RESPIRATORY MEDICINE Pulmonary Tuberculosis Objectives To know the

RESPIRATORY MEDICINE Pulmonary Tuberculosis •

Objectives To know the following Epidemiology Etiology Pathogenesis Clinical presentation Diagnosis Treatment Complication and prognosis

Case 1 • Twenty five years old female presented with 2 months fever , night sweating, weight loss. • Dry cough • Tem 38 c R. Rate 20 • Chest clear. • What is d dx will include.

Case 2 Seventeen years student present with heamoptysis , fever , weight loss What investigation? What D dx ?

Case 3 • Sixty five years old male present with weight loss fatigue, enlargment of liver and spleen. • What is next ?
 is one of the oldest diseases known to affected humans.")
Introduction q. Tuberculosis (TB) is one of the oldest diseases known to affected humans. q Caused by bactria of mycobacterium complex, and usually affects the lungs. q. Transmitted by airborne droplet nuclei from infected persons. qcurable if properly treated. q May be fatal within 5 years in 50 -60%of cases if not treated

Old Disease

Oldest cases of T B
 is caused by infection with Mycobacterium tuberculosis (MTB). • In")
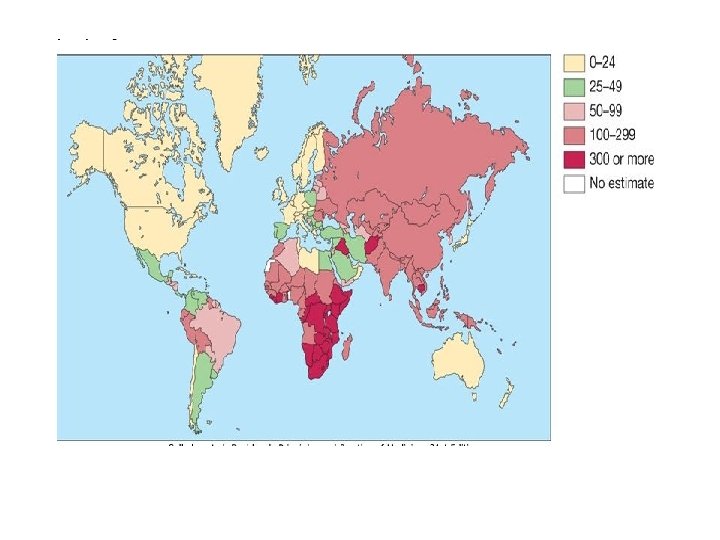
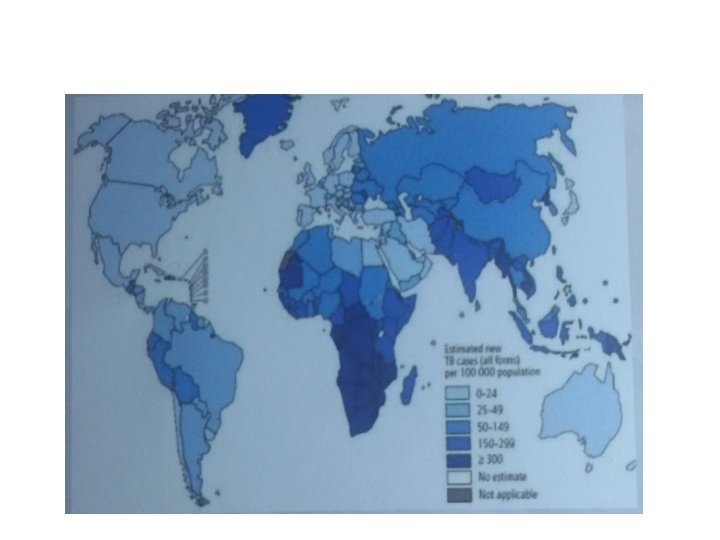
Epidemiology • Tuberculosis (TB) is caused by infection with Mycobacterium tuberculosis (MTB). • In 2006 • there were an estimated 9. 2 million new cases, 14. 4 million prevalent cases and 1. 5 million deaths attributable to TB. • around one-third of the world's population has latent TB. • The majority of cases occur in the world's poorest nations. • The resurgence of TB has been largely driven by HIV disease and by lack of appropriate health care.

Iraq has a • high burden of TB, the estimated incidence was 45 per 100, 000. • Prevalence is 74 per 1 00 000. • Mortality is 3 per 1 00 000.

Flourescent stained microcolonies of M. tuberclonies.

Pathology and pathgenesis • M. bovis infection arises from drinking nonsterilized milk from infected cows. • M. tuberculosis is spread by the inhalation of aerosolised droplet nuclei from other infected patients.

• Once inhaled, the organisms lodge in the alveoli and initiate the recruitment of macrophages and lymphocytes. • Macrophages undergo transformation into epithelioid and Langhans cells which aggregate with the lymphocytes to form the classical tuberculous granuloma.

Granuloma formation in the lung. The central region of multinucleated giant cells, mycobacteria and necrotic debris (right) is surrounded by concentric rings of tightly apposed epithelioid cells and lymphocytes, with smaller numbers of neutrophils, plasma cells and fibroblasts.

q Primary lesion or 'Ghon focus Form from aggregation of numerous granulomas which is situated in the periphery of the lung. q‘Primary complex of Ranke The combination of a primary lesion and regional lymph nodes ( the hilar lymph nodes) which has similar pathological reaction.

q Latent TB the primary complex in a fibrous capsule limiting the spread of bacilli WHICH calcifies and is seen on a chest X-ray. q Spread lymphatic or haematogenous before immunity, seeding secondary foci in other organs including lymph nodes, serous membranes, meninges, bones, liver, kidneys and lungs, which may lie dormant for years.

What Tuberculin skin test ? • The appearance of a cell-mediated, delayedtype hypersensitivity reaction to tuberculin. What happened if we inhale bacilli ? • The estimated lifetime risk of developing disease after primary infection is 5 - 10%, • half of this risk occurring in the first 2 years after infection.

Electron microscopy show T. B bacilli

Granuloma

Positive Ziehl–Neelsen stain. Mycobacteria retain the red carbol fuschin stain despite washing with acid and alcohol.

Diagram of the development of tuberculosis disease and its spread through the body .

Timetable of TB Time from infection Manifestations • 3 -8 weeks Primary complex, positive tuberculin skin test • 3 -6 months Meningeal, miliary and pleural disease • Up to 3 years Gastrointestinal, bone and joint, and lymph node disease • Around 8 years Renal tract disease • From 3 years onwards Post-primary disease due to reactivation or reinfection

Pathogenesis of TB infection

The answer
 Spread from the primary focus to hilar and mediastinal lymph")
Primary pulmonary TB. (1) Spread from the primary focus to hilar and mediastinal lymph glands to form the ‘primary complex’, which in most cases heals spontaneously. (2) Direct extension of the primary focus— progressive pulmonary TB. (3) Spread to the pleura—tuberculous pleurisy and pleural effusion. (4) Blood-borne spread: few bacilli—pulmonary, skeletal, renal, genitourinary infection often months or years later; massive spread—miliary TB and meningitis.
 Spread from the primary focus to hilar and")
Primary pulmonary TB. • (1) Spread from the primary focus to hilar and mediastinal lymph glands to form the 'primary complex', which in most cases heals spontaneously. • (2) Direct extension of the primary focusprogressive pulmonary TB. • (3) Spread to the pleura-tuberculous pleurisy and pleural effusion. • (4) Blood-borne spread: few bacilli-pulmonary, skeletal, renal, genitourinary infection often months or years later; massive spread-miliary TB and meningitis

q Factors increasing the risk of TB I--Patient-related • Age (children > young adults < elderly) • First-generation immigrants from high-prevalence countries • Close contacts of patients with smear-positive pulmonary TB • Overcrowding (prisons, ); homelessness. • Chest radiographic evidence of self-healed TB • Primary infection < 1 year previously • Smoking: cigarettes and bidis (indian cigarettes).

II—Associated diseases • Immunosuppression: HIV, anti-TNF therapy, highdose corticosteroids, cytotoxic agents. • Malignancy (especially lymphoma and leukaemia) • Type 1 diabetes mellitus • Chronic renal failure • Silicosis • Gastrointestinal disease associated with malnutrition • Deficiency of vitamin D or A • Recent measles.

Pathogenesis and progress of T B

Clinical features: • • • pulmonary disease Primary pulmonary TB. Post primary pulmonary T B. Miliary TB. Cryptic TB.
 • • • Influenza-like")
Features of primary TB q Infection (4 -8 weeks) • • • Influenza-like illness Skin test conversion Primary complex
. paratracheal")
Features of primary TB q Disease • • • Lymphadenopathy: hilar (often unilateral). paratracheal or mediastinal. Collapse (especially right middle lobe). Consolidation (especially right middle lobe). Obstructive emphysema. Pleural effusion. Endobronchial. Miliary. Meningitis. Pericarditis. q Hypersensitivity • Erythema nodosum. • Phlyctenular conjunctivitis. • Dactylitis.

Erythema nodusum

Phlyctenullar conjuctivitis

Miliary TB • • • Blood-borne dissemination acute 2 -3 weeks of fever, night sweats, anorexia, weight loss dry cough. Hepatosplenomegaly headache may indicate tuberculous meningitis.
 Chest x-ray and (b) CT scan from a 27 -year-old student with disseminated")
(a) Chest x-ray and (b) CT scan from a 27 -year-old student with disseminated tuberculosis. Multiple small opacities (miliary shadowing) are seen in the periphery of the chest x-ray and much more clearly in all areas of the CT scan
 Chest x-ray and (b) CT scan from a 27 -year-old student with disseminated")
(a) Chest x-ray and (b) CT scan from a 27 -year-old student with disseminated tuberculosis. Multiple small opacities (miliary shadowing) are seen in the periphery of the chest x-ray and much more clearly in all areas of the CT scan

• Auscultation of the chest is frequently normal, advanced disease crackles. • Fundoscopy show choroidal tubercles. • The classical appearances on chest X-ray are of fine 1 -2 mm lesions ('millet seed'). • Anaemia and leucopenia reflect bone marrow involvement.

'Cryptic' miliary TB • Age over 60 years • Intermittent low-grade pyrexia of unknown origin • Unexplained weight loss, general debility (hepatosplenomegaly in 25 -50%) • Normal chest X-ray • Blood dyscrasias; leukaemoid reaction, pancytopenia • Negative tuberculin skin test • Confirmation by biopsy (granulomas and/or acid-fast bacilli demonstrated) of liver or bone marrow

Post-primary disease q • • • q v v • • • Exogenous ('new' infection) Endogenous (reactivation of a dormant primary lesion) Lung apices. The onset insidious, slowly over several weeks. Systemic symptoms progressive pulmonary symptoms. Radiological changes include opacification in one or both of the upper lobes, consolidation collapse cavitation tuberculous pneumonia

Chronic complications of pulmonary TB Pulmonary • Massive haemoptysis • Cor pulmonale • Fibrosis/emphysema • Atypical mycobacterial infection • Aspergilloma • Lung/pleural calcification • Obstructive airways disease • Bronchiectasis. • Bronchopleural fistula

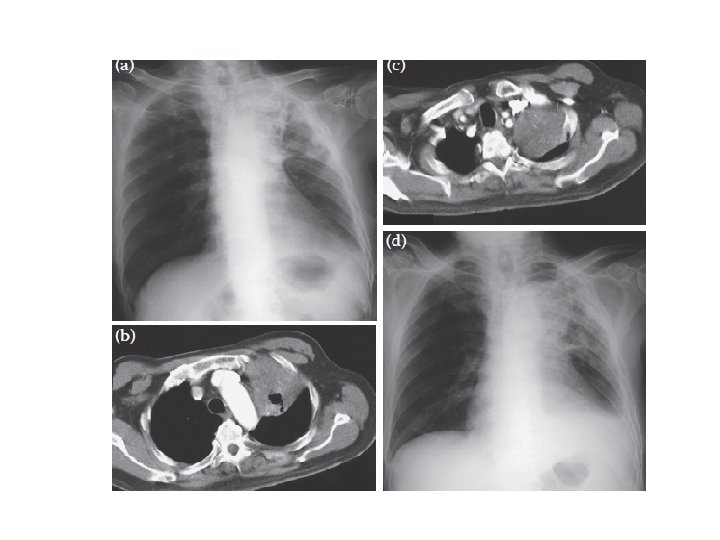
Case • Radiological investigation of a 78 -year-old man with a six-week history of productive cough, fever, left-sided chest pain, dyspnoea on exertion and hoarse voice. (a) Chest x-ray and (b) CT scan showed (c) a soft tissue mass in the left upper lobe that encased the left upper lobe bronchus. (d) A chest x-ray performed at the end of TB treatment showed a significant resolution of the initial consolidation seen in the left upper lobe, persistence of the mass (diagnosed as being carcinoid tumour), left upper lobe fibrosis, loss of left lung volume, a left pleural effusion and a large heart shadow

Posteroanterior chest x-ray showing an aspergilloma in the left apex.

Non-pulmonary complication • • • Empyema necessitans Laryngitis Enteritis. Anorectal disease. Amyloidosis. Poncet's polyarthritis

Diagnosis of TB • Specimens required q Pulmonary • Sputum (induced with nebulised hypertonic saline if not expectorating) • Bronchoscopy with washings or BAL • Gastric washing (mainly used for children) q Extrapulmonary • Fluid examination (cerebrospinal, ascitic, pleural, pericardial, joint): yield classically very low • Tissue biopsy (from affected site); also bone marrow/liver may be diagnostic in patients with disseminated disease
 • Tuberculin skin")
• Diagnostic tests • Circumstantial (ESR, CRP, anaemia etc. ) • Tuberculin skin test (low sensitivity/specificity; useful only in primary or deep-seated infection) • Stain – Ziehl-Neelsen – Auramine fluorescence • Nucleic acid amplification • Culture – Solid media (Löwenstein-Jensen, Middlebrook) – Liquid media (e. g. BACTEC or MGIT) • Response to empirical antituberculous drugs (usually seen after 5 -10 days)

Sputum AFB positive

T B bacilli

• • • • • Skin testing in TB: tests using purified protein derivative (PPD) Heaf test Mantoux test Results may be: False negatives false-positive

Gradings of the Heaf test response. A Negative. B Grade 1. C Grade 2. D Grade 3. E Grade 4.

Chest Xray TB

Chest Xray

Chest Xray

Chest Xray

CT Chest pulmonary TB show cavitation
. • culture filtrate protein")
Other TEST FOR PULMONARY TB • Interferon-gamma release assays (IGRAs). • culture filtrate protein (CFP)-10. .

The principles of interferon-gamma release assays.

• Chemotherapy q Indication: • Patient who is smear-positive, • smear-negative but with typical chest X-ray changes. q Quadruple therapy has become standard • Fixed-dose tablets combining two or three drugs are generally favoured: • (rifampicin, isoniazid and pyrazinamide) daily for 2 months(initial phase) • (rifampicin and isoniazid) daily for 4 months(continous phase).

q Duration of treatment • Six months of therapy • all patients with new-onset, uncomplicated pulmonary disease. • 9 -12 months of therapy • HIV-positive • drug intolerance • 12 months • Meningitis q Added to treatment Pyridoxine • pregnant women • malnourished patients. • Where drug resistance is not anticipated, patients can be assumed to be non-infectious after 2 weeks of appropriate therapy.

q Admission to a hospital unit if : • Uncertainty about the diagnosis. • Intolerance of medication. • Questionable compliance. • adverse social conditions. • a significant risk of multidrug-resistant TB (MDR-TB: culture-positive after 2 months on treatment, or contact with known MDR-TB).

• • • Recommendations in treatment Do baseline liver function and regular monitoring. Adverse drug reactions occur in about 10% of patients. Corticosteroids reduce inflammation Surgery is still occasionally required but usually only after a full course of antituberculosis treatment. • A positive sputum smear at 5 months defines treatment failure

• Control and prevention • 1 -detection of latent TB • 2 - treatment of active and latent TB. q Detection of latent TB • Contact tracing. • Probable index case. • Close contacts who should receive BCG vaccination or chemotherapy. • Rifampicin plus isoniazid for 3 months or isoniazid for 6 months is effective. q Vaccines • BCG (the Calmette-Guérin bacillus), a live attenuated vaccine, . BCG appears to be effective in preventing disseminated disease
 Poor adherence to therapy is")
• • • • Directly observed therapy (DOT) Poor adherence to therapy is a major factor in: prolonged infectious illness risk of relapse the emergence of drug resistance. Recommended unlikely to be adherent to therapy homeless, alcohol drug users serious mental illness non-compliance

• TB and HIV/AIDS • It is recommended that all patients with TB should be counselled and tested for HIV disease. • Mortality is high and TB is a leading cause of death in HIV patients.

• Drug-resistant TB • defined by the presence of resistance to any first-line agent. • Multidrug-resistant (MDR) TB. • Extensively drug-resistant (XDR). • Diagnosis is challenging

• Prognosis • Following successful completion of chemotherapy, cure should be anticipated in the majority of patients. • A small risk of relapse.

Thank u

Q QIUZE
- Slides: 74