitors of 5 -HT or NE aka 5 -HT transporter (SERT) blockade …
Mirtazapine
SSRI Pros Concerns / Comments Sertraline (Zoloft®) Safe in CV disease; good efficacy data FDA analysis – reduction in SI More diarrhea High male sexual dysfunction Citalopram (Celexa®) Safe in CV disease Well tolerated QTc prolongation (40 mg max) Escitalopram (Cipralex®) Well tolerated Efficacy data QTc prolongation Possibly higher sexual dysfx Formulary RESTRICTED to pts on PTA Fluoxetine (Prozac®) Useful in OCD, eating d/o No weight gain, stimulating FDA analysis – reduction in SI Very long half-life Fluvoxamine (Luvox®) Useful in OCD MANY drug interactions Most nausea and sedation Paroxetine (Paxil®) Useful in Anxiety VERY anticholinergic, caution delrium in elderly, High discontinuation rxn, Highest sexual dysfx and Wt gain in class FDA analysis – increase in SI Overall Class Side Effects N/V/D, sexual dysfunction, SIADH, Risk of GI bleeds, sweating, dry mouth, anxiety (esp early or fast titration), tremor, headache
Consider increased Serotonin … • Act on Serotonin 2 receptors (post-synaptically) • Agitation, Insomnia, Anxiety, Akathisia • Panic • Sexual dysfunction • Act on Serotonin 3 receptors (post-synaptically) • Nausea, Diarrhea, GI distress • Headache
Clinical Pearls - SNRIs SNRI Pros Concerns / Comments Venlafaxine (Effexor®) Lower sexual dysfunction than SSRIs Less wt gain Dual action without the TCA side effects May help neuropathic pain High incidence nausea High discontinuation rxn Desvenlafaxine (Pristiq®) Active metabolite of venlafaxine Increased cost / not covered on Plan G NOT on hosp formulary Duloxetine (Cymbalta®) May be helpful in chronic pain / neuropathy Possibly less HTN than Venlafaxine Weaker evidence of efficacy in depr Increased cost / not covered by Plan G NOT on hosp formulary Overall Class Side Effects N/V/D, risk of hypertension at higher doses, sexual dysfunction, SIADH, Risk of GI bleeds, sweating, anxiety (esp early or fast titration), tremor, headache, insomnia
Clinical Pearls - Others Drug Pros Concerns / Comments Bupropion (Bupropion®) Least sexual dysfunction Least wt gain (may cause wt loss) Helpful in smoking cessation Agitation, insomnia, tremor Caution with seizure hx or eating d/o Sweating Mirtazapine (Remeron®) Least sexual dysfunction Available as dissolvable tab Minimal GI upset or nausea Sedation (at doses 15 mg or LESS); more activating at higher doses due to NE action Weight gain Dry mouth, edema * Mirtazapine BLOCKS post-synaptic Serotonin 2 and 3 receptors – helpful for anxiety and insomnia, no GI upset * Trazodone BLOCKS Serotonin 2 receptors – helpful for insomnia
Clinical Pearls – TCA’s • Serotonin and NE reuptake inhibitors • ALSO block – Histamine, Muscarinic, Alpha receptors Tachycardia, hypotension Weight gain, sexual dysfunction Sedation Dry mouth, constipation, confusion/delirium risk, urinary retention, dry eyes, blurred vision • Can be FATAL in overdose – cardiac toxicity, seizures • Also cause sweating, tremors, SIADH, rash • • • Helpful in OCD (esp Clomipramine) or significant anxiety, atypical depressions • Desipramine and Nortriptyline often tolerated better than Amitriptyline or Imipramine
Comparative Efficacy • Systematic Review for treatment of MDD (1980 -2007) • acute, continuation, maintenance phases; includes unpublished data • Outcomes • Efficacy of response, speed and onset of response, remission, maintenance of remission and Qo. L • Acute phase treatment of MDD (N=26, 349) • 80 head-to-head RCTs (at least 6 wks duration), 34 placebo-controlled trials (indirect comparisons, meta-regression) • Across all efficacy trials for acute phase treatment of depression • 46% patients achieve remission • 62% patients achieve response • No reliable predictors of response Gartlehner G et al. Ann Int Med 2008; 149: 734 -750
Results Acute Phase Treatment Results Comments Efficacy and Effectiveness ESC over CIT Similar rates among all agents Not clinically significant SER & VEN over FLX Onset of Action MIR over CIT, FLX, SER or PAR Only fair quality trials Maintaining Response or Remission No difference FLX = SER; FLV = SER; TRAZ = VEN Only 3 trials Treatment Resistant Depression STAR-D Trial: BUP = SER = VEN Another fair qual trial: VEN over CIT, FLX, SER, MIR and PAR
Assessment of Harm • Adverse event profiles similar • VEN: higher incidence of N/V than SSRI’s (33% vs. 22%) • MIR: higher wt gain than SSRI’s • PAR and VEN: highest rates of discontinuation syndrome • Sexual dysfunction (overall 50% incidence) • Bupropion causes significantly less • PAR has highest rates among SSRI’s • Insufficient evidence to draw conclusions about: • Risk of Suicidality • Cardiovascular events • Weak evidence – VEN may increase CV risk
Cipriani A. et al. Lancet 2009; 373: 746 -758 Sys review; Acute tx MDD; response rates, N=25928
Comments • Efficacy • Escitalopram, Mirtazapine, Sertraline and Venlafaxine possibly more efficacious • Tolerability • Escitalopram, Sertraline, Bupropion and Citalopram possibly better tolerated • Only about 50 -60% pt achieve response in acute tx trials • Only about 1/3 pts achieve remission • If don’t respond to first SSRI tried, may respond to a different SSRI (based on STAR-D trial) • Augmentation strategies if partial response …
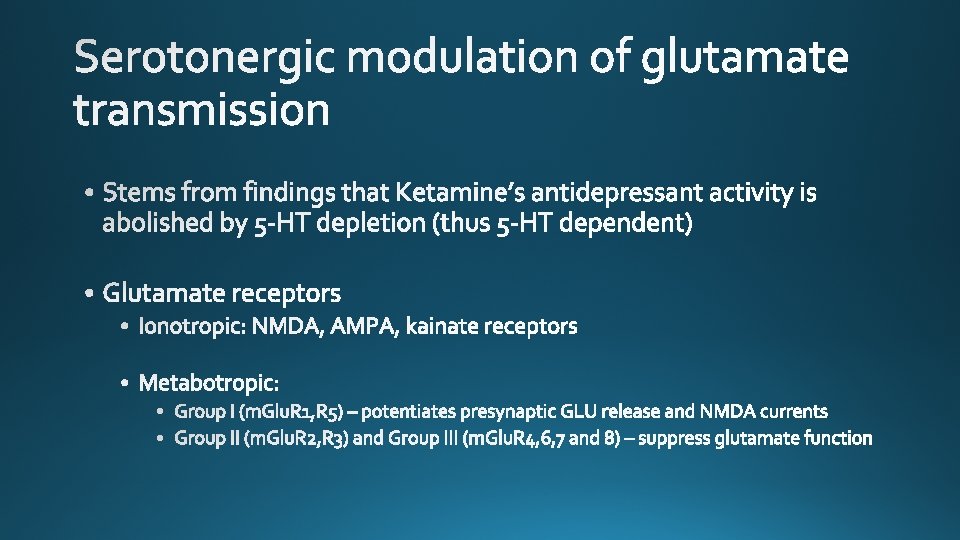
5 -HT reuptake inhibitor 5 -HT 1 a agonist 5 -HT 1 b partial agonist 5 -HT 1 d/3/7 antagonist In vivo non-clinical studies also demonstrated that vortioxetine enhances levels of 5 -HT, NE, DA, Ach and Hist in specific areas of the brain • Modulates glutamate transmission • • •
1 A: incr or decr glu; modulates memory; anxiolytic 1 B: agonism antidepressant / antagonism memory impr 3: increases glu by reducing GABA; AD activity and memory impr 7: incr or decr glu; AD activity and memory impr
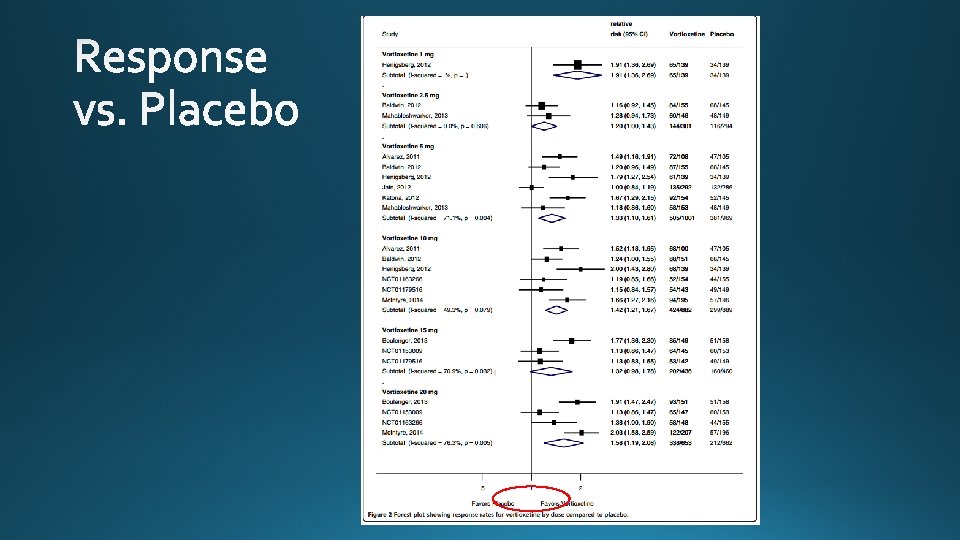
Meeker et al. Systematic Reviews 2015; 4: 21
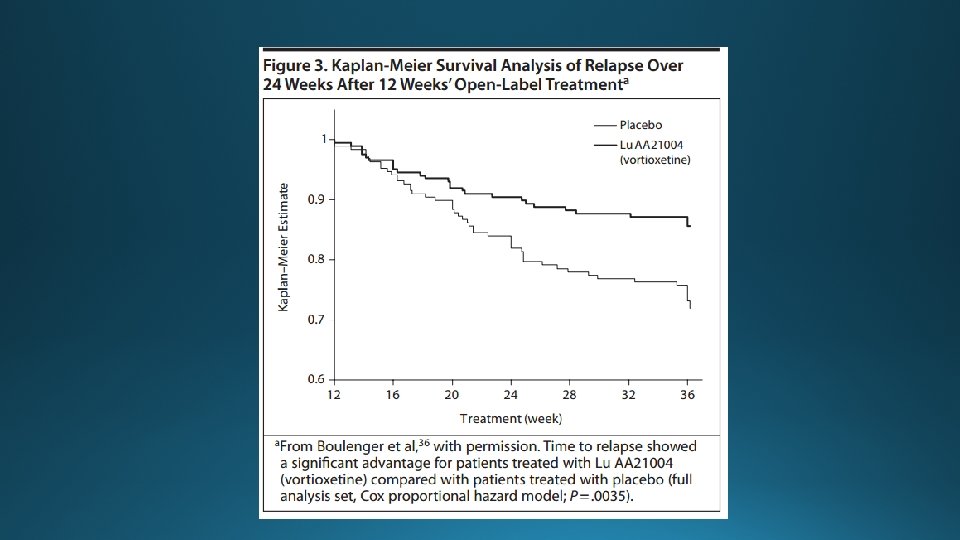
Overall not significant difference from placebo in the short trial duration (6 -8 wks) …
• 5 of 6 trials used duloxetine as active comparator • Individual trials not powered to compare active arms • Pooled comparison show data favors SNRI response rates
• NS difference between active arms • Short trial length
J Psychopharmacol 2012; 26: 1408 -1416
Drug Approx Cost per Month Citalopram $20 Venlafaxine $21 -42 Escitalopram $25 Desvenlafaxine $85 Sertraline $24 -38 Duloxetine $74 -274 Bupropion $24 -47 Vortioxetine $100 Mirtazapine $14 -21
American Fam Physician 2015; 91: 5 STEPS New Drug Reviews
Thank-you!!!
Atypical Antipsychotic Augmentation • Risperidone, Aripiprazole, Olanzapine and Quetiapine have been studied as augmenting to antidepressant therapy in pts who have not responded to monotherapy • All had a small-modest effect over placebo for improvement in depression severity and remission • Pooled Remission NNT 10 (8 -15) … Olanzapine weakest evidence to support • All caused significant side effects • Sedation, Akathisia, EPS, Metabolic changes to glucose and cholesterol, Weight gain • Questionable benefit on quality of life measures • Would reserve for • patients who have depression with psychotic features or atypical features; • patients who have failed multiple trials of mono/dual antidepressant therapy; and • pts who would qualify for ECT but who refuse to consent PLOS Medicine 2013; 10: e 1001403