Restoration of acquired defects of hard palate in
























 If the defect is small and remaining teeth are stable, intra coronal retainer")


 Residual soft palate � Provides posterior palatal seal and minimizes passage of food")
 Residual Hard Palate � Under cuts along the line of palatal resection into,")
 Lateral Scar Band �For adequate surgical closure, most maxillary resections are lined with")
 Height of lateral wall �Engaging lateral wall of defect provides indirect retention. �Longer")













































- Slides: 81
Restoration of acquired defects of hard palate in dentate patients Part II Hemant Jivnani JR II
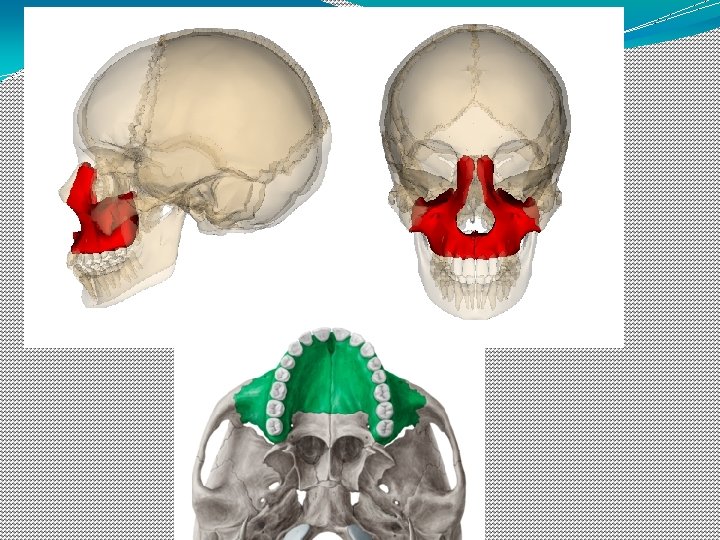
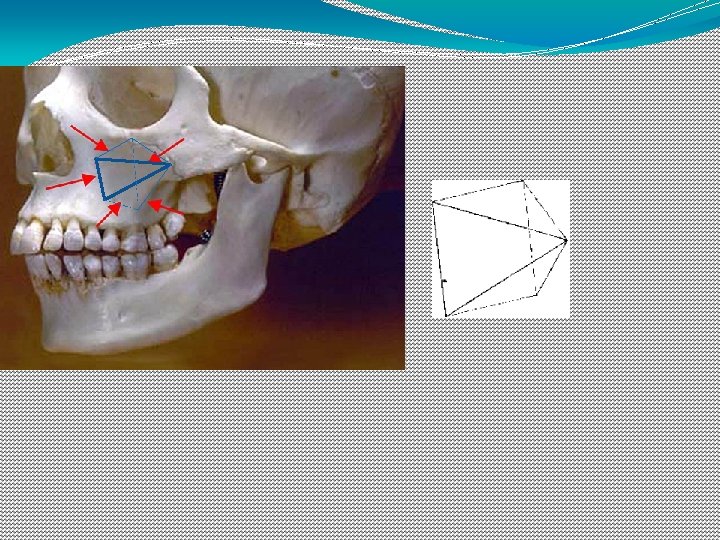
Brief anatomy of the maxilla, the palate and the maxillary sinus
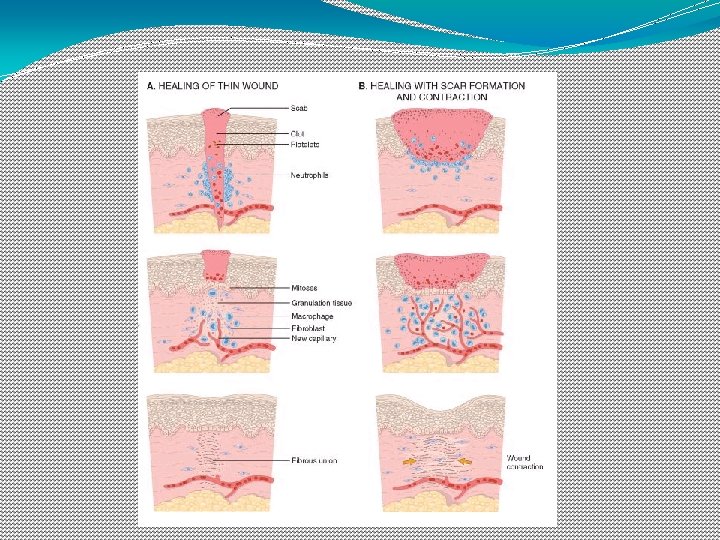
How are Scars and scar contractures different?
Surgical considerations
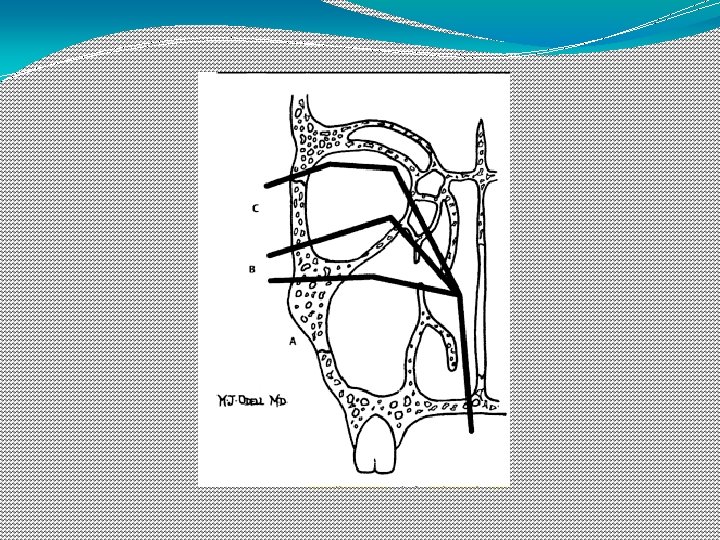
Maxillectomy �Several different subtypes of maxillectomy have been described and due to the use of many terms like radical, total, subtotal, limited, partial, medial, extended maxillectomies; there has been a confusion regarding the nomenclature. �Maxillectomies can be classified according to spiro et al. based on the number of walls as �Limited: one wall �Subtotal: at least two walls including the palate �Total : resection of the entire maxilla
Brown’s classification
Surgeon should be advised the following considerations.
�Line the reflected cheek flap with a split-thickness skin graft
�If the wound is allowed to epithelialize spontaneously, it results in formation of poorly keratinized epithelium or respiratory epithelium which can not be utilized to obtain support, retention or stability for the obturator. While lining the defect with skin graft provides a highly keratinized surface that can be used to obtain support and retention for the obturator prosthesis on the defect side.
�Provide superior and lateral access to the defect
�To remove the entire soft palate if less than one-third of the posterior aspect of the soft palate is to remain post surgically. (unless the patient is edentulous)
�Imbibing the residual fibers of the levator veli palatini muscle within the lateral wall of the pharynx can enhance the residual velopharyngeal mechanism and an obturator can aid it to achieve velopharyngeal closure during swallowing along with a decreased hypernasality in speech.
�Retain Premaxillary Segment
�Save some of the palatal mucosa normally included in the resection and use it to cover cut medial bone margin of the palatal bones. Bony cut Palatal incision
CONSIDERATON IN OBTURATOR PROSTHESIS DESIGN
�The need for support, retention and stability in designating any prosthesis should be understood if the objective of prosthodontic care to be attained. �For the patient with an acquired maxillary defect it is often necessary to modify, and sometimes violate, some of the basic principles of prosthesis design because of the basic nature of the defect. �The remaining structure are most often unilateral, thus encouraging movement of the prosthesis with associated stress directed to these remaining structures.
�The frequent location of unilateral remaining structures suggests that the obturator portion of the prosthesis, in addition to the residual structures, must contribute significantly to the support, retention, and stability of the prosthesis to satisfy the basic prosthodontic objectives.
SUPPORT �Support is the resistance to movement of a prosthesis toward the tissue. The support available from the residual maxilla and from within the defect both must be considered. Residual maxilla support �In the residual maxilla the primary areas available for support are the residual teeth, the alveolar ridge and the residual hard palate.
A. Residual teeth � Carious involvement of the remaining teeth should be treated and their periodontal status made optimal. � Support is also provided by the placement of occlusal rests, cingulum rest and incisal rest. � Maximum effort should be directed toward saving as many teeth as possible without compromising the tumor resection protocol.
Within-the-defect support � Positive support within the defect to prevent rotation of the prosthesis into it must be considered. This support can be achieved by contact of the prosthesis with any anatomic structures that provides a firm base. � In most acquired maxillary defects the floor of the orbit, the bony structures of the pterygoid plate, and the anterior surface of the temporal bone near the infratemporal fossa are considered for positive support.
a. Floor of the Orbit � Use of the floor of the orbit for support should be minimal. It cannot be used for support, if orbital floor has been removed then the orbital contents will move with the movement of the prosthesis. Drawbacks: � If prosthesis is extended up to the orbital floor it would make insertion through the oral opening difficult, unless a two piece sectional prosthesis is used. � Additional weight � Problems of fabrication � Alteration in speech quality due to too much obturation of the resonating chamber.
b. Pterygoid Plate or Temporal Bone � Positive contact of the prosthesis with this bony structure can be relatively extensive and adequate to tripod the support for an obturator prosthesis.
c. The Nasal Septum It is a poor support for extensive prosthesis because, � It is partly cartilage � Has little bearing area � Is covered with nasal epithelium.
RETENTION Retention is the resistance to vertical displacement of the prosthesis. � Retention is provided by A. Within the residual maxilla B. Within the defect A. Residual Maxilla Retention-is provided by teeth in a dentate patient. � If the defect is small and remaining teeth are stable, intra coronal retainer can be used. ii) If the defect is large and all teeth are weak, extra coronal retainers should be used.
i) If the defect is small and remaining teeth are stable, intra coronal retainer can be used. ii) If the defect is large and some or all teeth are weak, extra coronal retainers should be used.
B. Within the defect retention � Retention of an obturator prosthesis cannot be totally and adequately provided by the residual maxillary structures in either the edentulous or the dentulous patient unless the defect in exceptionally small. � Large defects that approach the extent of the hemimaxillectomy must contribute intrinsically to the retention of the obturator prosthesis if the objectives of prosthesis design and prosthodontic care to be achieved.
�If the obturator extension itself could minimize the vertical displacement of the prosthesis, less stress would be generated to the residual maxillary structures. The following structures should be considered for retention within the defect. a) Residual soft palate b) Residual hard palate c) Anterior nasal aperture d) Lateral scar band e) Height of lateral wall
a) Residual soft palate � Provides posterior palatal seal and minimizes passage of food and liquid above the prosthesis. � Extension of the obturator prosthesis onto the nasopharyngeal side of the soft palate provides retention.
B) Residual Hard Palate � Under cuts along the line of palatal resection into, nasal or para nasal cavity or medial wall of defect can increase retention. � Obturator extension into the undercut is best provided by a soft denture base material. � The extension shouldn’t contact the nasal septum or the turbinates
C) Lateral Scar Band �For adequate surgical closure, most maxillary resections are lined with split – thickness skin graft along the anterior lateral and postero – lateral walls of defects. �This results in the formation of scar band which is more prominent in laterally and postero – laterally as compared to scar band anterior to premolar region. �These act as good undercuts for retention.
D) Height of lateral wall �Engaging lateral wall of defect provides indirect retention. �Longer radius undergoes less vertical displacement than the shorter radius.
STABILITY �Stability is the resistance to prosthesis displacement by functional forces. �Because function tends to move an obturator prosthesis, the principles of obturator design that minimize rotation around the horizontal plane and minimize movement within the horizontal plane itself must be considered. �Rotation of the prosthesis around the horizontal plane is that rotation seen around the fulcrum line. Many aspects of obturator design are important to both retention and stability.
�Movement of the prosthesis within the horizontal plane can be anteroposterior, mediolateral, rotational, or a combination of any or all of these directions. As with retention and support specific areas of the residual maxilla, as well as the defect itself, must be considered in minimizing the extent of these potential movements. Residual maxilla �If natural teeth remain, the bracing components of the prosthesis framework can be used to minimize movement in all three directions.
It is advantageous to provide maximal bracing and to extend this bracing interproximally when possible to minimize rotational as well as anteroposterior movement of the prosthesis.
Within the defect stability �The defect itself must be considered to enhance the stability of an obturator prosthesis. �Maximal extension of the prosthesis in all lateral directions must be provided. �Special emphasis must be placed on maximal contact with the medial line of resection, the anterior and lateral walls of the defect, the pterygoid plates, and the residual soft palate. �Contact of the obturator portion of the prosthesis with these structures minimizes anteroposterior, mediolateral and rotational movement of the prosthesis.
Occlusion �Occlusion is a very important aspect for stability of the prosthesis. an unstable prosthesis is the result if the occlusal relationship fails to maintain intimate contact of the prosthesis with the supporting and the retentive structures. �To minimize the movement of the prosthesis, maximum distribution of occlusal forces is essential. �Mastication over the defect should be avoided.
Purpose of the prosthetic dentition on defect side: �Esthetic display �Lip support �Prevent opposing dentition from super-erupting Occlusal scheme �Centric only contact on the defect side is preferred. �Lateral interferences should be removed.
General considerations concerning the bulb design �A bulb is not necessary �Small to average size defect �Surgical or immediate temporary prosthesis �Need of hollow �To aid in speech resonance �Light weight
�It should not be high as to cause the eye to move during mastication �It should be closed superiorly always �It should not be large as to interfere with insertion if the mouth opening is restricted.
Principles of framework design for obturator prosthesis
General requirements of the framework design for obturator prosthesis, similar to that of a conventional removable partial denture � A rigid major connector. �Guide planes and other components that facilitate stability and bracing �Rests that place supporting forces along the long axis of the abutment tooth
�Direct retainers that are passive at rest and provide adequate resistance to dislodgment without overloading the abutment teeth �Control of the occlusal plane that opposes the defect, especially when it involves natural teeth.
Unique considerations of the obturator framework �The location and size of the defect, especially as it relates to the remaining teeth. �The importance of the abutment tooth adjacent to the defect, which is critical to the support and retention of the obturator prosthesis. �The usefulness of the lateral scar band, which flexes to allow insertion of the prosthesis but tends to resist its displacement and �The use of the surveyor to examine the defect for the purpose of locating and preserving useful undercuts or eliminating undesirable undercuts.
Class 1 - curved arch from �Tripodal design is recommended if the anterior teeth are to be used for support or retention �Linear design is recommended if the anterior teeth are not to be used for support or retention. Support for the prosthesis can be derived from: the remaining teeth, the residual palate, and the structures in the defect that may be contacted.
�Rests: on most anterior and the mesiocclusal surface of the most distal abutment tooth when alignment and occlusion will permit. �The mesiocclusal posterior rest, most often located between adjacent posterior teeth, is accompanied by a rest on the distoocclusal surface of the more anterior adjacent tooth. �Since the prosthesis will first contact the undercuts and the other support areas, during insertion and the teeth will be engaged later, the prosthesis needs a compound path of insertion.
� Guide planes will assist in the precise placement of the prosthesis once the teeth have been contacted. They will also ensure more predictable retention and add a greater degree of stability to the prosthesis. Guide planes on the anterior abutment should be kept to a minimum vertical height (1 to 2 mm) to limit torque on the abutment teeth and should be physiologically adjusted. �This is important since movement can be expected during function because of the extensive lever arm provided by the defect and the dual nature of the support system.
�An indirect retainer is usually located perpendicular to the fulcrum line (which connects the most anterior and most posterior rests) and as far forward as possible. This is usually a canine or first premolar.
Retention �Retention is supplied by direct retainer designs that allow maximum protection of the abutment teeth during functional movements. �On the anterior abutment, a 19 - or 20 -gauge wrought wire clasp of the ‘‘I-bar’’ design is often used to engage a 0. 25 -mm undercut on the midlabial surface of this abutment.
CLASS I. LINEAR ARCH FORM Support �In the linear design, support is provided by the remaining posterior teeth and the palatal tissues. The palate becomes more important in the linear design because the use of leverage to resist vertical dislodging forces is decreased. Retention �Retention is usually provided by the combined use of buccal premolar retention and lingual molar retention.
Class II �This type of resection is favored prosthodontically and should therefore be advised to the surgeon
�Support- perpendicular to the fulcrum line rest is placed �Stability –from palatal surfaces of abutments �Retention – from buccal surfaces of the abutment teeth
Class III • The design is based on quadrilateral configurations. • Support is widely distributed on both premolars and molars. • Retention is derived from the buccal surfaces and stabilization from the palatal surfaces.
Class IV �The design is linear �Support –on the center of all remaining teeth. �Retention -palatal on the premolars; buccal on the molars. �Stability - mesially on the premolars. palatally on the molars.
Class V • Tripodal configuration • Splinting of at least two terminal abutment teeth on each side is suggested. • I –bar clasps are placed bilaterally on the palatal surfaces. • Stabilization and support are located on the buccal surface of the most distal teeth. •
Class VI � 2 anterior teeth are splinted bilaterally and connected by a transverse splint bar. �A clip attachment may be used without an elaborate partial framework. �If the defect is large, or the remaining teeth are in less than optimal condition, a quadrilateral configuration design is followed.
Procedures for restoration of maxillectomy defects in a dentulous oral cavity �Impressions �Impression for RPD framework �Altered cast Impression of the defect
Impression for RPD framework �A stock tray is used. Periphery wax is used to extend the tray into the defect and onto the soft palate. �The completed impression records the contours of residual tissues, the dentition, and the defect. �Undercuts on the medial side of the defect should be blocked out. Otherwise the residual palatal contours will be distorted upon removal of the tray.
�Master cast is surveyed. �The framework design is delineated on the master cast and the framework is cast.
�The framework is then tried in the mouth. �Silicone disclosing materials can be used to evaluate the intimacy of contact of the framework to the tissues and to identify the pressure areas; and necessary adjustment of the framework can be done. Chloroform/halothane and rogue can also be used for the same purpose, silicone being expensive. �The framework should exhibit satisfactory frictional fit to the teeth.
Altered cast impression �Fabrication of an occlusal stop on the oral side of the tray is recommended.
Border molding �Use of low fusing compound for border molding the defect. �Anterior region is border molded first to stabilize the denture base.
Movements �Mandible: �Wide opening �Lateral �Head �Right to left movement with neck in normal position �Right to left movment with neck flexed �Right to left movment with neck extended �Swallowing
�Incremental build up of the border moulding material can cause unseating of the metallic framework leading to errors in orientation of the defect to the residual maxilla, which can be avoided by fabrcation of an occlusal stop on the impression tray that records the defect and asking the patient to close on the stop everytime the framework is inserted.
Wash impression �The compound is cut back 1 -2 mm to create space for the wash material and thermoplastic wax is used to make a wash impression and record the defect in functional position.
�The impression is placed in the mouth and border molded.
Boxing and pouring of the altered cast
Centric relation records �The occlusal indices made during the altered cast impression can serve for mounting of the cast or centric relation records can also be obtained �By conventional method
�After mounting on a suitable articulator, teeth setting is done keeping esthetics and the occlusal guidelines presented earlier, in mind. �The trial prosthesis is then tried in mouth and necessary adjustments done. �The quality of obturation is checked during the try in stage by having the patient swallow water, and speech is evaluated by having the patient pronounce m and b. �Palatograms can be used to improve the palatal contour to aid in speech.
�Occlusion is achieved on the defect side, keeping in mind the points discussed earlier. �The prosthesis is processed in heat polymerized acrylic resin. �Finishing and polishing is done in the usual fashion.
Conclusion �“The love our face is next only to the love of our life and thus the mutilated cry for help” �As a prosthodontist our aim should be to render the best service possible to the patient in regard to the restoration and continuity of the defect to its most natural form �Basic knowledge of the technique, materials is the basic requirements for any rehabilitation procedure
� 1. 2. 3. 4. Which is not a surgical enhancement procedure for a maxillectomy patient Maintaining more contra lateral premaxillary area Maintaining the anterior alveolus and the floor of the nose Placement of a skin graft over denuded surfaces Resection of the inferior turbinate when the hard palate is resected but the tumor does not involve the nasal cavity
� Treatment following resection of hard palate does not involve 1. Allowing the sinus walls to become load bearing 2. The palatal bone screw can be placed through the acrylic resin baseplate in the midpalate and secured to the middle turbinate 3. Avoid placing a bone screw in the irradiated palate 4. Bone screws, sutures and packing can be removed without sedation
� Which of the following is false 1. Nasal reflux and hypernasal speech is caused by continues fibrosis in the tissues bordering the prosthesis 2. Improvement in swallowing and speech can be tested by m and s sounds 3. Relining of the prosthesis will not alter hypernasal speech when the soft palate is short in an antero-posterior direction 4. Pharyngeal obturator extension can be arbitarily shaped to extend into the pharyngeal opening over the soft palate
� Which is false when hypernasal speech occurs 1. Disclosure of the bulb with tissue conditioning material often reveals that the surface is inadequate 2. The prosthesis is adequately closed at the periphery 3. Patient’s soft palate closure mechanism is not functional 4. Patient’s pharyngeal closure mechanism is not functional
� Which of the following classification system does not involve dental criteria for maxillectomy 1. Aramany, 1978 2. Okay, 2001 3. Brown, 2000 4. Rodriguez, 2007