Rev MED 300 SBAs in Medicine and Surgery

Rev. MED: 300 SBAs in Medicine and Surgery By Lasith Ranasinghe & Oliver Clements (Imperial College London, UK) 25% off with the online code WSREVMED 25 Valid until 31 August 2020 Only at www. worldscientific. com

Endocrinology Part 1 Silvia Muttoni

Disclaimer “Med. ED does not represent the ICSM Faculty or Student Union. This lecture series has been designed and produced by students. We have made every effort to ensure that the information contained is accurate and in line with Learning Objectives featured on SOFIA, however, this guide should not be used to replace formal ICSM teaching and educational materials. ”

Outline q Diabetes q Sodium imbalance q Pituitary disease q Thyroid disorders q Acromegaly q MEN q Carcinoid syndrome
 hypotonic polyuria")
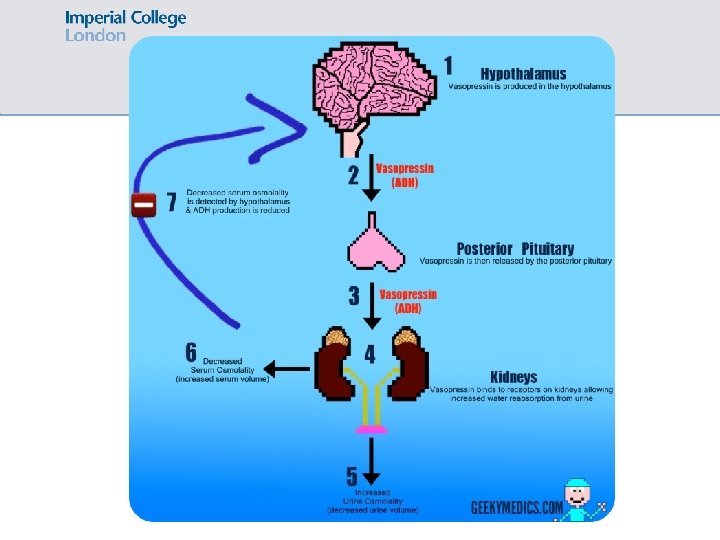
Diabetes insipidus Inadequate secretion of or insensitivity to vasopressin (ADH) hypotonic polyuria
 hypotonic polyuria 2 types:")
Diabetes insipidus Inadequate secretion of or insensitivity to vasopressin (ADH) hypotonic polyuria 2 types: • Cranial/central (posterior pituitary fails to secrete ADH) • Nephrogenic (collecting ducts insensitive to ADH) Causes: • Cranial: pituitary tumour, infection (meningitis), sarcoidosis • Nephrogenic: ↑ Ca, ↓ K, lithium, inherited (AVPV 2 gene), idiopathic
 – UO often >3 L • Polydipsia")
Diabetes insipidus Presentation: • Polyuria (including nocturia) – UO often >3 L • Polydipsia • Symptoms of hypernatremia: lethargy, irritability, confusion Investigations: • General: U&Es (Ca, Na, K), glucose (to exclude DM) • Diagnostic: water deprivation test

Diabetes insipidus – water deprivation test • Water is restricted for 8 hours • Plasma and urine osmolality are measured every hour • After 8 hours, give desmopressin and measure urine osmolality Water restriction causes… Normal DI – cranial DI – nephrogenic Rise in ADH ↑ plasma osm Urine osm >600 (concentrated) Desmopressin causes…

Diabetes insipidus – water deprivation test • Water is restricted for 8 hours • Plasma and urine osmolality are measured every hour • After 8 hours, give desmopressin and measure urine osmolality Water restriction causes… Desmopressin administration causes… Normal Rise in ADH ↑ plasma osm Urine osm >600 (concentrated) DI – cranial Lack of ADH urine is unable to concentrate Urine osm <400 Urine osm ↑ by >50% after desmopressin Lack of ADH urine is unable DI – nephrogenic to concentrate Urine osm <400 Urine osm ↑ by <45% after desmopressin

Diabetes insipidus Management: 1. Treat the cause 2. Cranial: intranasal desmopressin 3. Nephrogenic: thiazide diuretic or NSAIDs

Diabetes mellitus Pathophysiology Presentation Risk factors Diagnosis Management Type 1 DM Type 2 DM Hyperglycaemia due to deficiency of insulin production (autoimmune destruction of beta cells in 90%) Hyperglycaemia due to ↑ peripheral resistance to insulin action

Diabetes mellitus Type 1 DM Type 2 DM Pathophysiology Hyperglycaemia due to deficiency of insulin production (autoimmune destruction of beta cells in 90%) Hyperglycaemia due to ↑ peripheral resistance to insulin action Presentation Polyuria + polydipsia • Tiredness & weight loss • DKA: N&V, abdo pain, Kussmaul breathing, sweet breath Risk factors Diagnosis Management

Diabetes mellitus Type 1 DM Type 2 DM Pathophysiology Hyperglycaemia due to deficiency of insulin production (autoimmune destruction of beta cells in 90%) Hyperglycaemia due to ↑ peripheral resistance to insulin action Presentation Polyuria + polydipsia • Tiredness & weight loss • DKA: N&V, abdo pain, Kussmaul breathing, sweet breath Risk factors Diagnosis Management Susceptibility genes: HLA DR 3/4 Other autoimmune conditions Obesity, FH, ethnicity, endocrine, drugs

Diabetes mellitus Type 1 DM Type 2 DM Pathophysiology Hyperglycaemia due to deficiency of insulin production (autoimmune destruction of beta cells in 90%) Hyperglycaemia due to ↑ peripheral resistance to insulin action Presentation Polyuria + polydipsia • Tiredness & weight loss • DKA: N&V, abdo pain, Kussmaul breathing, sweet breath Risk factors Diagnosis Management HLA DR 3/4 Other autoimmune conditions Obesity, FH, ethnicity, drugs Blood glucose measurement • Fasting ≥ 7 mmol/L • Random >11. 1 mmol/L

Diabetes mellitus Type 1 DM Type 2 DM Pathophysiology Hyperglycaemia due to deficiency of insulin production (autoimmune destruction of beta cells in 90%) Hyperglycaemia due to ↑ peripheral resistance to insulin action Presentation Polyuria + polydipsia • Tiredness & weight loss • DKA: N&V, abdo pain, Kussmaul breathing, sweet breath Risk factors HLA DR 3/4 Other autoimmune conditions Diagnosis Management Obesity, FH, ethnicity, drugs Blood glucose measurement • Fasting ≥ 7 mmol/L • Random >11. 1 mmol/L Insulin Patient education In DKA 1 st line treatment is fluids 1 st line = diet and lifestyle 2 nd line = metformin +/- sulphonylurea +/- insulin

Outline ü Diabetes q Sodium imbalance q Pituitary disease q Thyroid disorders q Acromegaly q MEN q Carcinoid syndrome

Sodium imbalance Normal range of Na: 135 -145 mmol/L Na can be ↑ or ↓
 is a WATER PROBLEM caused by too much ADH: physiological")
HYPOnatraemia ↓ Na (<135) is a WATER PROBLEM caused by too much ADH: physiological or inappropriate secretion When you see ↓ Na 1. Think volume status v Dry pt postural hypotension, dry mucous membranes, tachycardic v Wet pt peripheral oedema, raised JVP v If neither are mentioned, you can assume the patient is euvolaemic

Hypovolaemia Euvolaemia = ENDOCRINE Hypervolaemia Drop in BP detected by hypothalamus → more ADH secreted in order to absorb more water. 1. Hypothyroidism, 2. Hypoadrenalism, 3. SIADH (pneumonia/cancer) 1. HF 2. Cirrhosis 3. Nephrotic syndrome Causes 1. Diarrhea 2. Vomiting 3. Diuretics Signs Reduced turgor, postural hypotension, dry mucous membrane. Oedematous, high JVP Ix - Clinically hypovolaemic TFTs - Low urine sodium Short syn. ACTHen: ACTH injection kidneys will detect volume (cortisol will not rise) Drug review, breast examination, and hang on to salt CXR, brain MRI (measure off diuretics) Fluid overloaded Low urine sodium aldosterone secretion --> retention of Na If very severe hyponatremia (seizures/↓ consciousness), can give slow hypertonic saline but change in [Na+] must not exceed 10 mmol/L in the first 24 hours risk of central pontine myelinolysis
 Causes: vomiting, diarrhea, diabetes insipidus, primary aldosteronism Presentation: lethargy, irritability,")
HYPERnatramia ↑ Na (>145) Causes: vomiting, diarrhea, diabetes insipidus, primary aldosteronism Presentation: lethargy, irritability, thirst, signs of dehydration, confusion, coma, fits Management: replace water

Outline ü Diabetes ü Sodium imbalance q Pituitary disease q Thyroid disorders q Acromegaly q MEN q Carcinoid syndrome

Syndrome of inappropriate ADH SIADH = too much ADH secretion = too much water is reabsorbed So serum Na ↓, urine Osm ↑, urine Na ↑ SIADH is not a final diagnosis – need to find the cause (clues in the hx!) Causes of SIADH: 1. 2. 3. 4. CNS pathology Lung pathology Drugs: SSRI, TCA, opiates, PPIs, carbamazepine Tumours (do not forget breast cancer!) Management: 1. Treat underlying cause 2. Fluid restrict to 0. 5 -1 L 3. If ineffective give demeclocycline or vasopressin receptor antagonist e. g. tolvaptan

Hypovolaemia Euvolaemia = ENDOCRINE Hypervolaemia Drop in BP detected by hypothalamus → more ADH secreted in order to absorb more water. 1. Hypothyroidism, 2. Hypoadrenalism, 3. SIADH (pneumonia/cancer) 1. HF 2. Cirrhosis 3. Nephrotic syndrome Causes 1. Diarrhea 2. Vomiting 3. Diuretics Causes of SIADH: 1. CNS pathology 2. Lung pathology 3. Drugs: SSRI, TCA, opiates, PPIs, carbamazepine 4. Tumours (do not forget breast cancer!) Signs Reduced turgor, postural hypotension, dry mucous membrane. SIADH: reabsorbing lots of water so serum Oedematous, high JVP Na low, urine Osm high, urine Na high. Ix - Clinically hypovolaemic - Low urine sodium kidneys will detect volume and hang on to salt (measure off diuretics) TFT Fluid overloaded Short syn. ACTHen: ACTH injection (cortisol Low urine sodium will not rise) aldosterone secretion --> Drug review, breast examination, CXR, retention of Na brain MRI Mx Saline (this abolishes the stimulus for ADH secretion) Treat the cause Fluid restrict

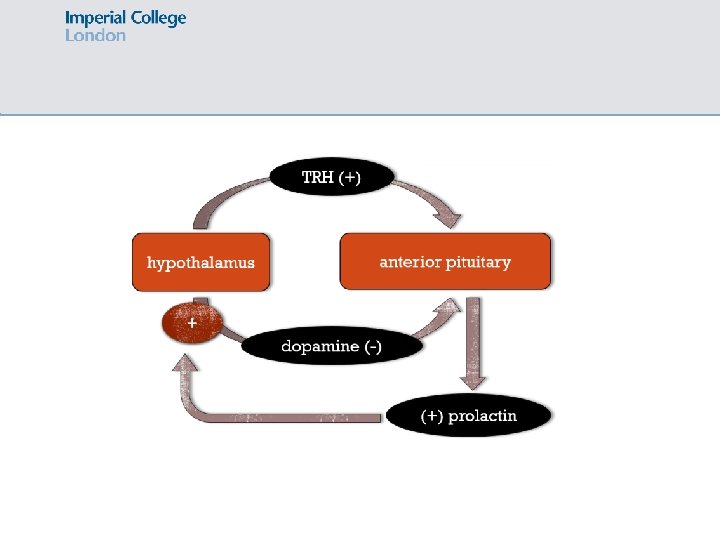
Hyperprolactinaemia Excess circulating prolactin
 • Hypothyroidism • Drugs e. g. metoclopramide, antipsychotics")
Hyperprolactinaemia Causes: • Pituitary prolactinoma (commonest) • Hypothyroidism • Drugs e. g. metoclopramide, antipsychotics (DA antagonists) • Physiological! Pregnancy, breast feeding Presentation: • Women: galactorrhoea, amenorrhoea, infertility, loss of libido • Men: loss of libido, infertility, galactorrhoea uncommon • Mass effects of tumour: headache, loss of visual fields Investigations: • Prolactin • TFTs • Pituitary MRI

Hyperprolactinaemia Management: 1 st line = DA agonist e. g. bromocriptine and carbergoline 2 nd line = surgery

Outline ü Diabetes ü Sodium imbalance ü Pituitary disease q Thyroid disorders q Acromegaly q MEN q Carcinoid syndrome

Thyroid

Thyroid disorders Hyperthyroidism Hypothyroidism Heat intolerance, sweating Cold intolerance Palpitations, irregular pulse Bradycardia Irritable Lethargy Weight loss but good appetite Weight gain Diarrhoea Constipation Menstrual irregularities in females, impotence in men Menstrual disturbance in females Tremor Dry skin, cold hands ↓ TSH, ↑ T 3/4 ↑TSH, ↓T 3/4

Hyperthyroidism Excess circulating T 4/T 3 Due to: 1. Increase thyroid hormone synthesis: hyperthyroidism 2. Increased release of stores thyroid hormones: thyroiditis

Hyperthyroidism Cause of hyperthyroidism Features Grave’s disease Autoantibodies to TSH receptor. Associated with other AI diseases e. g. Addison’s, vitiligo, T 1 DM (80%) Grave’s triad = exophthalmos, pretibial myxedema and thyroid acropachy

Hyperthyroidism Cause of hyperthyroidism Features Grave’s disease Autoantibodies to TSH receptor. Associated with other AI diseases e. g. Addison’s, vitiligo, T 1 DM (80%) Grave’s triad = exophthalmos, pretibial myxedema and thyroid acropachy De Quervain’s thyroiditis Post-viral, fever, high ESR. Causes painful goitre. Self-limiting (treat with NSAIDs)

Hyperthyroidism Cause of hyperthyroidism Features Grave’s disease Autoantibodies to TSH receptor. Associated with other AI diseases e. g. Addison’s, vitiligo, T 1 DM (80%) Grave’s triad = exophthalmos, pretibial myxedema and thyroid acropachy De Quervain’s thyroiditis Post-viral, fever, high ESR. Causes painful goitre. Self-limiting (treat with NSAIDs) Toxic multinodular goitre In elderly and iodine deficient areas

Hyperthyroidism Cause of hyperthyroidism Features Grave’s disease Autoantibodies to TSH receptor. Associated with other AI diseases e. g. Addison’s, vitiligo, T 1 DM (80%) Grave’s triad = exophthalmos, pretibial myxedema and thyroid acropachy De Quervain’s thyroiditis Post-viral, fever, high ESR. Causes painful goitre. Self-limiting (treat with NSAIDs) Toxic multinodular goitre In elderly and iodine deficient areas Adenoma Solitary nodule producing T 3/4

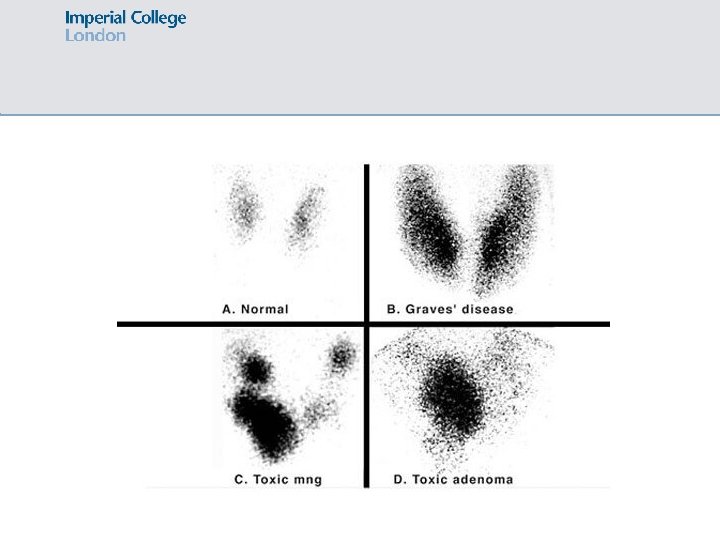
Hyperthyroidism – radioisotope scan Cause of hyperthyroidism Radioisotope scan findings Grave’s disease Diffuse increased uptake (smooth diffuse goitre) De Quervain’s thyroiditis NO uptake Toxic multinodular goitre Multiple areas of increased uptake Adenoma Single area of increased uptake
 • Iodine deficiency")
Hypothyroidism Causes: • Autoimmune Hashimoto’s thyroiditis (commonest cause in the West) • Iodine deficiency (commonest cause worldwide) • Iatrogenic: post-surgery, radioiodine, amiodarone • De Quervain’s thyroiditis hyperthyroidism then hypothyroidism. Usually self resolving but may need thyroxine replacement for a few weeks • Congenital thyroid dysgenesis ↑ TSH, ↓ T 3/4 Management = levothyroxine 25 -200 micrograms/day (monitor TFTs at 6 weeks and adjust dose accordingly)

Thyroid cancer Type Features Papillary Most common. Affects younger patients RF: radiation exposure Buzzwords: Psammoma bodies, Orphan Anne nuclei Follicular Affects middle aged women especially Buzzwords: Hurthle cells Medullary Associated with MEN 2 (? FHx) Lymphoma More common in females. Generally occurs after pre-existing Hashimoto’s thyroiditis Anaplastic Elderly females Buzzwords: giant cells, pleomorphic hyperchromatic nuclei

Outline ü Diabetes ü Sodium imbalance ü Pituitary disease ü Thyroid disorders q Acromegaly q MEN q Carcinoid syndrome

Acromegaly Hypersecretion of growth hormone in adults Same condition in children is known as gigantism. Usually caused by a GH secreting adenoma in the pituitary. GH stimulates release of IGF-1 growth of bones and soft tissues Presentation: rings and shoes become right, ↑ sweating, coarse facial features, sleep apnoea, weight gain, headaches/visual disturbance, carpal tunnel syndrome, hypertension, insulin resistance

Acromegaly Investigations: • Screening: serum IGF-1 • Diagnostic: OGTT acromegalics fail to suppress GH after 75 g glucose load • MRI brain to visualise the pituitary tumour Management: • 1 st line = transphenoidal hypophysectomy • 2 nd line = somatostatin analogue e. g. ocreotide

Outline ü Diabetes ü Sodium imbalance ü Pituitary disease ü Thyroid disorders ü Acromegaly q MEN q Carcinoid syndrome

MEN Hormone producing tumours in multiple organs Autosomal dominant

MEN Type Features • Parathyroid adenoma/hyperplasia hyperparathyroidism, (mutation in menin high Ca gene chr 11) • Pancreas: insulinoma, gastrinoma • Pituitary: prolactinoma, acromegaly, adrenal, carcinoid tumours MEN 1 MEN 2 (mutation in RET gene chr 10) MEN 3 aka 2 B • Thyroid: medullary thyroid cancer (in ALL) • Adrenal: phaeochromocytoma (in 50%) • Parathyroid hyperplasia • Med thyroid carcinoma + phaeo (as in MEN 2) • + Mucosal neuromas: bumps on lips/cheeks/tongue/eyelids • + Marfanoid appearance • NO hyperparathyroidism

Outline ü Diabetes ü Sodium imbalance ü Pituitary disease ü Thyroid disorders ü Acromegaly ü MEN q Carcinoid syndrome

Carcinoid syndrome Constellation of symptoms caused by systemic release of humoral factors from carcinoid tumours They produce secretory products such as serotonin, histamine, tachykinins and prostaglandin Common sites for carcinoid tumours are appendix and rectum Presentation: paroxysmal flushing, diarrhea, crampy abdominal pain, wheeze, sweating, palpitations Investigations: 24 hour urine collection: ↑ 5 -HIAA levels (serotonin metabolite) CT/MRI to localize tumour. Also consider looking for underlying MEN 1

Questions

SBA A 49 year old woman presents with 4 kg weight loss over 2 months. She complains of feeling hot all the time and her partner mentions that she’s been more irritable recently. On examination she has a smooth goitre, and you also notice proptosis and a rash on her shins. What is the most likely diagnosis? • De Quervain’s thyroiditis • Toxic multinodular goitre • Grave’s disease • Menopause • Medullary thyroid cancer

SBA A 49 year old woman presents with 4 kg weight loss over 2 months. She complains of feeling hot all the time and her partner mentions that she’s been more irritable recently. On examination she has a smooth goitre, and you also notice proptosis and a rash on her shins. What is the most likely diagnosis? • De Quervain’s thyroiditis • Toxic multinodular goitre • Grave’s disease • Menopause • Medullary thyroid cancer

SBA A 16 year old boy presents to the GP with polyuria and polydipsia. He is diagnosed with diabetes insipidus. This condition is characterized by overproduction of which of the following? • Antibodies against insulin-producing beta cells of the pancreas • Anti-diuretic hormone • Brain natriuretic peptide • Oxytocin • Aldosterone

SBA A 16 year old boy presents to the GP with polyuria and polydipsia. He is diagnosed with diabetes insipidus. This condition is characterized by overproduction of which of the following? • Antibodies against insulin-producing beta cells of the pancreas • Anti-diuretic hormone • Brain naturetic peptide • Oxytocin • Aldosterone

SBA A 35 year old female presents with 4 month history of amenorrhoea. On examination, she is noted to have loss of peripheral vision. What is the most likely underlying problem? • Second cranial nerve palsy • Stroke • Hyperparathyroidism • Prolactinoma • Pregnancy

SBA A 35 year old female presents with 4 month history of amenorrhoea. On examination, she is noted to have loss of peripheral vision. What is the most likely underlying problem? • Second cranial nerve palsy • Stroke • Hyperparathyroidism • Prolactinoma • Pregnancy

SBA A 49 year-old man presents with a history of difficulty sleeping. He reports feeling increasingly tired and general weakness which he attributes to his poor sleep pattern. Additionally, the patient has noticed he has gained weight and sweats more easily. On examination, the patient has coarse facial features. What is the most likely diagnosis? • • • Hyperthyroidism Cushing’s disease Acromegaly Hypothyroidism Diabetes

SBA A 49 year-old man presents with a history of difficulty sleeping. He reports feeling increasingly tired and general weakness which he attributes to his poor sleep pattern. Additionally, the patient has noticed he has gained weight and sweats more easily. On examination, the patient has coarse facial features. What is the most likely diagnosis? • • • Hyperthyroidism Cushing’s disease Acromegaly Hypothyroidism Diabetes

SBA A 50 year old Asian man is referred to diabetes clinic after presenting with polyuria and polydipsia. He has a BMI of 30, a blood pressure measurement of 137/88 and a fasting plasma glucose of 7. 7 mmol/L. The most appropriate first-line treatment is: • • • Dietary advice and exercise Sulphonylurea Exenatide Thiazolidinediones Metformin

SBA A 50 year old Asian man is referred to diabetes clinic after presenting with polyuria and polydipsia. He has a BMI of 30, a blood pressure measurement of 137/88 and a fasting plasma glucose of 7. 7 mmol/L. The most appropriate first-line treatment is: • • • Dietary advice and exercise Sulphonylurea Exenatide Thiazolidinediones Metformin

SBA A 15 year old girl complains of headaches which started 6 weeks ago. The headaches initially occurred 1 -2 times a week but now occur up to five times a week, they are not associated with any neurological problems, visual disturbances, nausea or vomiting. The girls also reports a white discharge from both of her nipples. She has not started menstruating. The most appropriate investigation is: • • • Lateral skull X ray CT scan MRI scan Thyroid function tests Serum prolactin measurement

SBA A 15 year old girl complains of headaches which started 6 weeks ago. The headaches initially occurred 1 -2 times a week but now occur up to five times a week, they are not associated with any neurological problems, visual disturbances, nausea or vomiting. The girls also reports a white discharge from both of her nipples. She has not started menstruating. The most appropriate investigation is: • • • Lateral skull X ray CT scan MRI scan Thyroid function tests Serum prolactin measurement

SBA A 58 year old woman presents with an acutely painful neck, the patient has a fever, blood pressure is 135/85, and heart rate is 102 bpm. The patient explains the pain started 2 weeks ago and has gradually become worse. She also experiences palpitations and believes she has lost weight. She presents one week later complaining of intolerance to cold temperatures. What would you see if you performed a radioisotope scan on her? • • • Single area of increased uptake Multiple areas of increased uptake Diffuse increased uptake No uptake She does not need a radioisotope scan

SBA A 58 year old woman presents with an acutely painful neck, the patient has a fever, blood pressure is 135/85, and heart rate is 102 bpm. The patient explains the pain started 2 weeks ago and has gradually become worse. She also experiences palpitations and believes she has lost weight. She presents one week later complaining of intolerance to cold temperatures. What would you see if you performed a radioisotope scan on her? • • • Single area of increased uptake Multiple areas of increased uptake Diffuse increased uptake No uptake She does not need a radioisotope scan

ic_meded Feedback Thank you for listening! Please remember to fill out feedback: https: //forms. gle/up. Bh 6 x. Zj. Qh 43 Fuh. L 6
- Slides: 64