Returning Veterans Traumatic Brain Injury TBI Ellen Crouse
 Ellen Crouse, Ph. D Clinical Neuropsychologist VA")
Returning Veterans & Traumatic Brain Injury (TBI) Ellen Crouse, Ph. D Clinical Neuropsychologist VA Medical Center at Memphis Assistant Professor UT Medical School
 -- Toms River Police say")
SEASIDE PARK, N. J. - September 13, 2013 (WPVI) -- Toms River Police say Officers Brian Jackowski, 39, Chelsea Richard, 26 and Daniel Reale, 19, were hurt Friday morning. It happened around 9: 00 a. m. near Boulevard and N streets. Witnesses say an estimated five or six officers were riding on the back of a truck headed back to the police station. Authorities say a bench in the back snapped off, causing several officers to fall out. "Evidently there was a malfunction with one of our high water vehicles, and the officers fell out of the vehicle onto the roadway, " said Chief Francis Larkin, Seaside Park Police Department. The injured officers, two male and one female, all suffered head injuries.

Medics worked on one officer in a State Police helicopter moments before another victim was loaded inside. Shortly after the chopper took off, another landed. Chief Larkin says all three were conscious and talking at the time of transport. They were taken to Jersey Shore Medical Center. Officer Richard was hurt most seriously. She is hospitalized in critical condition. Officer Reale is hospitalized in serious condition. Officer Jackowski was treated and released from the hospital. Seaside Park resident Robert Rochford saw the group drive by. "That truck was turning around from the saw mill, had all officers on it, I saw the Seaside Park logos, they honked the horn and waved, " said Rochford. (Copyright © 2013 WPVI-TV/DT. All Rights Reserved. )

Objectives • Background Information on TBI • Prevalence, Incidence, and Risk Factors • Veterans and TBI • What might you see? • Alcohol/Drugs & TBI • Veterans with combined TBI & PTSD • Hearing problems in returning Veterans • What is helpful? • Considerations when interacting with Veterans with TBI (with or w/o PTSD)
 is a blow or jolt")
What Is a TBI? • Traumatic Brain Injury (TBI) is a blow or jolt to the head or a penetrating head injury that disrupts the function of the brain • Most blows or jolts to the head do not result in a TBI • Levels of TBI severity: • Mild - brief changes or loss of consciousness (LOC) • Moderate - LOC > 30 min but less 24 hours; skull fracture • Severe - an extended period of LOC or amnesia • TBIs can affect short-term or long-term functioning

TBI in Civilians – USA Annual Stats Each Year • • 1. 5 -2 million Americans sustain a TBI 230, 000 people hospitalized & survive 50, 000 people die from TBI 80, 000 -90, 000 have long-term disability Cumulative Result ~ 5. 3 million people (2% of the U. S. population) live with a permanent TBI-related disability

Annual Incidence of TBI – US Civilians http: //schatz. sju. edu/neuro/epidem/index. html

TBI 101 - Risk Factors for Sustaining a TBI

TBI Risk Factors • Highest risk groups: • Age 0 to 4 years • Adolescents/ young adults ages 15 -19 • Older adults (age 65+) • Risk to males twice the risk among females • TBI is a contributing factor in about 1/3 (30. 5%) of injuryrelated deaths in the US • Adults age 75+ have the highest rates of TBI-related hospitalization and death

Other Risk Factors for TBI § Alcohol/drug use § Unemployment § Familial discord § Low educational status § Psychiatric symptoms § Low SES § Antisocial/Aggressive behavior § Previous head injury § Certain military duties

Causes of TBI in Civilians http: //www. cdc. gov/

TBI in Veterans • Certain military duties increase TBI risk (e. g. , turret gunner, paratrooper, IED hunter) • TBI represents ~ 22% of confirmed injuries in Iraq/Afghanistan War Veterans • Many Veterans have experienced multiple TBI’s due to chronic exposure to blasts • As many as 50% to 60% of Veterans with chronic blast exposure have significant hearing loss or tinnitus (“ringing” in the ears) (Lew, et al. 2007)

TBI in the Military

Not All Veterans are Male 9. 2% of Veterans nationally were female, as of 30 Sep 2014 (VA statistics). In Sep 2014, the State of Tennessee had a total of 506 thousand Veterans. 8. 9% of Tennessee Veterans (45, 000) were female.

§ Over 200, 000 women deployed in OEF/OIF § Women in almost all jobs at all ranks § 1973: Women = 2% of US active-duty force § 2008: Women = 14% of US active-duty force

Mechanisms of TBI Unique to Veterans Traditional Mechanisms vs. Blast vs. Combination

Traditional TBI Mechanism

Coup-Contrecoup Injury • Coup injury: injury occurs at the site of impact with an object • Contrecoup: Contrecoup occurs on the side opposite the area of impact • May see noted as an “accel-decel” injury • Coup and contrecoup injuries are associated with cerebral contusion, which basically means that the brain is bruised

Blast Waves & the Brain “Start by envisioning a bowl of Jello. Tap it on one side and watch how it wiggles all the way over to the other. This mundane image illustrates the force of a blast wave — from a bomb, an improvised explosive device (IED), a mine, grenade or mortar shell — traveling through brain matter, disrupting pathways and unleashing a chemical soup on its victim. ” ~ Jonathan Fellus, MD Director of Brain Injury Services, Kessler Institute of Rehabilitation

What Happens in an Explosion + -

Blast Injury Types Primary – Unique to blasts, results from impact of the over-pressurization wave on the body

Blast Injury Types Secondary – Results from flying debris & bomb fragments

Blast Injury Types Tertiary – Results from people being thrown into other objects by a blast

Blast Injury Types Quaternary – Injuries, illnesses, or diseases not due to primary, secondary, or tertiary causes. Includes complications of existing conditions.

What Problems Might You See in Veterans with TBI?
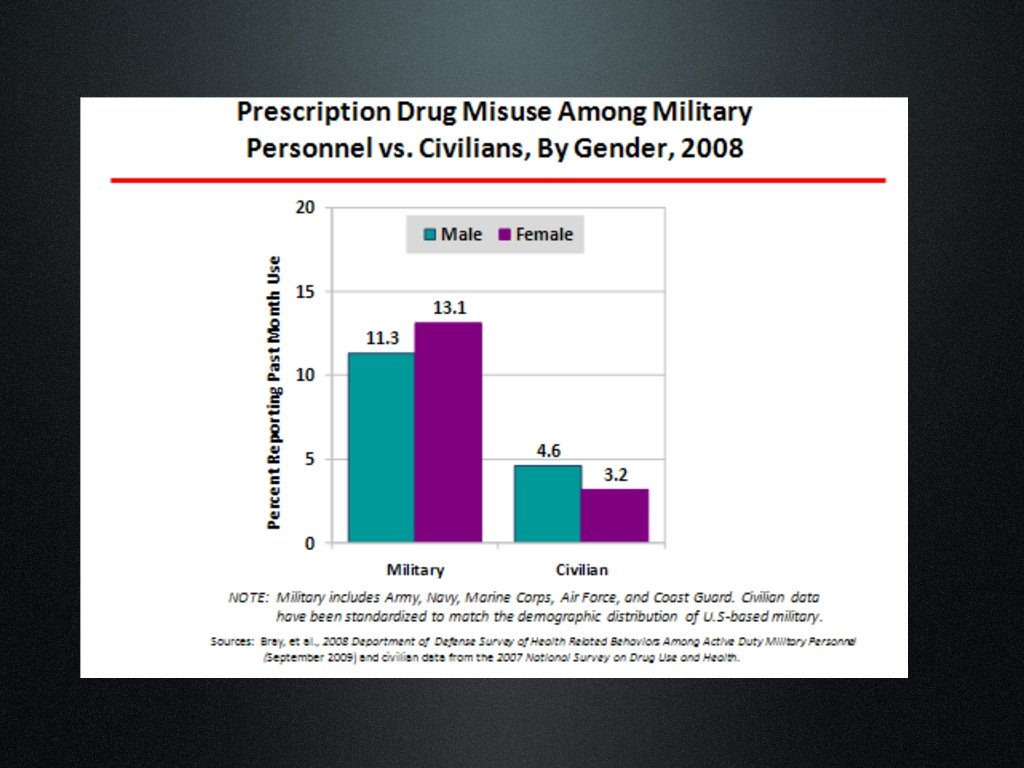
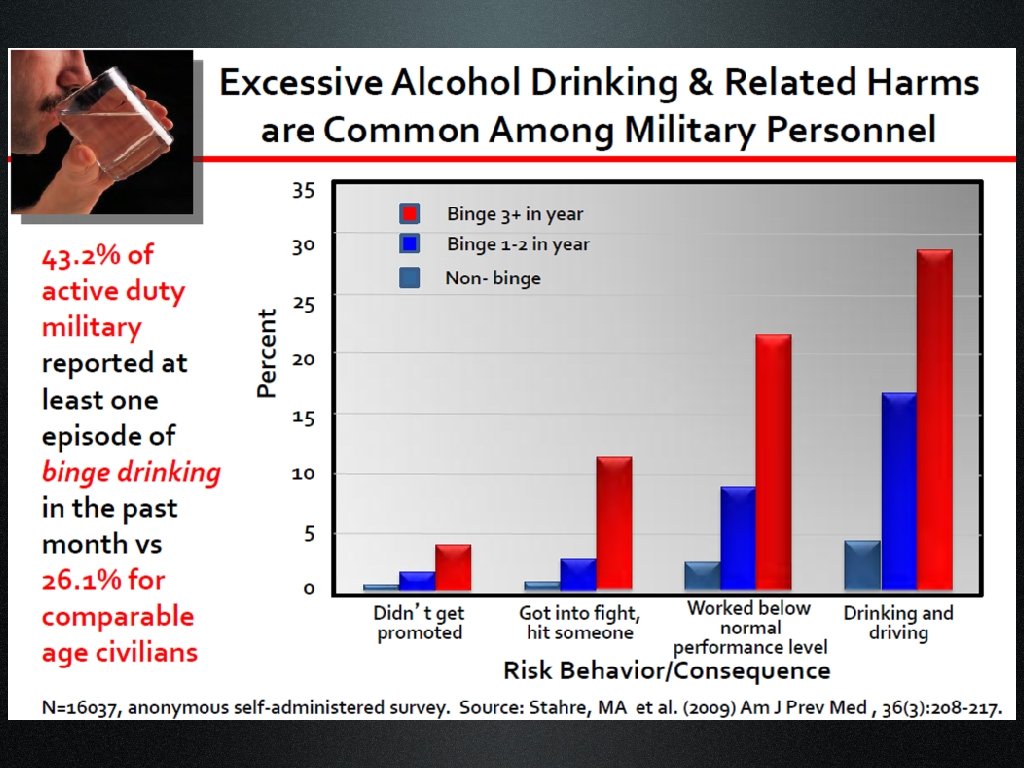

Reported Prevalence of History of Alcohol Dependence Patients with TBI: Ranges from 25% to 68% General Population: Alcohol 15%, Drug Addiction 9%-20% Slide courtesy of L. Brenner
")
TBI Sequelae (then what happens? )

Possible TBI Presentations • • • Impaired Judgment Impatience Restlessness Confusion Poor Emotional Control • Slow Processing • Aggressiveness • Suspiciousness or paranoia • Impulsiveness • Impaired attention • Anxiety • Depression

Attention Problems TBI Depression Irritability Headache Nausea & Vomiting Hearing Loss Sleep Problems Ringing in Ears Dizziness Poor Anger Control Anxiety

PTSD Attention Problems Flashbacks Depression Nightmares Irritability Sleep Problems Poor Anger Control Anxiety Isolates Self Easily Startled

PTSD Attention Problems TBI Flashbacks Depression Headache Nausea & Vomiting Hearing Loss Nightmares Irritability Sleep Problems Ringing in Ears Dizziness Poor Anger Control Anxiety Isolates Self Easily Startled
")
MENTAL HEALTH PROBLEMS IN VETERANS ~ Hoge (2004)

“MH” = PTSD or Depression ~ Rand Corporation 2008

Sleep, TBI, & PTSD § Disruptions of the sleep cycle and pattern are common after TBI. § People with PTSD may have frequent nightmares and/or may be chronically sleep-deprived.

TBI & Suicide - Civilian Suicidal Thoughts: • 23% of TBI sample endorsed clinically significant suicidal ideation, compared to 3. 5% in community sample (Kienhorst et al. , 1990) Suicide Attempts: • In a community sample, people with TBI reported higher frequency of suicide attempts than those without TBI (8. 1% vs. 1. 9%). • Difference present even after adjusting for sociodemographic factors, quality of life, & presence of co-existing psychiatric disorder (Silver et al. 2001)
: • In a sample")
TBI & Suicide - Civilian Role of Substance Abuse (SAb): • In a sample of TBI pts, a history of pre-TBI SAb was significantly higher in those who committed suicide than in the group that did not (Achte, et al. , 1975) • Teasdale & Enberg (2001) found that co-morbid diagnosis of Sab disorder + TBI at time of admission was associated with a much greater risk for subsequent suicide than TBI alone. Role of Sleep: • Poor sleep quality has recently been linked to increased risk for suicide (Wojnar, et al. , 2009)

Social Issues in TBI & PTSD § High rates of unemployment in returning (especially younger) Veterans § Work/financial stress in TBI and PTSD § Disrupted social functioning § Increased caregiver burden and changes in marital relationship/roles

Hearing Loss in Veterans • Tinnitus: the false perception of sound in the absence of acoustic stimulus; a phantom noise (aka, “ringing” ears) • As many as 50% to 60% of Veterans with chronic blast exposure have significant hearing loss or tinnitus (Lew, et al. 2007). • Hearing loss and tinnitus are the most common medical issues faced by OEF/OIF Veterans.

Possible Effects of Hearing Loss / Tinnitus EMOTIONAL EFFECTS Mood Problems Anxiety Frustration Anger Irritability Helplessness EFFECTS ON LIFESTYLE Misunderstandings (relationships and work) Avoidance of pleasant events/activities Disturbed sleep Communication difficulties

What is Most Helpful When Interacting with Veterans with TBI?

Slowed Processing Speed • Be patient and maintain a calm attitude. • Recognize that thinking more slowly does not equal lower intelligence. • Speak more slowly, with slightly longer pauses than usual. • Allow extra time for Veteran to respond.

Impaired Attention • Decrease environmental stimuli when possible. Take Veteran to quiet area to talk. • Consider asking Veteran to state back what you’ve said in his/her own words. • Allow breaks in longer conversations for Veteran to get up and stretch.

Impaired Working Memory • Try not to say too much at once. Break down what you want the vet to remember into smaller parts. • Be very organized in what you say and ask. • Recognize that you may need to repeat information. • Consider asking Veteran to state back what you’ve said in his/her own words.

Difficulty with Problem-Solving • Offer options rather than expecting Veteran to generate solutions. • Minimize distractions in the environment. • Walk Veteran through the problem and assist in breaking it down into smaller components. • Allow time to think.

“Yo-Yo” Emotions and/or Aggressiveness • Create as calm an environment as possible. • Slow your own speech and project a sense of calmness. • Assess potential for suicide or assault. • Ask Veteran what (if anything) has been helpful in the past. Encourage that tactic if it is safe. • Consider need for transfer to VA.

Hearing Impairments • Ask if Veteran can hear you well. • Face Veteran when talking with him/her. • May need to use large gestures to get Veteran’s attention from a distance. Don’t depend on shouting. • Recognize that some people with new hearing problems are more prone to suspiciousness. (Imagine if everyone around you was whispering. ) • Be more careful about speaking slowly & clearly.

Final Thought It is not always apparent that someone has a TBI history. Best to simply use these strategies whenever you can.

Thank You for your service to our communities and to our Veterans!!
- Slides: 50