Respiratory Distress Syndrome obstructive vs restrictive lung disease

Respiratory Distress Syndrome obstructive vs. restrictive lung disease Fatma Rabea Ahmed Hamdan Physiology department Qena Faculty of Medicine South Valley University

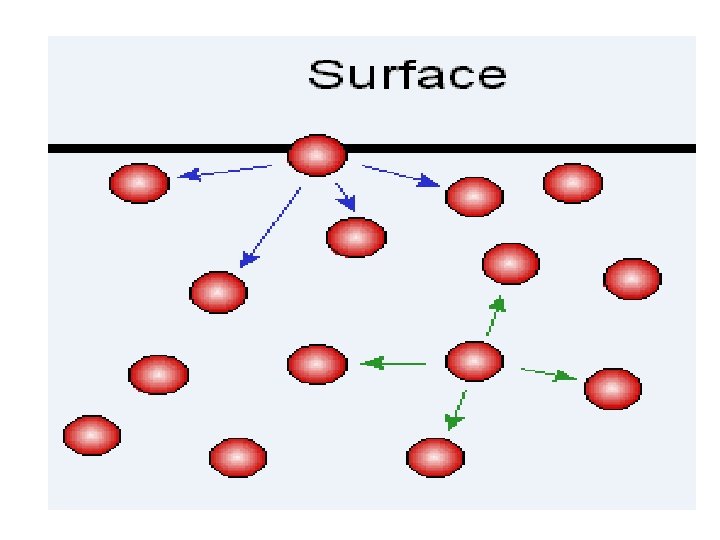
ELASTIC RECOIL OF THE LUNGS: ●Def. , When the lung is inflated, it tends to recoil (collapse). ●Causes: 1 -Elastic fiber in the lung (responsible only for 30%). 2 -Surface tension of fluid lining alveoli (responsible for 70%).

THE PULMONARY SURFACTANT ●Def. , It is the It is a surface active agents secreted by type II alveolar epithelial cell to decrease the surface tension of fluid lining alveoli and antagonist lung collapse. ●Composition: It is mixture of: 1 -Phospholipids 77% = (diplmintoyl phosphatidyl cholin and glycerine). Lecithin comprises about 70% of the total surfactant phospholipids. 2 -lipoprotein 8% 3 -calcium ions (increase rate of spread).
")
●Mechanism of Action -Physpholipid is formed of two parts; hydrophilic head (towards the fluid) and hydrophobic tail (towards air). It interdigitates between the water molecules and prevents the attractive force between them. ﺷﻜﻠﻪ ﺫﻯ ﺍﻟﺴﻨﻪ ﻟﻬﺎ ﺭﺍﺱ ﻭﺟﺬﺭ -Calcium and lipoproteins allow for rapid and better spread of surfactant over the fluid surface.

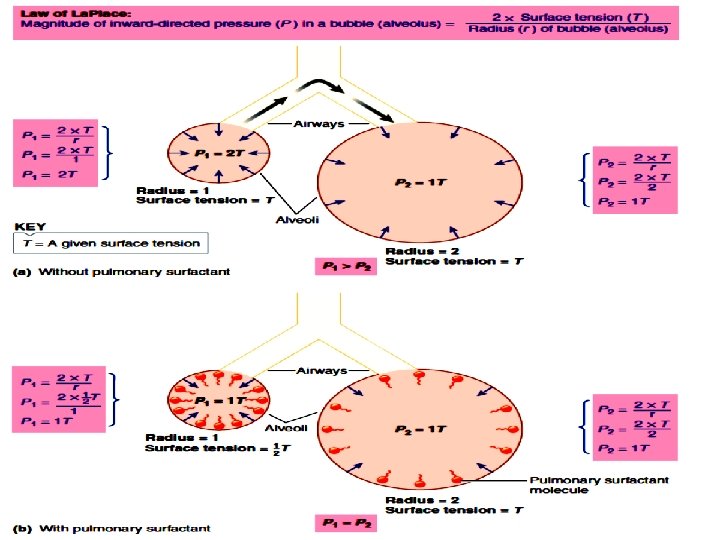
●Functions: 1 - Decreases the tendency of alveoli to collapse. 2 - Decreases the muscular work of breathing and increases the pulmonary compliance (reducing the effort needed to expand the lungs). 3 - Prevents the pulmonary edema (safety factor). Surface tension not only pulls alveolar wall to the center of alveolus but also pulls fluid from capillaries into alveoli leading to pulmonary edema. Surfactant prevents this phenomenon by decreasing surface tension. 4 - Alveolar stabilization: According to the low of Laplace: the pressure in alveoli (P) as spherical structure equals twice the surface tension (T) divided by the radius (r). P = 2 T/r

●Factors Affecting the Surfactant Formation: A-Factors which increase: -Glucocorticoids help the surfactant maturation. -Thyroid hormone increases the size and number of bodies in alveolar II cells. B- Factors which decrease: - Smoking. - Insulin hormone. (Hypoglysemia stops alveolar II) -Long term inhalation of pure O 2. (DAMAGE) - Occlusion of main bronchus. ( ↓ o 2 supply to alveolar II ) - Occlusion of pulmonary artery ↓ o 2 & nutrition supply to alveolar II - Cutting of both vagi.
. 2 -Pulmonary Edema.")
Surfactant Deficiency 1 -Respiratory Distress Syndrome (= Hyaline Disease). 2 -Pulmonary Edema.

1 -Respiratory Distress Syndrome is common in A- premature babies Surfactant production starts around 20 wks of life and peaks at 35 wks. Therefore any neonate less than 35 wks is prone to develop RDS, without surfactant infants are unable to keep their lungs inflated.

1 -Respiratory Distress Syndrome is common in B-Babies with diabetic mothers (those babies were subjected to fetal hyperinsulinemia, which suppress the surfactant formation). C- Interruption of the pulmonary circulation with lung ischemia as during open-heart surgery (= damage of type II cells) (patchy atelectasis).

Respiratory Distress Syndrome -Effect: The surface tension is abnormally high; the work of breathing is markedly increased. Large regions of alveoli are collapsed (atelectasis) & death may occur. • During expiration>> Absence of surfactant >> Surface tension increases >> Alveoli collapse • During inspiration>> More negative pressure is needed to keep alveoli patent.

Respiratory Distress Syndrome • Due to all these conditions >> Inadequate Oxygenation >> Increased work of breathing >>> Hypoxemia and acidosis >> Pulmonary vasoconstriction >> Right to left shunting across foramen ovale >>> Worsens Hypoxia >>> Respiratory failure

Respiratory Distress Syndrome -Diagnosis: By taking amniotic fluid sample and estimated of lecithin/ sphingomyelin ratio (test for lung maturity) (normally it is more than 2, but in respiratory distress syndrome it is less than 1. 5). -Treatment: by inhalation of bovine surfactant.
![Clinical feature • Tachypnea (< or = 80 – 120 breaths per min) [Wong’s]](http://slidetodoc.com/presentation_image_h2/8593bd96dac27325d30508202c43981b/image-15.jpg "Clinical feature • Tachypnea (< or = 80 – 120 breaths per min) [Wong’s]")
Clinical feature • Tachypnea (< or = 80 – 120 breaths per min) [Wong’s] • Dyspnea • Pronounced intercostals or substernal retractions • Fine inspiratory crackles • Audible expiratory grunt • Flaring of external nares • Cyanosis or pallor


Case Study • A 24 -year-old pregnant woman presented to the hospital in preterm labor and subsequently delivered a premature infant at only 27 weeks gestation (normal term pregnancy is 37 -42 weeks). After the delivery, the infant cried, but it subsequently began to grunt and showed signs of hypoxia despite oxygen supplementation. The baby immediately was intubated by endotracheal tube and given surfactant down the endotracheal tube. The baby’s hypoxia resolved, and he was transferred to the neonatal intensive care unit for further stabilization.

Case Study • • • 1 - What is the principal cause of RDS? 2 - What is the role of surfactant in the lung? 3 - What is the effect of RDS on the infant? 4 -Who have low incidence of RDS? Why? 5 -Where is the major site of airway resistance?

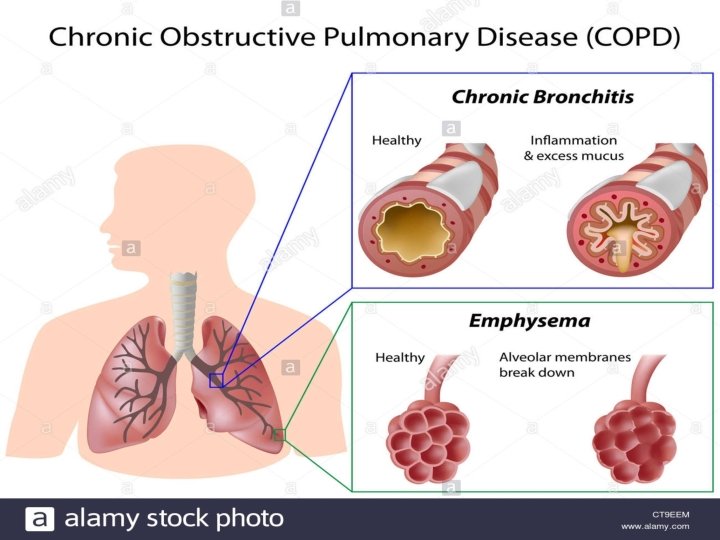
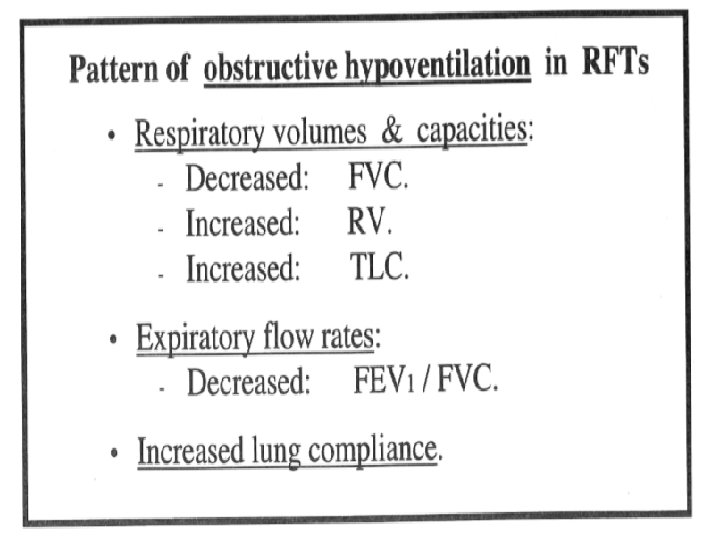
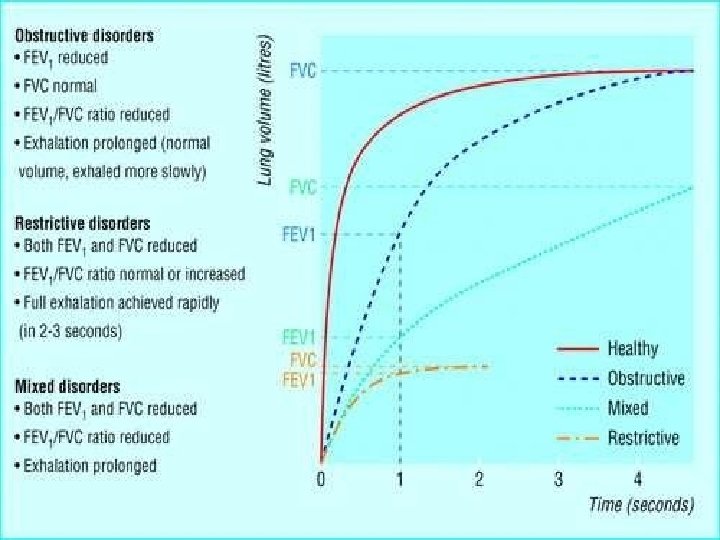
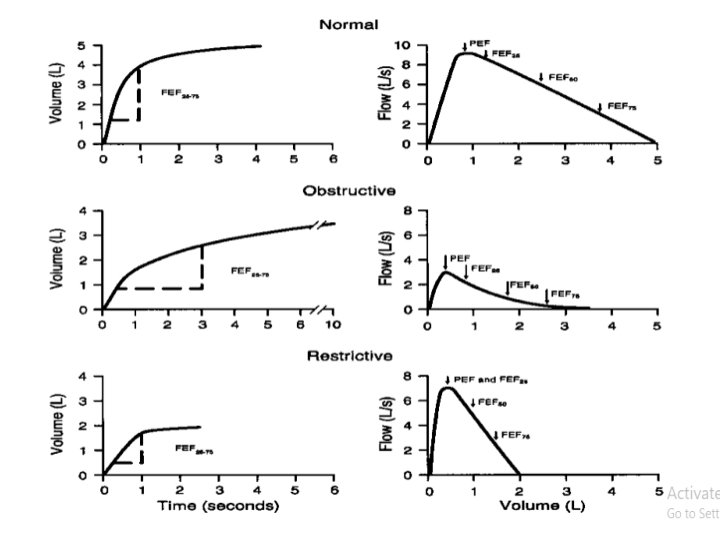
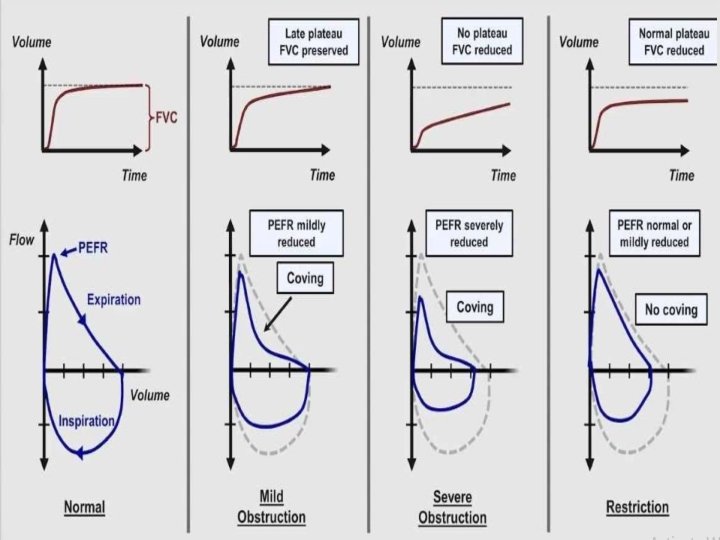
Obstructive Lung Disease • shortness of breath due to difficulty exhaling all the air from the lungs. • Because of damage to the lungs or narrowing of the airways inside the lungs, exhaled air comes out more slowly than normal. • At the end of a full exhalation, an abnormally high amount of air may still linger in the lungs.
, which includes emphysema and chronic")
most common causes • Chronic obstructive pulmonary disease (COPD), which includes emphysema and chronic bronchitis • Asthma • Bronchiectasis • Cystic fibrosis

Obstructive Lung Disease • Obstructive lung disease makes it harder to breathe, especially during increased activity or exertion. • As the rate of breathing increases, there is less time to breathe all the air out before the next inhalation.


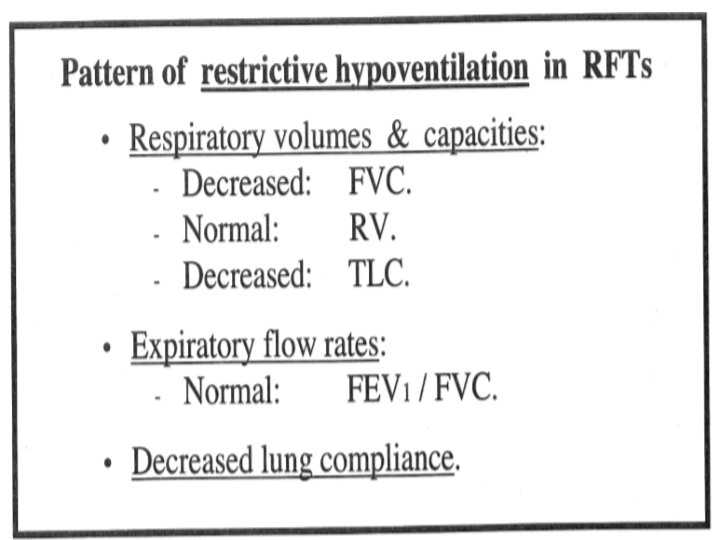
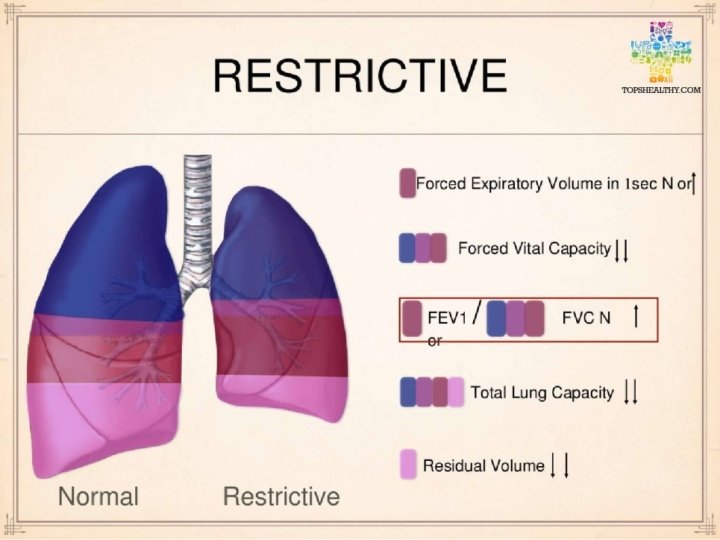
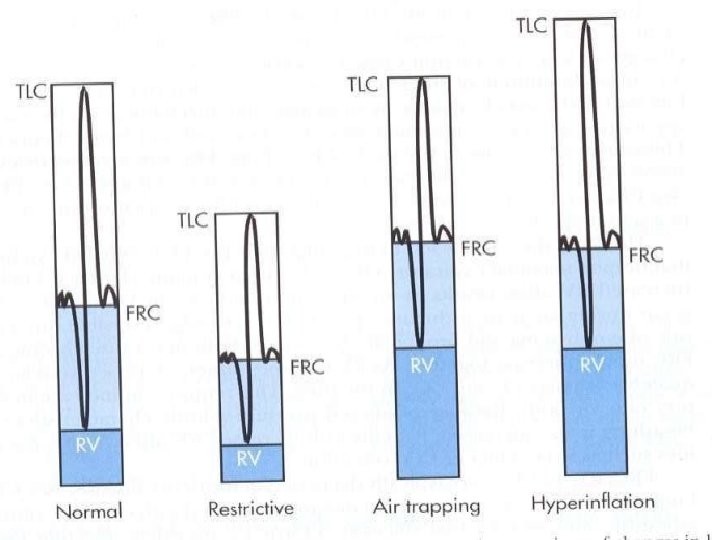
Restrictive Lung Disease • The lungs are restricted from fully expanding. • Restrictive lung disease most often results from a condition causing stiffness in the lungs themselves. In other cases, stiffness of the chest wall, weak muscles, or damaged nerves may cause the restriction in lung expansion.

Restrictive Lung Disease Some conditions causing restrictive lung disease are: • Interstitial lung disease, such as idiopathic pulmonary fibrosis • Sarcoidosis, an autoimmune disease • Obesity, including obesity hypoventilation syndrome • Scoliosis • Neuromuscular disease, such as muscular dystrophy or amyotrophic lateral sclerosis (ALS)
- Slides: 32