RENAL REPLACEMENT THERAPIES 1 Hemodialysis PURPOSES OF DIALYSIS











- Slides: 13
RENAL REPLACEMENT THERAPIES 1 - Hemodialysis
PURPOSES OF DIALYSIS 1. Removes excess fluids and waste products. 2. Restores chemical and electrolyte balance
HEMODIALYSIS ‑ One of several renal replacement therapies used for the treatment of renal failure. HD involves the extracorporeal (outside of the body) passage of the client’s blood through a semi permeable membrane that serves as an artificial kidney.
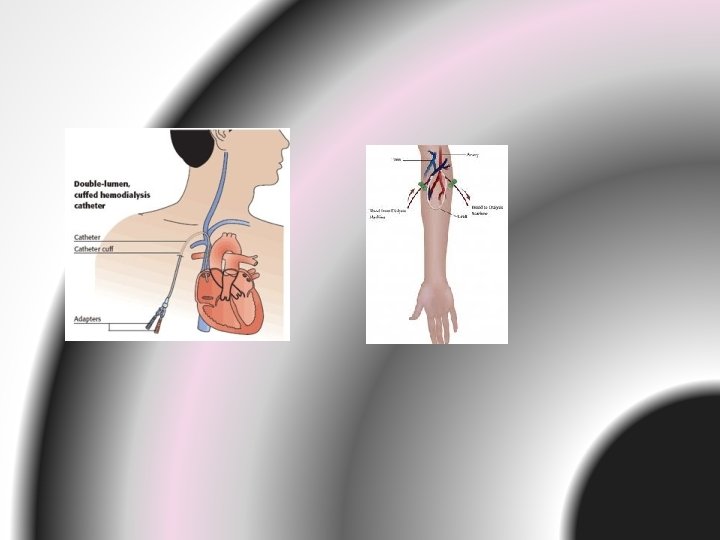
Components of Hemodialysis -Dialyzer or artificial kidney - Blood compartment -Dialysate – made up of clear H 2 O & chemicals. Prevent decrease in pt’s blood temperature. -Vascular access routes – AV fistula, AV Graft, Dual Lumen Cathater, AV Shunt. -Hemodialysis machine.
TYPES OF VASCULAR ACCESS FOR HEMODIALYSIS
Caring for the client Undergoing Hemodialysis -Weigh the client before and after dialysis. -Know the client’s dry weight. -Discuss with physician whether any of the client’s medications should be withheld until after dialysis. -Be aware of events that occurred during the dialysis treatment. -Measure blood pressure, pulse rate, respirations, and temp. -Assess for symptoms of orthostatic hypotension. -Assess the vascular access site. -Observe for bleeding -Assess the client’s level of consciousness and assess for headache, nausea, and vomiting-
PROCEDURE -The principles of HD are based on the passive transfer of toxins, which is accomplished by diffusion. -When HD is initiated, blood and dialysate flow in opposite directions from their respective sides of an enclosed semi permeable membrane. The dialysate is a balanced mix of electrolytes and water that closely resembles human plasma. On the other side of the membrane is the client’s blood, which contains metabolic waste products, excess water, and excess electrolytes.
-During HD, the waste products move from the blood into the dialysate because of the difference in their concentrations (diffusion). Excess water is also removed from the blood into the dialysate (osmosis). Electrolytes can move in either direction, as needed, and take some fluid with them. Potassium and sodium typically move out of the plasma. This process continues as the blood and the dialysate are circulated past the membrane for a preset length of time.
-Duration and frequency of HD tx depend on the amt of metabolic waste to be cleared, and the amt of fluid to be removed.
COMPLICATIONS OF HEMODIALYSIS Dialysis disequilibrium syndrome- the cause is unknown but maybe due to rapid decrease in blood urea nitrogen levels during HD. These change can cause cerebral edema- leads to increase intracranial pressure. Infection- transmitted by blood transfusion are another serious complication associated with long term HD. Hepatitis Infection- in clients with chronic renal failure.