Results and Reporting The Wessex Experience Ellen Copson




















- Slides: 21
Results and Reporting: The Wessex Experience Ellen Copson Emily Shaw June 2018
Issues considered when designing Wessex cancer results pathway • Need to review technical as well as biological aspects of sequencing results • Need to verify somatic results depends on “actionable” status entirely dependent on clinical status of pt • Clinical genetics expertise required for germline findings • Multi-disciplinary discussion required but different skillset to current cancer (site specific) MDTs • Not feasible to add this discussion into current MDTs – Multiple tumour sites – job plan issues – Time pressures of current MDTs (UHS breast MDT 102 patients in 3 hrs!) • Need to engage effectively with oncologists
Wessex Molecular Tumour Board • To review, analyse and interpret results from next generation sequencing of DNA/RNA derived from solid tumour samples • Providing responsible oncologist and site specific MDT with interpretation of NGS finding and, where appropriate, suggesting possible clinical consequences • Meeting weekly since Dec ‘ 17 Genomic Oncologist Genomic Cellular Pathologist Molecular Pathologist Genomic technician Clinical geneticist Site specific oncologist Biomedical scientist Oncology and pathology trainees Terms of reference • Advisory role • Membership of board • Reporting activity to genomic strategy board • Confidentiality and information governance • Educational role
MTB Documentationa Proforma • • Date of meeting and staff present Patient identifiers and current clinical situation Responsible consultant and date/ location of next appointment Date of report and version no of WGS report Review of technical aspects of sequencing Comparison to standard of care test results Other potentially ‘actionable’ results – e. g. clinical trial eligibility, CDF or compassionate use therapies • Further action required, person responsible and target date • Recently reviewed and updated based on experience so far
Wessex Cancer Programme Results Pathway Pre Meeting Preparation Weekly MTB Meeting Pt list circulated Molecular Tumour Board Genomic Oncologist Contacts clinical team to ascertain pt. status Reviews technical, somatic and germline data Correlate with clinical status Germline mutation of clinical significance -Provides recommendation for referral to clinical genetics for validation testing Somatic mutation of clinical significance -confirms if “actionable” -refers for validation testing Biomedical scientist reviews NGS results & searches literature Completes summary report- stored in electronic pt. record Validation testing - formal pathology report issued Clinical Interface Site specific MDT Review summary report and recommend any changes to pt. management Responsible Clinician Informs patient of results and confirms ongoing management Refers to clinical genetics if recommended Clinical Genetics Review pt. & requests germline validation
Reporting back • Selected cases only so far: – Issues with patient identifiers – Closed correspondance with responsible clinicians • Electronic version of MTB proforma and letters to be piloted within next few weeks • Series of meetings with MDT co-odinators and leads in progress to introduce pathway • Monthly updates on project to oncology consultant meetings
Experience to date • 212 results received so far • 115 cases reviewed in MTAB • no changes to patient care – Time from diagnosis to results 1 -2 years – Many patients deceased – Most completed treatment for primary cancer – SOC tests done at point of diagnosis – Clinical trial tests returned rapidly – Very limited availability to targeted therapies if not NICE approved/ CDF or via clinical trials • 1 case to be validated • 1 fast track case – Neuroblastoma in child diagnosed with germline KDM 5 B mutation in RD programme – No actionable somatic mutations
MTAB and Reporting of 100 KGP Results • Highly educational • + time consuming – Pre-meeting preparation clinical and mol path – 1 hour weekly meeting – Clinical follow-up: letters/ emails/ tracing of patients • Needs to be adopted into relevant job plans – Funding an issue from 1 st Oct 18…. .
Current Challenges • Change in process for issuing cancer reports – Reports now sorted by Illumina number • Cancer report re-issues • Cancer portal feedback format • BSVI: software issues
Molecular tumour board case study Dr Emily Shaw Consultant Cellular Pathologist University Hospital Southampton NHS Foundation Trust/ Wessex GMC
Molecular tumour board case study Dr Emily Shaw Consultant Cellular Pathologist University Hospital Southampton NHS Foundation Trust/ Wessex GMC
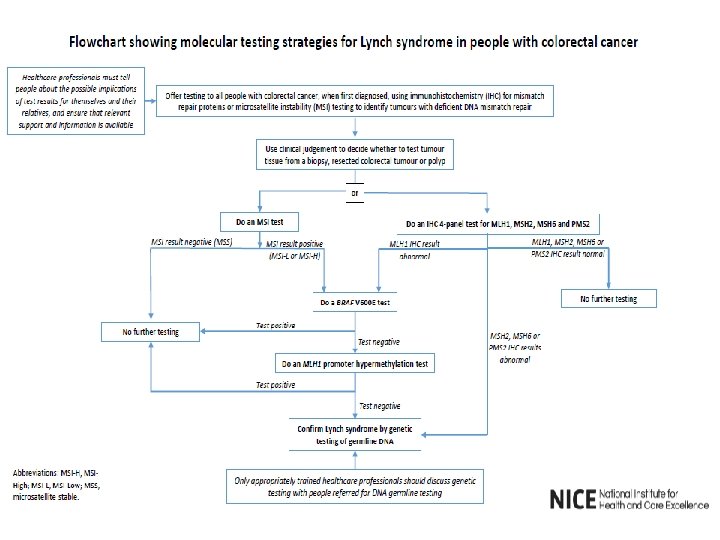
Clinical details • 74 year old female presenting with abdominal pain and change in bowel habit, March 2016 • Probable tumour identified in caecum on CT colonography and biopsied at colonoscopy • Resected Nov 2016: p. T 3 p. N 0 (Dukes B) mucinous adenocarcinoma • Mismatch repair deficiency on immunohistochemistry: loss of MLH 1 and PMS 2 protein expression
DNA mismatch repair protein function http: //www. jimmunol. org/content/jimmunol/162/6/3121/F 1. large. jpg
Further investigations • Referred to clinical genetics for investigation of possible underlying Lynch Syndrome • FH: – sister hysterectomy for cancer – maternal: mother diagnosed with bowel cancer aged 67 – paternal: uncles and grandmother cancer ? type, grandfather melanoma, cousin stomach cancer – son melanoma aged 42, daughter breast cancer • Germline mutation analysis negative
Whole genome analysis
Distribution of SNVs
Domain 1 gene variants ATRX FANCE NTRK 1 MCPH 1 MLH 1 x 2 MLH 3 FGFR 3 PPP 2 R 1 A FGF 18 ATM ATR RICTOR RNF 43 x 2 MET SLX 4 MDM 2 FANCA x 2 BRAF x 2 WNT 5 A MSH 2 MSH 3 MSH 6 PMS 1 x 2 PMS 2 RAD 50 CTNNA 2 RPTOR x 2 ROS 1 SMARCB 1 TSC 2 x 2 FGF 7 FGF 22 x 3 ALK + variants in 117 domain 2 genes
Mutational signatures Deficient DNA mismatch repair
Molecular tumour board interpretation • Sporadic colorectal adenocarcinoma with acquired microsatellite instability/ DNA mismatch repair deficiency • Clinical features consistent: female gender, older age, right colon, high grade, mucinous differentiation • WGA findings supportive: BRAF V 600 E mutation (to be validated) and no pertinent germline mutations in cancer predisposition genes • MSI favourable prognostic factor in early stage disease: longer disease-free/ overall survival
Emily Shaw Liz Hodges Ros Ganderton Nicola Meakin Chris Mattocks Diana Eccles Steve Docherty James Bennett Karen Temple Tony Williams Catherine Mercer Ryan Beegan Kathy Bovey Ben Johnson Jane Dare Lucy Hogan Angie Blackmore Carine Fixmer Omer Ahmed Phillandra Costello Dale Seviar Nadia Peppa Maria Lane Amicha Alfonso Hannah Markham Victoria Elliott