Respiratory Tract Infections Common cold Acute and chronic
 וסרלאוף")




")






")











- Slides: 59
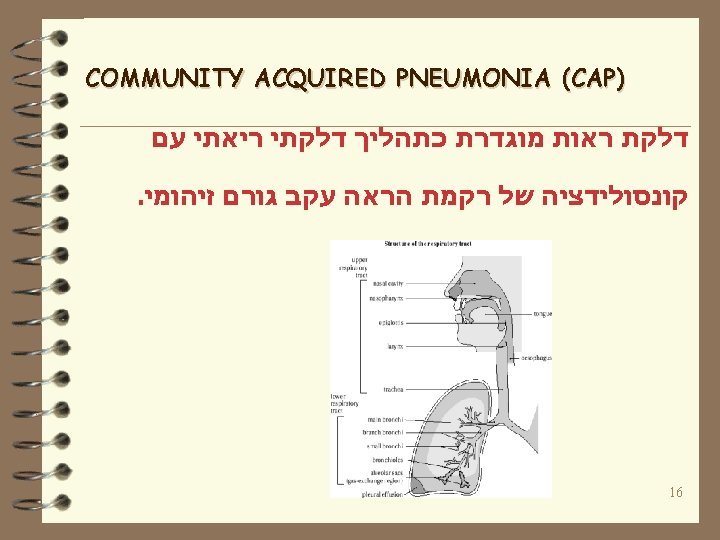
Respiratory Tract Infections Common cold Acute and chronic bronchitis Pneumonia (CAP and VAP) וסרלאוף - דר רות אורני היחידה למחלות זיהומיות ת”א , המרכז הרפואי ע”ש סוראסקי 1
The Common Cold The common cold is mild, self-limited, catarrhal syndrome SIGNIFICANCE- ·The leading cause of acute morbidity and of visits to a physician. ·Major cause of school and industrial absenteeism. 2
ETIOLOGY Five families of viruses: • Myxovirus, • Paramyxovirus, • Adenovirus, • Picornavirus • Coronavirus Adenovirus 3
VIRUSES ASSOCIATED WITH COMMON COLD Antigenic type Rhinoviruses 100 types +1 subtype Coronavirus 3 or more types Parainfluenza virus 4 types Respiratory syncytial virus 2 types Influenza virus 3 types Adenovirus 47 types Other viruses (Enterov. , Rubella, Rubeola, Varicella) Presumed undiscovered viruses Group A b-hemolytic streptococci %of cases 30 -40 > 10. 10 -15 5. 5 25 -30 5 -10. 4
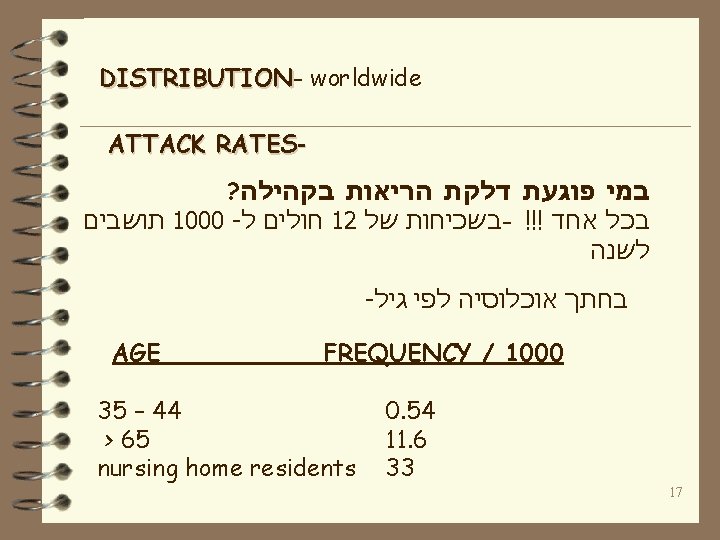
DISTRIBUTION worldwide SEASONAL INCIDENCE Colder month of the year, or rainy season in the tropics. ATTACK RATES During the season Adults have 6 -8 colds/ 1000 people/ day. (Children 9/1000) In the summer Adults have 2 -3 colds/ 1000 people/ day. 5
TRANSMISSIONClose contact (direct contact with infectious secretions or aerosol with large and small droplets) PATHGENESISviral infection of mucous membrane of nose, sinuses, throat and ear. 6
CLINICAL CHARACTERISTICS Incubation – 24 -72 hours Nasal discharge and obstruction, sneezing, soar or scrachy throat and cough. Low fever in adult, higher in children. Max. severity during the 2 nd or 3 rd day. Median duration – 1 week but in ¼ the disease last 2 weeks. 7
DIAGNOSIS · Clinical · Laboratory TREATMENT TLC, decongestants, cough control, worm saline gargles. PROSPECT OF NEW TREATMENT # Antiviral treatment # Virucidal hand wash # Preventive treatment 8
ACUTE BRONCHITIS ·Acute inflammation of the tracheo-bronchial tree, associated with generalized respiratory infection 9
ETIOLOGY Respiratory viruses – Mild disease with Rhinoviruses and some Coronaviruses, and more sever disease with Influenza virus and Adenovirus and lately with SARS (an new emerging Coronavirus. ) Respiratory bacteria – Bordetella pertussis, Mycoplasma pneumoniae, Chlamydia pneumoniae. 10
VIRUSES ASSOCIATED WITH ACUTE BRONCHITIS and cough %Of cases Influenza 75 -93 Adenovirus 45 -90 Renoviruses 32 -60 Coronaviruses 10 -50 RSV 61 Coxsackieviruses 26 Parainfluenza virus 2 -45 11
DISTRIBUTION- worldwide SEASONAL INCIDENCE all year, more cases in the winter, epidemic. ATTACK RATES in the UK: Mean 40 -50 / 100, 000 people Winter 117 -170 / 100, 000 Summer 26 -42 / 100, 000 12
TRANSMISSIONClose contact (direct contact with infectious secretions or aerosol with large and small droplets) PATH 0 GENESIS Hyperemia and edema of the tracheobronchial mucous membrane and increase in bronchial secretions. Local – extensive distraction of the airway epithelium. Slow down of bronchial tree mucociliary function. May play a role in pathogenesis of chronic obstructive lung disease. 13
CLINICAL CHARACTERISTICS- • Cough begins early and tends to become more prominent as the illness progresses. • The cough can continue for 2 -3 and even more weeks depend on the causing organism. (If the cough takes longer look for chronic disease) • Nasal discharge and obstruction, sneezing, soar or scratchy throat for 3 -5 days 14
DIAGNOSISclinical diagnosis is suspected with any acute RTI with cough. R/O pneumonia (history, exposure, physical examination and if needed chest x-ray). Specific cultures. TREATMENTSymptomatic- to control the cough (cough suppression an hydration) Antibacterial or antiviral therapy: according to the causing organism. PREVENTIONvaccination and medications 15
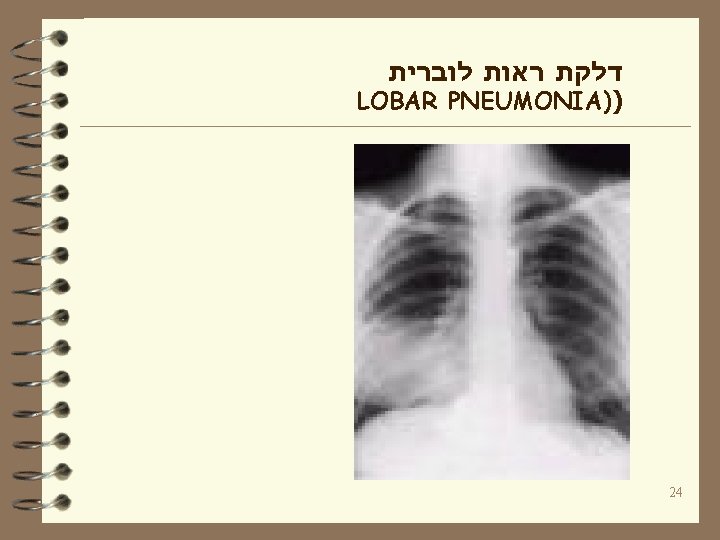
: גורם לדלקת ראות בסדרות שונות THE ORGANISM Unknown Strep. pneumoniae Haemophilus influenzae Legionella sp. Mycoplasma pneumoniae Infuenza virus Staph. aureus Strep. sp Chlamydia pneumoniae C. psittaci Aerobic gram negative bacilli % OF THE CASES 25 – 45 14 - 28 0 – 12 10 – 14 5 - 7 0 - 5 1 - 3 0– 3 0 - 4 3 - 12 19
PNEUNOMIA COUSING ORGANISMS BACTERIA S. pneumoniae H. influenza M. catharalis S. aureus Strep. sp. ATYPICAL BAC. K. pneumoniae M. pneumoniae E. coli L. pneumophila P. aeruginosa C. pneumoniae C. psitaci C. burnetii OTHERS ANAEROBES F. tularensis Nocardia sp. Staph. Epidermidis Myc. tuberculosis FUNGI P. jerovicii (PCP) Aspergillus sp 20
: דוגמה לטיפול בחולה דלקת ראות אמבולטורי Doxicyclin, Macrolides, New Quinolones דוגמה לטיפול בחולה דלקת ראות אמבולטורי : קשה 2 nd or 3 rd generation Cephalosporin iv + one of the above דוגמה לטיפול בחולה עם דלקת ראות קשה : בטיפול נמרץ 4 th generation cephalosporin iv+ Quinolone iv +/rifampin or carbapenem + new macrolide 36
includes Hospital acquired pneumonia Ventilator associated pneumonia 37
? מי החיידקים הגורמים לדר”נ • Streptococcus pneumoniae - 5 -20% • Haemophilus influenzae - 5 -15% • Staphylococcus aureus - 20 -40% • Pseudomonas aeruginosa • E. coli • Enterobacter spp. • Klebsiella pneumoniae • Serattia marcescens • Acinetobacter 25 -60% 49
• Legionella pneumopila 5% ? מי עוד 0 - • Mycobacterium tuberculosis - <1% • Anaerobes - <35% • Polymicrobial - 25 -46% • VIRAL- RSV, Influenza, parainfluenza 50