Respiratory system Lecture 1 Atelectasis and Disturbances of

Respiratory system Lecture 1 Atelectasis and Disturbances of Pulmonary Circulation.
: l It is loss of lung volume. l Caused by:")
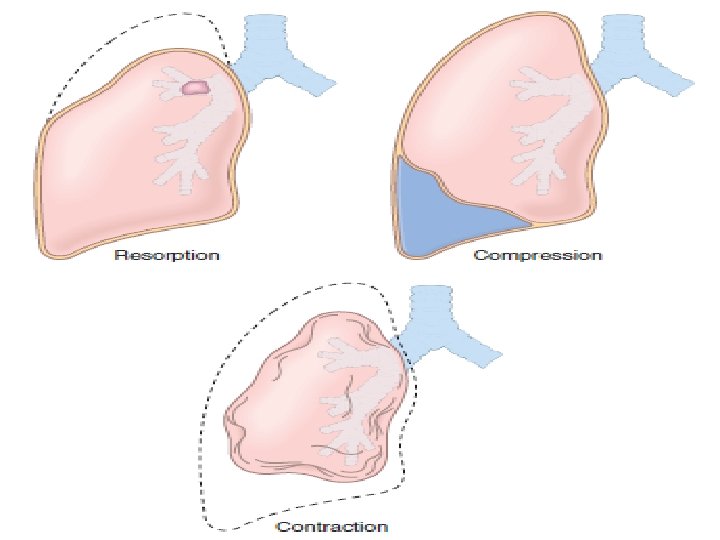
Lung diseses: Atelectasis (Collapse): l It is loss of lung volume. l Caused by: l Inadequate expansion of air spaces. l Results in hypoxia ( O 2). l Three forms: Resorption, Compression & Contraction atelectasis.
 Cause: Obstruction that prevents air from reaching distal airways.")
1 • Resorption atelectasis: (Obstructive) Cause: Obstruction that prevents air from reaching distal airways. Obstruction of bronchus by: # Mucous or muco-purulent plug: Postoperatively after surgery. Bronchial asthma. Bronchiectasis. Chronic bronchitis. # Tumor. # Foreign body aspiration (In children).
. Causes: 1. Accumulation of fluid, blood,")
2 • Compression atelectasis: (Passive or relaxation atelectasis). Causes: 1. Accumulation of fluid, blood, or air within the pleural cavity, occurs with: # Pleural effusion caused by congestive heart failure (CHF). # Pneumothorax: Leakage of air into pleural cavity. 2. Elevated position of diaphragm occurs in: - Bedridden patients. - Patients with ascites.
 Cause: Fibrotic changes in the lung or pleura preventing")
3 • Contraction atelectasis: (Cicatrization) Cause: Fibrotic changes in the lung or pleura preventing expansion. Atelectasis: q Reversible except the contraction type. q Should be treated to prevent hypoxemia and superimposed infection of the collapsed lung.

Pulmonary diseases of vascular origin Pulmonary Embolism, Hemorrhage & Infarction v Pulmonary thrombus: v It is blood clots that may occlude large or small pulmonary arteries. v Almost always embolic in origin. v More than 95% arise from thrombus within the large deep veins of lower legs, so called: Thromboembolism.
 Prolonged bedrest with immobilization of")
Risk factors of venous thrombosis in the legs: (1) Prolonged bedrest with immobilization of legs. Surgery: Orthopedic surgery of knee & hip. Severe trauma: Burns or multiple fractures. (2) Congestive heart failure. (3) Oral contraceptive pills use with high estrogen content. (Increase conc. of coagulative protein). (4) Disseminated cancer. (5) Primary disorders of hypercoagulability: e. g. : Factor V Leiden: Mutation in clotting factors.

Nonthrombotic forms of pulmonary embolism: 1. Air embolism. 2. Fat embolism. 3. Amniotic fluid embolism. 4. Foreign body embolism: In intravenous drug abuse. 5. Bone marrow embolism: Hematopoietic & fat elements within pulmonary circulation occur after massive trauma.

Pathological consequences of thromboembolism: Depend on: 1. Size of embolus: Large Occlusion. Small Clinically silent. 2. Cardiopulmonary status of patient. Consequences of embolic pulmonary arterial occlusion: (1) Increase in pulmonary artery pressure due to blockage of flow & vasospasm caused by neurogenic mechanisms and/or release of mediators. (2) Ischemia of pulmonary parenchyma.

Occlusion of major vessel results in: q q q Sudden increase in pulmonary artery pressure. Diminished cardiac output. Right-sided heart failure (Acute cor pulmonale). Hypoxemia Death. q Occlusion of smaller vessels is less effective & is clinically silent.

Morphology of pulmonary embolism: Large embolus: In the main pulmonary artery or its major branches or lodge across the bifurcation as a: Saddle embolus Hypoxia. Acute right side heart failure. Death. No time for morphologic alterations in the lung. Large saddle embolus across the left & right pulmonary arteries.

Smaller emboli: Impacted in medium & small pulmonary arteries. The vitality of lung parenchyma is maintained, because there adequate circulation from bronchial arterial flow. Alveolar hemorrhage occur as a result of ischemic damage to the endothelial cells.

Clinical features of pulmonary thromboembolism q • 60 -80% of pulmonary emboli are small. q. Clinically silent. q. Rapidly removed by fibrinolytic activity. q. Bronchial circulation sustains the viability of affected lung parenchyma. v • In 5%: v. Sudden death. v. Acute right-sided heart failure.

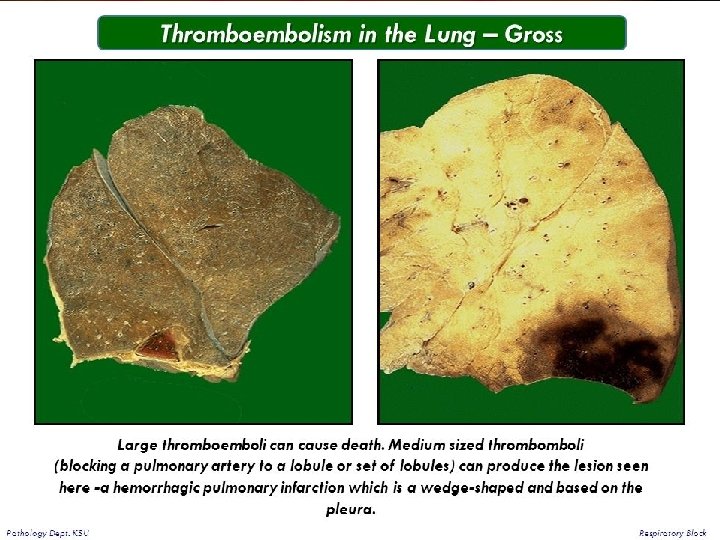
Infarction = Ischemic necrosis Occurs in only 10% of thromboembolism, because lungs are oxygenated by pulmonary arteries, bronchial arteries & directly from air in the alveoli. Causes: 1. Compromised cardiovascular function. 2. Underlying pulmonary disease resulting in underventilated region in the lung.

Morphology of infarction: Wedge-shaped, with their base at pleural surface and apex pointing toward hilus of lung. In early stage: Hemorrhagic raised, red-blue areas. Within 48 hours: Lysis of red cells Pale infarct (Hemosiderin production). By time: Fibrous tissue replacement: A gray-white peripheral zone (Scar). Red-brown

Wedge-shaped hemorrhagic pulmonary infarct.

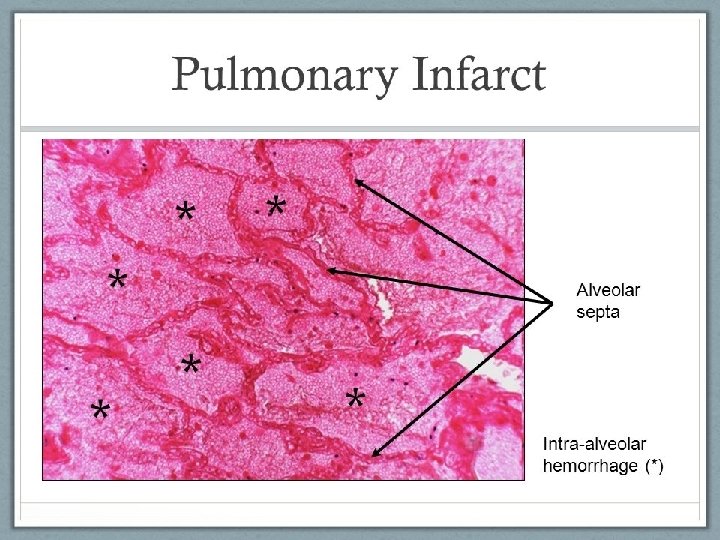
Histologic examination: Coagulative necrosis of lung parenchyma & hemorrhage.

Pulmonary Hypertension Pulmonary circulation is of low resistance & pulmonary blood pressures are one eighth of systemic pressures. Pulmonary hypertension: Occurs when the mean pulmonary pressures reach one fourth or more of systemic levels. Pulmonary hypertension: 1. Primary. 2. Secondary.

Primary or idiopathic pulmonary hypertension: ØOccurs without obvious causes. ØMostly sporadic. Ø 6% : Familial (Autosomal dominant inheritance). Secondary pulmonary hypertension: Causes: 1. Decrease in cross-sectional area of pulmonary vessels (narrowing of lumen). 2. Increased pulmonary vascular blood flow.

These may occurs in: 1. • Chronic lung disease Destruction of lung & reduction in alveolar capillaries Increased pulmonary arterial resistance Elevated arterial pressure. 2. • Recurrent pulmonary emboli Reduction in cross-sectional area of vascular bed Increased vascular resistance. 3. • Heart disease: Mitral stenosis increases left atrial pressure Higher pulmonary venous pressures Pulmonary arterial hypertension.

Pathogenesis In most forms of pulmonary hypertension, there will be pulmonary endothelial cell and/or vascular smooth muscle dysfunction. There is production of growth factors & cytokines that induce the migration and replication of vascular smooth muscle and elaboration of extracellular matrix. Abnormal vascular endothelial and pulmonary smooth muscle proliferation.
 Main elastic arteries: Atheromas similar to those in atherosclerosis. Gross picture of")
Morphology (1) Main elastic arteries: Atheromas similar to those in atherosclerosis. Gross picture of atheroma, a finding limited to large vessels.
 In medium-sized muscular arteries: Proliferation of myointimal cells and smooth muscle cells, causing")
(2) In medium-sized muscular arteries: Proliferation of myointimal cells and smooth muscle cells, causing thickening of intima & media with narrowing of lumin. Marked medial hypertrophy.
 In smaller arteries & arterioles: Thickening, medial hypertrophy & reduplication of internal &")
(3) In smaller arteries & arterioles: Thickening, medial hypertrophy & reduplication of internal & external elastic membranes leading to narrowing of lumen.

Idiopathic pulmonary arterial hypertension: Plexiform lesions: Endothelial proliferation forms multiple lumina within small arteries. Plexiform lesion characteristic of advanced pulmonary hypertension seen in small arteries.

Clinical Features It reflect the underlying disease, pulmonary or cardiac. 1. Fatigue. 2. Syncope (Fainting) particularly on exercise. 3. Dyspnea on exertion (Shortness of breath). 4. Sometimes chest pain. 5. Severe respiratory insufficiency & cyanosis. 6. Death results from right-sided heart failure.

THANK YOU
- Slides: 30