RESIDUAL RIDGE RESORPTION INTRODUCTION Residual Ridge resorption RRR

 is a complex biophysical process. According to Mosby the")





























- Slides: 32
RESIDUAL RIDGE RESORPTION
INTRODUCTION Residual Ridge resorption (RRR) is a complex biophysical process. According to Mosby the following terms are defined: Residual: Pertaining to the position of something that remains after an activity that removes the bulk of the substance. Ridge: A projection or projecting structure. Resorption: A loss of substance or bone by physiologic or pathologic means, such as the reduction of the volume and size of the residual ridge of the mandible or maxilla.
Residual Ridge: The portion of the dental ridge that remains after the alveolar process has disappeared after extraction of the teeth. Residual ridge resorption (GPT 7): A term used for the diminishing quantity and quality of the residual ridge after teeth are removed.
CLASSIFICATIONS OF RESIDUAL RIDGE RESORPTION According to Brånemark et al in 1985, ridges were classified on the basis of bone quantity and bone quality by radiographic means. BONE QUANTITY: (Brånemark) Class A: Most of the alveolar bone is present Class B: Moderate Residual Ridge Resorption occurs Class C: Advance residual ridge resorption occurs Class D: Moderate resorption of the basal bone is present Class E: Extreme resorption of the basal bone
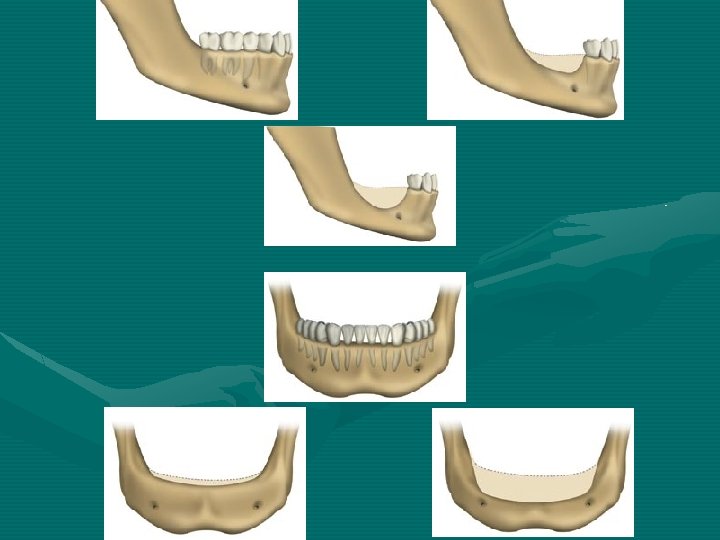
ATWOOD’S CLASSIFICATION: Order I Pre-extraction Order II Post – extraction Order III High, well rounded Order IV Knife edge Order V Low, well rounded Order VI Depressed
PATHOLOGY OF RRR A frequent lay expression for RRR is “my gums have shrunk”. Actually, the basic structural change in RRR is a reduction in the size of the bony ridge under the mucoperiosteum. It is primarily a localized loss of bone structure. In some situations, this loss of bone may leave the overlying mucooperiosteum excessive and redundant. However, sometimes there is no redundant soft tissue in areas where severe bone loss has occurred.
Gross anatomic studies of dried jawbones have shown a wide variety of shapes and sizes of residual ridges. In order to provide a simplified method for categorizing the most common residual ridge configurations, a system of six orders of residual ridge forms have been described earlier. This self descriptive system is useful clinically as well as for research purposes and helps one to differentiate the various stages of RRR in the individual patient.
ü Another gross finding seen on dry specimens is that while external cortical surfaces of the maxilla and mandible are uniformly smooth, the crestal areas of residual ridge have a different appearances and show many more porosities and imperfections no matter at what stage of residual ridge configuration. ü Bones with the most severe RRR (Order V and VI) may display the gross porosity of medullary bone on the crest of the ridge and eventually may even display the uncovering of the inferior alveolar canal on the mandible. ü RRR does not stop with the residual ridge; but may go well below where the apices of the teeth were, sometimes leaving only a thin cortical plate on the inferior border of the mandible or virtually no maxillary alveolar process on the upper jaw.
ü However, a knife-edge may be masked by redundant or inflamed soft tissues. ü One can more accurately determine the amount of underlying bone by palpation in the mouth rather than by attempting to take measurements on stone casts. ü Lateral cephalometric radiography provides the most accurate method for determining the amount of residual ridge and the rate of RRR over a period of time. ü The panoramic radiographic technique described by Wical and Swoope is a simple, useful method for arriving at a gross estimate of the amount of RRR to date in a given patient. ü Clinically, the soft tissues, overlying residual ridges that have undergone RRR may range from normal to inflamed, edematous, ulcerated, indented or otherwise abused tissue.
PATHOPHYSIOLOGY OF RRR Ø It is a normal function of bone to undergo constant remodeling throughout life through the processes of bone resorption and bone formation. Except during growth, when bone formation exceeds bone resorption, bone resorption and bone formation are normally in equilibrium. Ø Osteoporosis is a generalized disease of bone in which bone is in negative balance, because bone resorption exceeds bone formation. Ø In periodontal disease, there is a localized destruction of the bone around teeth, perhaps due to certain local pathologic processes. In both generalized osteoporosis and localized periodontal disease, when bone matrix is lost it does not
Ø RRR is a localized pathologic loss of bone that is not built back by simply removing the causative factors. Ø To date, the process of RRR has not been reversed such that the residual ridge has increased in size. Yet the physiologic process of internal bone remodeling goes on even in the presence of this pathologic external osteoclastic activity that is responsible for the loss of so much bone substance. Ø New bone is laid down inside the residual ridge in advance of the external osteoclastic removal of bone. Ø RRR is not inevitable, and the rate of RRR varies, and that RRR can proceed far beyond the “alveolar bone, and that the rate of resorption in some patients is not much greater than the rate of formation that the patient ends up with no cortical bone on the crest of the ridge. From a practical point of view, RRR
ETIOLOGY OF RRR It is postulated that RRR is a multifactorial biomechanical disease that results from a combination of anatomic, metabolic, and mechanical determinants. Each of the major co-variables will be discussed separately and then will be brought together in a combined major variable formula. ANATOMIC FACTORS It is postulated that RRR varies with the quantity of the bone of the residual ridges. RRR Anatomic factors
Ø However, this must be interpreted carefully. It is to state that the more bone there is, the more RRR there will ultimately be, sometimes large ridges resorb rapidly and some knife-edge ridges may remain with little change for long periods of time. If a low depressed ridge has existed thus for many years, future RRR will probably be at a low rate. Ø Another way to evaluate the anatomic factors is to consider the mechanical factors that would be favorable to stability and retention of a denture. Thus, large well – rounded ridges and broad palates would seem to be favorable anatomic factors. Ø Still another anatomic factor to consider is the density of the ridge. However, here again one must interpret carefully, for the density at any given moment does not signify the current metabolic activity of the bone, and bone can be
METABOLIC FACTORS It is further postulated that RRR varies directly with certain systemic or localized bone resorptive factors and inversely with certain bone formation factors: RRR Bone resorption factors Bone formation factors
Ø RRR is a localized loss of bone on the crest of the residual ridge. It is quite possible that some of the local biochemical factors that have been studied in relation to periodontal disease could play an important role in RRR. Ø These factors include endotoxins from dental plaque (plaque can occur in edentulous mouths, especially in patients who do not properly clean their dentures), osteoclast activating factor (OAF), prostaglandins human gingival bone-resorption stimulating factor, and others. Ø Heparin, which has been shown to be a cofactor in bone resorption, has been associated with mast cells that have been observed in microscopic sections of residual ridges close to the bone margins.
Other possible local bone resorption factors could be related to trauma (especially under ill-fitting dentures), which leads to increased or decreased vascularity and changes in oxygen tension. Whatever the local bone resorbing factors may be, they must be considered in the environment of the systemic factors that influence the balance between normal bone formation and bone resorption. There are some patients who seem to have a natural resistance to unfavorable local factors whether it be calculus or bacteria; occlusal force in patients with natural teeth; or vertical dimension, cusp form, or other prosthetic factors in denture wearers.
Perhaps such individuals have the correct amounts of circulating estrogen, thyroxine, growth hormone, androgens, calcium, phosphorus, vitamin D, protein, fluoride, and so on to compensate for poor local factors, while others may be already in a negative bone balance owing to some form of osteoporosis and may therefore be more vulnerable to unfavorable local factors.
MECHANICAL FACTORS Though mechanisms are not yet clearly understood, the remodeling of bone is influenced by force factors. Bone that is used, as by regular physical activity, will tend to strengthen within certain limits, while bone that is in “disuse” will tend to atrophy. Once the teeth are removed, the residual alveolar ridge is subjected to entirely different types of forces. Some postulate that RRR is an “abuse” bone resorption due to excessive forces transmitted through dentures. Perhaps there is truth in both hypotheses. The fact is that with or without dentures some patients have little or no RRR and some have severe RRR.
In considering force, one must concern oneself not only with the amount of force, but also with the frequency of force, the duration of force, the direction of force, the area over which force is distributed (force per unit area), and the damping effect of the underlying tissue. Abnormal parafunctional forces from clenching and grinding of teeth may last may up to several hours per day. In some patients it is quite likely that this can place pathologic loads on the residual ridges. In summary, it is likely that force is a cofactor in RRR that can be expressed as: RRR force
A force applied to the bone may be affected inversely by the “damping effect” or energy absorption. This cofactor may be expressed as follows: RRR 1 Damping effect The “damping effect” may take place in the mucoperiosteum, which can be considered a visco-elastic material. Since the overlying mucoperiosteum varies in its visco-elastic properties among patients and from maxilla to mandible, its energy absorption qualities may influence the rate of RRR.
The fact that the maxillary residual ridge is frequently broader, flatter, and more cancellous than its mandibular counterpart is of interest and may be a factor in the frequently observed differences in the RRR of the two jaws. Frost pointed out that trabeculae in such bones as a vertebral body are oriented parallel to the direction of compression deformation, allowing for maximal resistance to deformation. The stronger these trabeculae are the greater is the resistance. The traditional design of dentures includes many features whose goal is to reduce the amount of force to the ridge and thereby to reduce RRR.
These prosthetic factors include Ø broad area coverage (to reduce the force per unit area decreased number of dental units, Ø decreased buccolingual width of teeth, and Ø improved tooth form (to decrease the amount of force required to penetrate a bolus of food); Ø avoidance of inclined planes (to minimize dislodgement of dentures and shear forces); Ø centralization of occlusal contacts (to increase stability of dentures and to maximize compressive forces); Ø provision of adequate tongue room (to improve stability of denture in speech and mastication); Ø adequate inter-occlusal distance during rest jaw relation (to decrease the frequency and duration of tooth contacts)
The various formulas describing the correlative relationship of possible factors the RRR must be combined if one is to more truly illustrate this concept. For simplicity, only the major categories of cofactors are included as follows: RRR anatomic factors + bone resorption factors + Force factors bone formation factors damping effect factors In addition to the three major categories of factors (anatomic, metabolic, and mechanical), the importance of the time since extraction to the bone loss curves, described in the section on the pathogenesis of RRR, should be emphasized by adding an inverse relation.
RRR 1 Time To the combined formula as follows RRR anatomic factors + bone resorption factors + force factors time bone formation factors damping effect
EPIDEMIOLOGY OF RRR Epidemiology is the study of the distribution and determinants of disease in man. Epidemiologic methodology can contribute to an understanding of the etiology of a specific disease, especially by the use of a large experimental population. There have been no large scale studies of RRR in man. Most studies of RRR to date have been meticulous longitudinal cephalometric studies of a relatively few subjects, while such studies are responsible for, much of what we know about RRR. They are time consuming and expensive and not really good examples of epidemiologic methodology.
To date it would appear that RRR is worldwide, occurs in males and females, young and old, in sickness and in health, with and without dentures, and is unrelated to the primary reason for the extraction of the teeth (caries or periodontal disease). Sometimes a disease is caused by a single determinant, sometimes by multiple factors. The resistance of the host to the causative or predisposing factors may affect the frequency or severity of a disease. Sometimes a certain dose of the causal factor is necessary to cause the disease. Sometimes the causal factor must be present a certain length of time to be effective. All of these factors tend to obscure the etiology of a disease.
TREATMENT OF RESIDUAL RIDGE RESORPTION Pre-prosthetic surgery includes the following: 1. Ridge preservation procedure as a preventive measure. 2. Corrective or recontouring procedures of the defects and abnormalities. 3. Ridge extension procedures: • Relative methods Eg. sulcus extension (vestibuloplasty) • Absolute methods Eg. Ridge augmentation methods. 4. Reconstruction methods like correction of abnormal ridge relationship.
5. Provision of accessory undercuts. • Creating favorable undercuts • Dental implants. • Onlay denture. 6. Modified denture construction procedure Eg. Immediate denture where construction of the denture proceeds surgery.
CONCLUSION Bone resorption of residual ridges is common. The rate of resorption varies among different individuals and within the same individual at different times. Factors related to the rate of resorption are divided into anatomic, metabolic, functions, and prosthetic factors. Anatomic factors include the size, shape and density of ridges, the thickness and character of the mucosal covering, the ridge relationships, and the number and depth of sockets.
Metabolic factors include all of the multiple nutritional, hormonal and other metabolic factors which influence the relative cellular activity of the bone-forming cells (osteoblasts) and the bone-destroying cells (osteoclasts). Age, sex and general health are inadequate to describe the bone factor but do give some clinical clues. Functional factors include the frequency, intensity, duration and direction of forces applied to bone which are translated into cellular activity, resulting in either bone formation or bone resorption, depending on the patient’s individual resistance to these forces.
Prosthetic factors include the myriad of technique, materials, concepts, principles and practices which are incorporated into the prosthesis. Although the various factors can be divided into these five groups for academic purpose, they are interrelated any one factor may be evaluated only if we place it in its proper perspective to all factors. Since bone resorption depends on the response of living cells to force, the more basic sciences concerned with the physiology and pathology of cells are understood, the more educated will be our clinical judgment.