Resuscitation in sepsis Which hemodynamic targets and how



")







 Design of MAP")


")





 vs. No. A")
")




")



")

")





")



- Slides: 48
Resuscitation in sepsis. Which hemodynamic targets and how to achieve them Pierre Asfar
Septic shock Hypovolemia Vasopressors - Norepinephrine - Epinephrine - Vasopressin - Angiotensin II ↓ peripheral venous tone ↑ microvascular permeability Volume expansion Inotropes -Dobutamine -Levosimendan - IPDE -Norepinephrine -Epinephrine Hypotension Vascular failure ↓ vasoconstrictor tone ↓ vasopressor response Myocardial Failure ↓ myocardial contractility
Shock states: Hemodynamic targets. • Correction of organ perfusion pressures – Fluids, vasopressors. • Maintain or increase (optimize? ) DO 2 – Oxygen, fluids, transfusions, inotropes. • Improvement of local or regional hemodynamics (splanchnic, renal etc)?
Resuscitation of circulatory shock should be guided by. . . arterial pressure (? ) WHY?
Rhodes et al: Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock. ICM 2017; 43: 304 ". . . We recommend an initial target mean arterial pressure (MAP) of 65 mm. Hg in patients with septic shock. . . " "…(strong recommendation, moderate quality of evidence)…"
Low perfusion pressure Excessive vasoconstriction
Retrospectives studies
111 patients No. of periods MAP < 65 mm Hg mortality
274 patients No. of periods MAP < 60 mm Hg mortality MAP improved kidney function?
Dünser et al: Association of arterial blood pressure and vasopressor load with septic shock mortality: a post hoc analysis of a multicenter trial. Crit Care 2009; 13: R 181 290 patients
Prospective Studies
Prospectives studies: Short-term design, small no. of patients study Patients (n) Design of MAP titration mm Hg Measures Results Ledoux (10) CCM 2000 65, 75, 85 (105’) Hemo, tono, LD, rénal function I C remaining NS Bourgoin (2 x 14) CCM 2005 MAP 65 vs 85 (4 h) Hemo, renal function CI Renal function NS 65, 75, 85 (120’) Hémo, renal function, RRI 65 -75 mm Hg, urine output, RRI 60, 70, 80, 90 (45’) Hemo, Pt. O 2, LD, SDF DO 2, Pt. O 2 LD, SDF ns Dubin (20) CC 2009 65, 75, 85 (30’) Hemo, tono, SDF CI, DO 2 ns, Tono ns, SDF ns Thooft (13) CC 2011 65, 75, 85 (30’) Hemo, St. O 2, SDF CI, St. O 2, SDF R A E L C O Deruddre (11) ICM 2007 Jhanji (16) CCM 2009 N R E W S AN Hemo: hemodynamics. Tono: tonometry. RRI: renal resistance index. Pt. O 2: cutaneous Pt. O 2. SDF: sidestream darkfield imaging
423 patients: 153 with vs. 270 without progression of AKI Predicting factors: CKD, hypotension/hypovolemia, contrast dye prior to ICU, MV, vasopressors, furosemide, steroids
Multicenter-Trials? No answer!
Resuscitation of circulatory shock should be guided by. . . arterial pressure (? ) Real life practice?
Rivers, et al: Early goal-directed therapy in the treatment of severe sepsis and septic shock. NEJM 2001; 345: 1368
Asfar et al: High versus Low Blood Pressure Target in Patients with Septic Shock. NEJM 2014; 370: 1583 RCT; 776 patients; target MAP 65 -70 vs. 80 -85 mm. Hg Target MAP 65 -70 mm. Hg
CATS Annane Lancet 2007 VASST Russell NEJM 2008 SOAP 2 study De Backer NEJM 2010
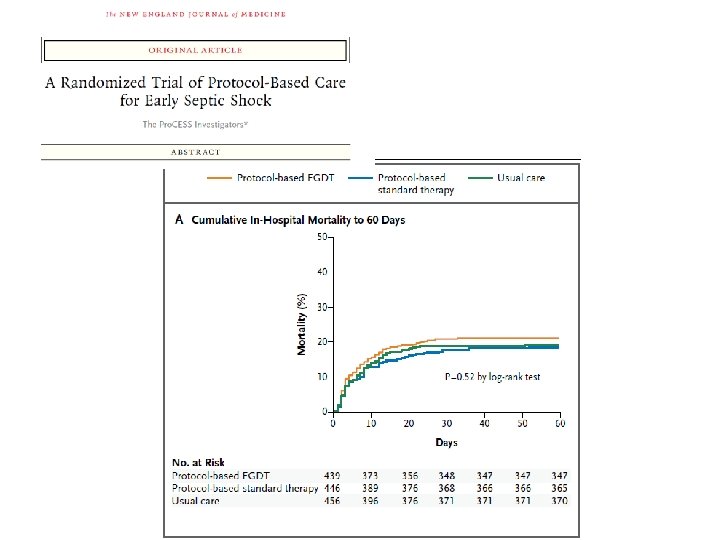
Pro. CESS investigators: A randomized trial of protocol-based care for early septic shock. NEJM 2014; 370: 1683 MAP mm. Hg Start 6 h Protocol-based EGDT 65 77 79 ± 84 ± 86 ± ± 16 ± Protocol-based standard therapy 66 79 80 ± 85 ± 86 ± ± 17 ± 15 Usual care 65 76 78 ± 84 ± 86 ± ± 16 ± 14 13 24 h 14 15 14 48 h 14 16 15 72 h 15 15 16
Pro. CESS investigators: A randomized trial of protocol-based care for early septic shock. NEJM 2014; 370: 1683 MAP mm. Hg Start 6 h Protocol-based EGDT 65 77 79 ± 84 ± 86 ± ± 16 ± Protocol-based standard therapy 66 79 80 ± 85 ± 86 ± ± 17 ± 15 Usual care 65 76 78 ± 84 ± 86 ± ± 16 ± 14 13 24 h 14 15 14 48 h 14 16 15 72 h 15 15 16
Lopez et al: CCM 2004; 32: 21 NO inhibitor (LNMA) vs. No. A
Resuscitation of circulatory shock should be guided by. . . arterial pressure (? ) WHICH?
Asfar et al: High versus Low Blood Pressure Target in Patients with Septic Shock. NEJM 2014; 370: 1583 RCT; 776 patients; target MAP 65 -70 vs. 80 -85 mm. Hg
Asfar et al: High versus Low Blood Pressure Target in Patients with Septic Shock. NEJM 2014; 370: 1583 RCT; 776 patients; target MAP 65 -70 vs. 80 -85 mm. Hg
Lamontagne et al: Pooled analysis of higher versus lower pressure targets for vasopressor therapy septic and vasodilatory shock. ICM 2018; 44: 12 894 patients (pooled OVATION/SEPSISPAM) SEPSISPAM (274/776) OVATION (35/118) Hypertension Yes (139/393) No (170/501) Congestive heart failure Yes (55/122) No (254/772) Hours on vasopressor < 6 (271/769) > 6 (38/122) Odds ratio 0. 2 0. 5 Favors higher 1. 0 2. 0 lower target 5. 0 10. 0
Maheshwari et al: The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. ICM 2018; 44: 857 Retrospective; 8, 782 patients (6 years) 1. 2 Odds Ratio 1. 1 1. 0 55 65 75 85 Mortality 55 65 75 85 AKI 55 65 75 MI 85 mm. Hg MAP thresholds
Resuscitation of circulatory shock should be guided by. . . arterial pressure (? ) SIDE EFFECTS?
Asfar et al: High versus Low Blood Pressure Target in Patients with Septic Shock. NEJM 2014; 370: 1583 RCT; 776 patients; target MAP 65 -70 vs. 80 -85 mm. Hg 65 -70 mm Hg Catecholamine infusion rate (mg/h) 80 -85 mm Hg 0. 50 ± 0. 07 0. 71 ± 0. 08 p value 0. 037 Catecholamine infusion duration (d) 3. 7 ± 3. 2 4. 7 ± 3. 7 <0. 0001 Total fluid loading (L) 2. 7 ± 3. 2 2. 7 ± 3. 7 0. 9 Daily urine output (L) 1. 4 ± 1. 3 0. 8
Asfar et al: High versus Low Blood Pressure Target in Patients with Septic Shock. NEJM 2014; 370: 1583 RCT; 776 patients; target MAP 65 -70 vs. 80 -85 mm. Hg Low MAP High MAP p value 69 (17. 8%) 74 (19. 1%) 0. 64 19 (4. 9%) 35 (9%) 0. 034 AMI 2 (0. 5%) 7 (1. 8%) 0. 18 AF 11 (2. 8%) 26 (6. 7%) 0. 017 VT/VF 15 (3. 9%) 22 (5. 7%) 0. 24 All ischemic side effects 53 (13. 7%) 44 (11. 4%) 0. 39 Bleedings 42 (10. 8%) 31 (8%) 0. 22 Mesenteric ischemia 9 (2. 3%) 1 Digital ischemia 9 (2. 3%) 10 (2. 6%) 0. 82 All side effects All cardiac side effects
Pearce RM: Experimental myocarditis; a study of the histological changes following intra-venous injections of adrenalin. J Exp Med 1906; 8: 400 -409 Chappel CJ et al: Comparison of cardiotoxic actions of certain sympathomimetic amines. Can J Biochem Physiol 1959; 37: 35 -42 Schmittinger CA et al: Histologic pathologies of the myocardium in septic shock: A prospective observational study. Shock 2013; 39: 329 -35 20 patients dying from septic shock-induced cardiovascular failure; histological findings directly related to No. A, Epi-dose!! Contraction band necrosis Mononuclear infiltrates
Resuscitation of circulatory shock should be guided by. . . arterial pressure (? ) Organ specific?
Asfar et al: High versus Low Blood Pressure Target in Patients with Septic Shock. NEJM 2014; 370: 1583 RCT; 776 patients; target MAP 65 -70 vs. 80 -85 mm. Hg Doubling of plasma creatinine (All) — no. (%) No chronic hypertension — no. (%) Chronic hypertension — no. (%) RRT from Day 1 to Day 7 (All) — no. (%) No chronic hypertension — no. (%) Chronic hypertension — no. (%) Low MAP High MAP P value 161 (41. 5) 150 (38. 7) 0. 42 71 (33. 0) 85 (38. 5) 0. 32 90 (52. 0) 65 (38. 9) 0. 02 139 (35. 8) 130 (33. 5) 0. 5 66 (30. 7) 77 (34. 8) 0. 36 73 (42. 2) 53 (31. 7) 0. 046
Resuscitation of circulatory shock should be guided by. . . arterial pressure (? ) Rhodes et al: Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock. ICM 2017; 43: 304 ". . . When a better understanding of any patient’s condition is obtained, this target should be individualized. . . " individualized
Crit Care Med 2013; 41: 580
Crit Care Med 2013; 41: 580
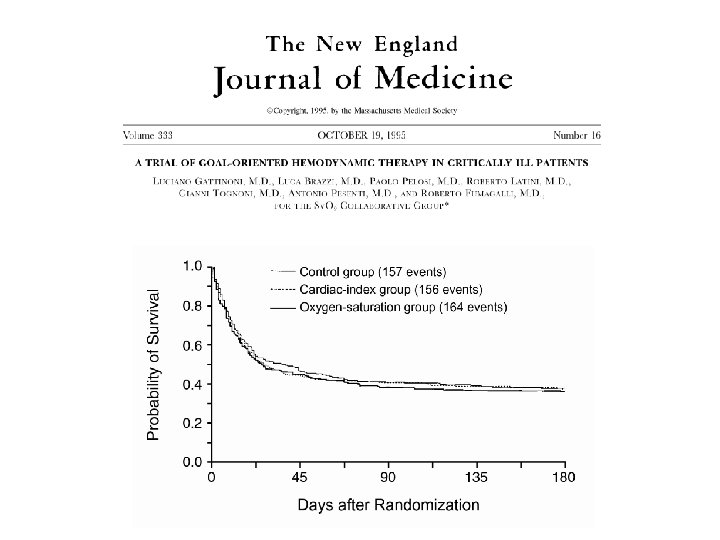
Patients were randomly assigned to one of three treatments designed to achieve different hemodynamic goals: - a “normal” cardiac index (2. 5 - 3. 5 L min-1 m-2) - a “supranormal” cardiac index (> 4. 5 L min-1 m-2) - a “normal” Sv. O 2 >70%
Baseline-characteristics of the patients Characteristics during the five-day study period
JF Pope Ann Emerg Med 2010; 55: 40 -46
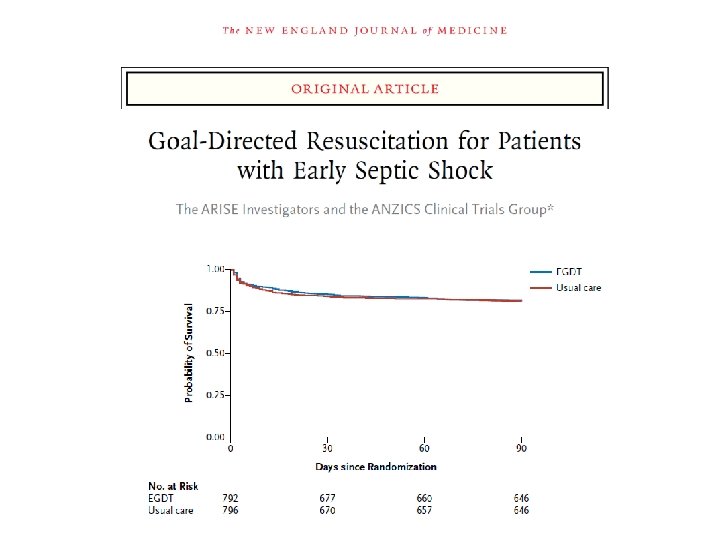
ARISE: Central venous oxygen saturation (Sc. VO 2)
363 patients en sepsis ou choc septique 111 patients avaient une Scv. O 2 initiale <70%
2010; 303: 739
Shock states: Hemodynamic targets. • Correction of organ perfusion pressures – Fluids, vasopressors. – Target > 65 mm Hg according patients features • Maintain or increase (optimize? ) DO 2 – Oxygen, fluids, transfusions, inotropes. – The best tool is Sv. O 2 or Sc. VO 2 measurements