Renal transplantation with pregnancy Dr Abd ElNaser Abd

Renal transplantation with pregnancy Dr. Abd El-Naser Abd El-Gaber Ali Assist. Prof. of obstet. & Gynecol.

Introduction �End-stage renal disease can have adverse impact on the quality of life. Plans for education, work and family are often interrupted or stopped completely as patients cope with illness and the demands of treatment. �Kidney transplantation not only decrease mortality rate but it can increase opportunities of patients for life and achieve her dreams

Annual patient mortality After Kidney Transplantation VS haemodialysis �With dialysis 21%-25% �With cadaveric transplant donors <8% �With living-related transplant donors < 4%.
 had the idea")
History of Renal Transplantation �in 1907 Simon Flexner (American medical researcher) had the idea of renal transplantation theoretically. �In 1933 surgeon Yuriy Voroniy attempted the first human kidney transplant, using a kidney donor to be reimplanted into the thigh. His first patient died 2 days later as the graft was incompatible with the recipient's blood group and was rejected

�In 1950, a successful transplant was performed on Ruth Tucker, a 44 -year-old woman with polycystic kidney disease, Although the donated kidney was rejected ten months later because no immunosuppressive therapy was available at the time. �The first kidney transplants between living patients were undertaken in 1952 by Jean Hamburger in Paris �The first kidney transplantation in the United Kingdom did not occur until 1960
,")
Indications of renal transplatation �The indication for kidney transplantation is end-stage renal disease (ESRD), regardless of the primary cause. This is defined as a glomerular filtration rate <15 ml/min �Common diseases leading to ESRD include: �Malignant hypertension, infections, diabetes mellitus, and focal segmental glomerulosclerosis, genetic causes as polycystic kidney disease,
")
Types of Kidney Donor n Living related. n Living unrelated n Cadaveric (Brain dead) Beating and non-beating heart ( on artificial machine)

CRITERIA FOR LIVING DONOR SELECTION - - 1 -Blood relative. 2 -ABO blood group-compatible. 3 -HLA typing: HLA-identical (siblings of monozygotic)HLA Haploidentical (siblings, parents, children, relatives) HLA Less than haploidentical (Relatives) Distant donors with negative cross-match. 4 -Excellent medical condition with normal renal function.

CRITERIA FOR CADAVER DONOR SELECTION - Irreversible brain damage. Normal renal function appropriate for age. No evidence of preexisting renal disease. No evidence of transmissible diseases. ABO blood group-compatible. Negative cross-match. HLA match if possible

Evaluation Of Target Kidney Function In Potential Kidney Donor n n n Serum creatinine. Creatinine clearance. Radionuclide glomerular filtration rate. Urine analysis. Urine Culture. GFR > 70 ml/min

What about future donor health ? n Following nephrectomy, compensatory hypertrophy and increase in GFR occur in the remaining kidney. n Slight risk of poteinuria and hypertension. n Meta-analysis of data from donors followed for >20 y confirmed safety of kidney donation

Matching between Recepient And Donor �Tissue typing: �Cross matching �Compatible ABO blood group
 �Human leukocyte antigen (HLA) is genes of chromosome 6 present on")
Tissue typing (HLA) �Human leukocyte antigen (HLA) is genes of chromosome 6 present on the surface of cells that are responsible for regulation of the immune system in humans. �The HLA genes are the human versions of the major histocompatibility complex (MHC) genes �MHC class I (A-B-C) are expressed on the surface of most nucleated cells. �MHC class II (DP, DQ, and DR) are expressed on surface of Antigen-presenting cells (APC) and activated lymphocytes. �The match between donor and recipient can range from 0 to 6.

Oraganization of the human HLA genes on chromosome 6.

Cross matching �A laboratory test that determines weather a potential transplant recipient has preformed antibodies against the HLA antigens of the potential donor. (Donor Lymphocytes +Recipient Serum)

Compatible ABO blood group.

If a potential living donor is incompatible with his recipient, what can we do? �Kidney exchange : The donor could be exchange for a compatible kidney also known as "kidney paired donation“ �Desensitization protocols (plasmapheresis) utilizing intravenous immunoglobulin (IVIG) have been developed, with the aim to reduce ABO and HLA antibodies that the recipient may have to the donor

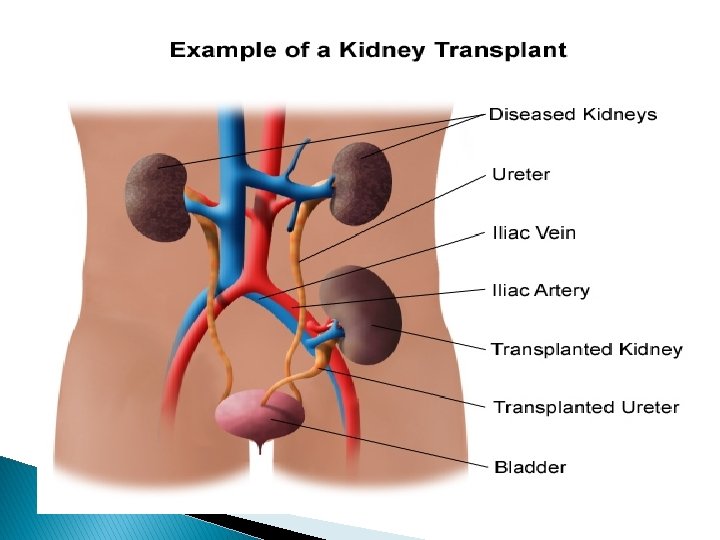
Procedure � Original kidneys are not removed, to minimize rate of surgical morbidities. The new kidney is placed extraperitoneally in iliac fossa. � Contralateral iliac fossa is preferred to ensure the renal pelvis and ureter are anterior in the event that future surgeries are required. Some textbooks recommend using the right side because the right vessels are “more horizontal” with respect to each other and therefore easier to use in the anastomoses � The renal artery of the new kidney, is often connected to the external iliac artery in the recipient and renal vein is often connected to the external iliac vein in the recipient

An adult donor kidney transplanted to the left iliac fossa of an adult recipient.

Elapsed time for renal graft to do its job �Living donor kidneys normally require 3– 5 days to reach normal functioning levels. �Cadaveric donations stretch that interval to 7– 15 days. �Hospital stay is typically for 4– 7 days.

Lifetime of renal graft �The average lifetime for a donated kidney is 10 -15 years. � When a transplant fails, a patient may prepared for a second transplant, and may have to return to dialysis for sometimes.

Factors Influencing The Longivity Of Renal Allograft �Age �HLA matching �Delayed graft function �Ischemia time. �Number of acute rejection episodes. �Native kidney disease.
 �Infections due to the immunosuppressant")
Complications of renal transplantation �Rejection (hyperacute, acute or chronic) �Infections due to the immunosuppressant drugs �Post-transplant lymphoproliferative disorder (a form of lymphoma due to the immune suppressants) �Imbalances in electrolytes including calcium and phosphate which can lead to bone �Proteinuria �Other side effects of medications as ulceration of the stomach and esophagus, hirsutism, hair loss, obesity, acne, diabetes mellitus type 2,

What Are The Most Common causes Of Death After Kidney Transplantation? n Cardiovascular disease. n Infection.

Renal Allograft Rejection 1 - Hyperacute. 2 - Acute. 3 - Chronic

Hyperacute Rejection n Humeral immunity is responsible n Is mediated by preformed antibodies that recognize HLA antigens in donor organ. n Usually these are formed as a consequence of blood transfusion, prior organ transplantation, autoimmune diseases. n Fibrinoid necrosis lead to immediate graft loss. n Delayed form may occur several days following transplantation. n Plasmapheresis pulse steroid may be used.

Acute Renal Allograft Rejection n Cellular immunity is responsible n IS mediated by activated T-lymphocytes. n Activations of T-cells occur after recognition of graft antigen. n This usually occur during the first 6 months. n It manifest as increase in s. creatinine with or without oliguria.

Chronic allograft Rejection �The term chronic rejection initially described long-term loss of function in transplanted organs via fibrosis of the transplanted tissue's blood vessels. �A- Immunologic �B- Non-lummunologic • Hypertension • Hyperlipidemia • Drug toxicity • Ischaemic injury • Viral infection (CMV)


Banff criteria for diagnosis of allograft rejection BANFF GRADE I HISTOLOGY Interstitial edema and tubulitis (i. e. , lymphocytic invasion of tubular basement membranes. II More severe tubulitis with or without mild vasculitis characterized by intimal lymphocytic infiltrates III Severe vasculitis with fibrinoid necrosis.

Pregnancy outcome in patients with renal transplant

�How much this problem affect our society ? �Another question what is the incidence of transplanted kidney among Egyptian pregnant women ?

�No statistics can tell us, but in our mind we think in incidence about zero why? �Social aspect �Medical aspect

�Chronic renal failure patients suffer from loss of libido, anovulatory vaginal bleeding or amenorrhea and high prolactin levels. �On dialysis (decreased libido and Conception is rare). It occurs at a rate of no more than one in every 200 patients. �Fertility is usually restored in women with renal transplants. Pregnancy is then common, occurring in 12% of women at childbearing age in one series. Pregnancy success rate exceeds 90% after the first trimester

What is the Proper time for patient with renal transplant to get pregnant ? 1 - The American Society of Transplantation (AST) recommends delay pregnancy 1 year or more (1 year after living related transplant and 2 years post cadaver transplant) to avoid rejection 2 - No rejection over the last year. 3 - Graft has good function: serum creatinine <1. 5 mg/ml, good GFR, minimal or no proteinuria (proteinuria < 500 mg/d). 4 - BP ≤ 140/90 mm. Hg on medications 5 - Maintain stability of immunosuppressive drugs doses. 6 - Normal allograft ultrasound

Factors that affect pregnancy outcomes �Good general health for about 2 years after transplantation �No graft rejection in the last year �Adequate and stable graft function �No acute infections that might affect the fetus �Maintenance immunosuppressant at stable doses �Patient compliance with treatment and follow-up �Normal or controlled blood pressure with one medication �Normal allograft ultrasonography results

Evidences of well graft function �Serum creatinine level less than 1. 5 mg/d. L �Proteinuria level less than 500 mg/d �Normal appearance of allograft ultrasonography �Blood pressure within the reference range �No recent episodes of acute rejection

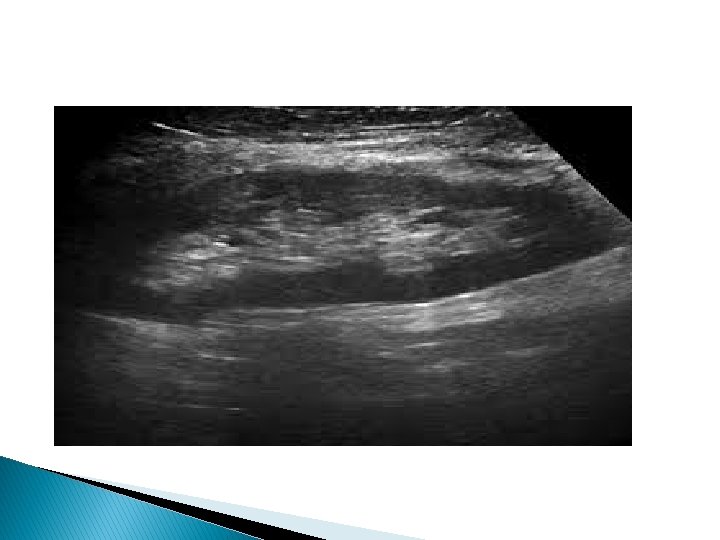
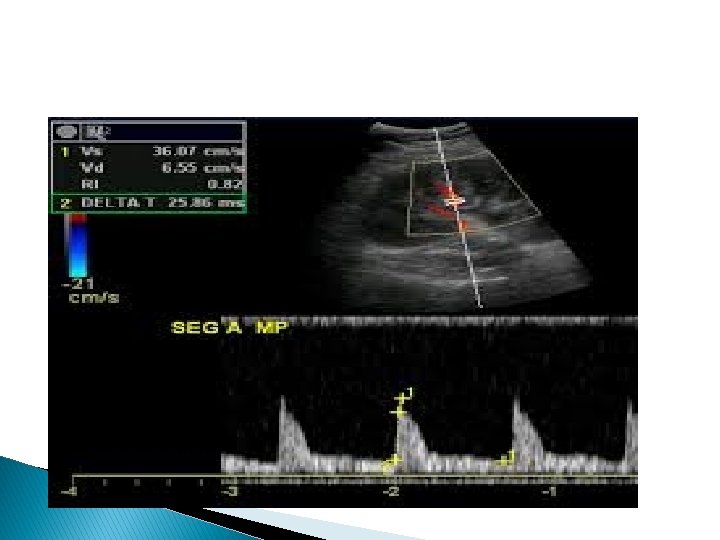
Ultrasonographic assessment of Transplanted Kidney �A baseline US evaluation is performed in the first 24– 48 hours post transplantation. �A detailed examination protocol includes � renal size and echogenicity, � collecting system and ureter condition � evaluation of any postoperative collections. � Color Doppler should assess flow in the renal and iliac vessels, flow velocity measurements, as well as evaluation of the intrarenal vessels. “using (RI), (PI), and S/D ratio.
 Good contrast resolution between cortex and medulla.")
Ultrasonographic Features of Kidney Transplants � (a) Good contrast resolution between cortex and medulla. � (b) Normal renal artery and vein on color Doppler ultrasound. � (c) Normal homogeneous blood flow throughout the transplant kidney on color Doppler ultrasound. Interlobar, arcuate, and the peripheral cortical branches are illustrated. � (d) Normal renal artery and vein waveforms on spectral Doppler ultrasound. � (e) Normal intrarenal artery waveform on spectral Doppler �.
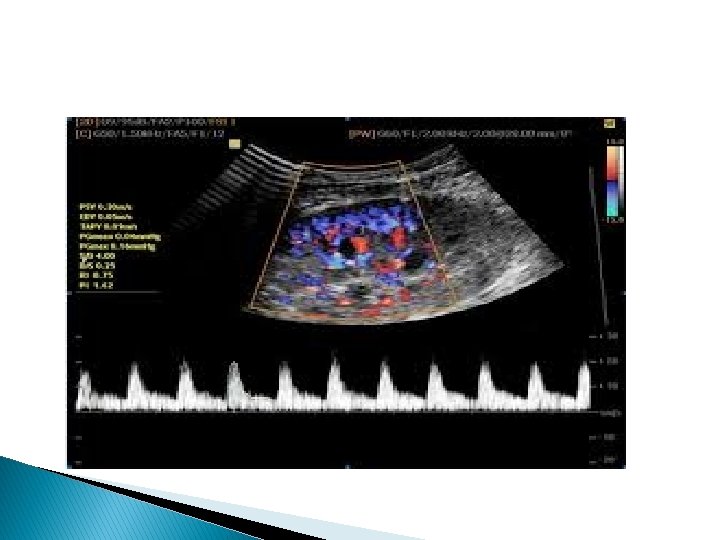

Color Doppler of renal graft �Image show homogeneous vascularity of the entire graft. Duplex color Doppler

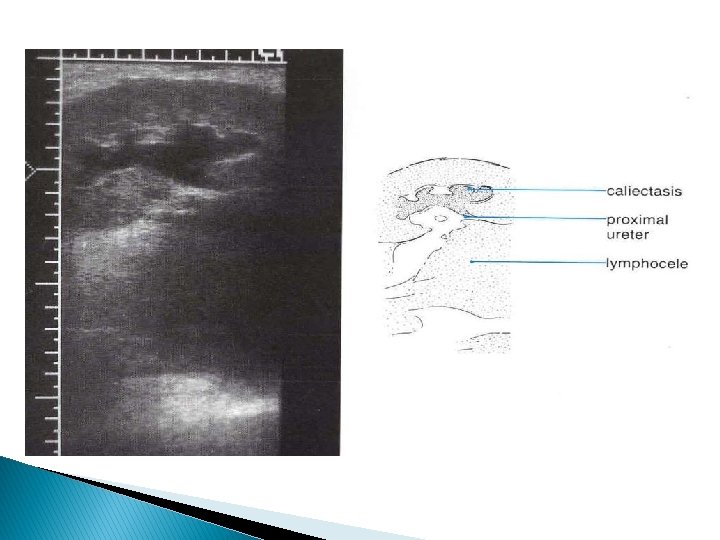
Ultrasound features for dysfunctioning renal graft �Kidney enlargement, hyper- or hypoechogenicity �Doppler may reveal high PI and RI values (>0. 9) �In very serious cases, reversed diastolic flow in renal artery may be seen



Color Doppler of renal graft �Renal infarct. Power Doppler image post operative day 1

Co-morbid factors that may worsen pregnancy outcomes �Etiology of previous renal disease (ie, risk of recurrence) �Chronic graft dysfunction �Renal insufficiency �Cardiopulmonary diseases �Hypertension �Diabetes mellitus �Obesity �Maternal infection with hepatitis B or C

Effect of pregnancy on renal graft �Increases risk of graft rejection if Cr > 1. 5 mg/dl before pregnancy. �Decrease in creatinine clearance & increase proteinuria �Pregnancy causes an increase in the glomerular filtration rate. In theory, this could lead to hyperfiltration and glomerulosclerosis.

Effect of renal transplatation on Pregnancy outcomes �Increase incidence of abortion, preterm labor and IUGR �Increased incidence of congenital anomalies due to immunosuppressive drugs. �Increase incidence of pregnancy induced hypertension as preeclampsia.

Obstetrical manegement �Counseling: All women of childbearing age should be counseled concerning the possibility and risks of pregnancy after kidney transplantation �Women are usually advised to wait at least 1 year after living related donor transplantation and 2 years after cadaver transplantation. �Graft should preferably be functioning well (stable Cr < 1. 5 mg/dl, proteinuria < 500 mg/d)
. �No hospital admission routinely.")
Obstetrical manegement �Increase frequency of prenatal visit (every 2 weeks). �No hospital admission routinely. �Early treatment of asymptomatic bacteriuria �Renal function tests monthly �Early detection of pre eclampsia �Aggressive management of hypertension: The drug of choice is methyldopa; methyldopa second-line agents beta blockers and calcium channel blockers (angiotensin-converting enzyme inhibitors and angiotensin receptor blockers are contraindicated)

Obstetrical manegement �Aggressive treatment of any infection �Screening and treatment of asymptomatic bacteriuria �Close monitoring of graft function; if rejection is suspected, consider biopsy �In cases of acute rejection, steroids are the preferred drugs and dose should be increased. �Transplant medications should not be reduced during pregnancy (pregnancy is immunosuppressive state wrong belief).
: spontaneous or induced labor. �Minimize instrumentations �Increased steroid dose")
Obstetrical manegement �Vaginal delivery (preferred): spontaneous or induced labor. �Minimize instrumentations �Increased steroid dose at onset of labor to overcome the stress of labor and prevent postpartum rejection �Cesarean delivery is only indicated for obstetric reasons (in such cases, avoid injury to the ureter of transplanted graft by knowing its exact location) �Antibiotic prophylaxis for all surgical procedures
.")
Obstetrical manegement �Breastfeeding �Only allowed with immunosuppressive drugs (azathioprine and prednisone).

Selection of Contraceptive method �COCs: Low dose oestrogen–progesterone oral contraceptive preparations are advised. �IUCD: is contraindicated because: 1 -The risk of infection from the use of intrauterine devices is increased in immunocompromised patients. 2 -The efficacy of IUDs may be reduced because of the anti‐inflammatory properties of immunosuppressive agents. �Barrier methods are preferred

ART in patient with renal graft �ART can be applied for infertile couple with female renal transplantation �Incidence of ovarian hyperstimulation syndrome is high

Graft dysfunction in pregnancy �Diagnose of Rejection is difficult because Cr falls somewhat during pregnancy �Ureteric obstruction from a gravid uterus �Cyclosporine may cause Thrombotic thrombocytopenic purpura and HUS Hemolytic -uremic syndrome Treatment �Methylprednisolone is the recommended treatment of rejection �IVIg has been used a fair amount without problems

kidney biopsy during pregnancy �Data for native kidneys before transplantation �Diagnosis of renal rejection �Can be done safely in women with well-controlled blood pressure �Biopsy after 32 weeks is not recommended except if there were signs of rejection.

What about donor if get pregnant ? �Hyperfiltration of compensated kidney during pregnancy. �Normal renal function

Transplant Immunosuppression medications with pregnancy �Most centers maintained pregnant patients on two or three drug regimens with various combinations of calcineurin inhibitors, prednisone and azathioprine. �Mycophenolate mofetil (MMF) and sirolimus used infrequently

Some commonly used combinations of maintenance Immunosuppressive drugs 1 - Prednisolon + Azathiaprine 2 - Prednisolon + cyclosporine 3 - Prednisolon + cyclosporine + Azathioprine 4 - Mycophenolate mofetil (MMF) may replace Azathioprine. 5 - Sirolimus may replace Azathioprine or cyclosprine

Steroids �Prednisone associated with a variety of birth defects ( mainly if doses > 20 mg/d) �prednisolone can cross the placenta, but maternal‐ to cord‐blood ratios are approximately 10: 1 �Fetal adrenal insufficiency and thymic hypoplasia if dose > 15 mg/day �Increased risk of cleft palate �Possible increased risk of PROM & IUGR �Increased maternal infection �Glucocorticoids are excreted in breast milk (small amounts),

Azathioprine �low birth weight, �Prematurity �Neonatal jaundice �Respiratory distress syndrome

Cyclosporine �Has no effect on organogenesis �Can induce/worsen hypertension, maternal diabetes �Drug levels may fall during pregnancy lead to graft dysfunction and rejection �Increase incidence of Preterm labor and IUGR �Small amount passes through placenta
 �Its serum level increased")
Tacrolimus �Causes preterm labor in 60% �Possible malformations (no pattern) �Its serum level increased during pregnancy due to inhibition of hepatic cytochrome P 450 enzymes �Levels in breast milk similar to that in maternal serum not recommended during lactation

Sirolimus �Should be discontinued >/= 12 weeks before conception �Recommend switch to cyclosporine if planning to conceive and switch back following delivery. �Increase incidence of congenital anomalies �Increase incidence of abortion

Mycophenolate mofetil �Increases 1 st trimester pregnancy loss �Congenital malformations (cleft lip/palate, anomalies of distal limbs, heart, esophagus, kidneys) �Excreted into breast milk so stop lactation or shift to another drug.

Conclusions �Fertility return after transplant with a pregnancy success rate of more than 90% after the first trimester �Neither low dose prednisolone or azathioprine appear to have adverse effect on the fetus �There is slight increase in spontaneous abortion and intrauterine growth retardation �Pregnancy has no important early effect on renal function and affected by the same factors in pregnancy in patients with renal impairment

Thank You
- Slides: 72