Renal Denervation CRT 2013 Applications beyond hypertension management

Renal Denervation @ CRT 2013 Applications beyond hypertension management Felix Mahfoud Klinik für Innere Medizin III Kardiologie, Angiologie und Internistische Intensivmedizin Universitätsklinikum des Saarlandes Germany

Felix Mahfoud, MD Medtronic, St. Jude, Vessix, Re. Cor, Cordis X Research contracts X Consulting fees

Local versus systemic effect? ?
 p<0. 01 Hering D et al,")
-37% Single unit MSNA per 100 hearts bearts) p<0. 01 Hering D et al, Hypertension 2012

Effect of renal denervation on hypertensive endorgans and comorbities Diabetes LVH Diastolic function Heart rate Arrhythmias Renal function Renal hemodynamics Albuminuria

Myocardial effects

N=64 Brandt MC, Mahfoud F, et al, JACC 2012

Greater LV mass reduction in patients with LVH N=64 Brandt MC, Mahfoud F, et al, JACC 2012

Improvement in diastolic function Brandt MC, Mahfoud F, et al, JACC 2012
 4 HR 1. Tertile HR 2. Tertile HR 3.")
Change of heart rate (bpm) 4 HR 1. Tertile HR 2. Tertile HR 3. Tertile HR ≤ 60 bpm HR 61 -71 bpm HR ≥ 71 bpm p=0. 035 p=0. 113 n=120 2 0 3 months -2 6 months -4 p=0. 008 p=0. 035 -6 -8 -10 -12 p<0. 0001 p=0. 002 ANOVA 3 months: p<0. 0001 ANOVA 6 months: p<0. 0001 Ukena C, Mahfoud F, et al, Int J Card 2012

No correlation between change of heart rate and change of SBP Response to SBP: reduction of ≥ 10 mm. Hg Change of heart rate (bpm) 40 30 20 10 0 Response to HR: reduction of ≥ 3 bpm -10 -20 -30 -40 -100 r = 0. 07 p = 0. 455 -80 -60 -40 -20 0 20 40 Change of SBP (mm Hg) Ukena C, Mahfoud F, et al, Int J Card 2012

Sympathetic activity correlates to NYHA class • CHF is characterized by increased SNS activity – proportional to severity of CHF Normal Subject MSNA 10. 4 bursts/min NYHA functional class II MSNA 18. 8 bursts/min NYHA functional class III MSNA 67. 4 bursts/min NYHA functional class IV MSNA 99. 4 bursts/min Ferguson D, JACC 1990

Cardiac and renal spillover in heart failure Rundqvist B. , Circulation 1997; 95: 169 -75.

REn. Al Denerv. Ation in Patien. Ts with chronic heart failure – The RE-ADAPT-CHF study • International, multicentre, randomized trial 50 Control 6 M Randomization Baseline SBP≥ 100 Primary Endpoint Treatment 6 M 50 Following collection of the primary endpoint at 6 months, control patients permitted to cross-over 12 -36 M

REn. Al Denerv. Ation in Patien. Ts with chronic heart failure – The RE-ADAPT-CHF study Inclusion criteria • 100 patients with CHF in NYHA class II-III • LV-EF <40% • e. GFR >30 ml/min/1. 73 m 2 • Optimal and stable medical therapy

Atrial fibrillation

Higher sympathetic activity in patients with CHF+AF compared to CHF+SR N=21 Ikeda T et al, J Physiol 2012
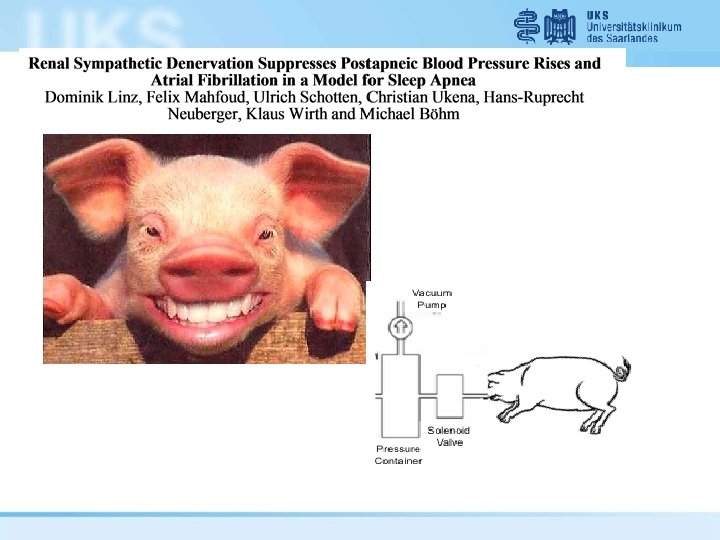

Effect of RDN on postapneic blood pressure rises Linz D et al, Hypertension 2012

RDN reduces AF inducibility Normal breathing 2 -min of NTP at -80 mbar after Atenolol 2 -min of NTP at -80 mbar after RDN Linz D et al, Hypertension 2012

RDN reduces AF inducibility Normal breathing 2 -min of NTP at -80 mbar after Atenolol 2 -min of NTP at -80 mbar after RDN Linz D et al, Hypertension 2012

RDN reduces AF inducibility Normal breathing 2 -min of NTP at -80 mbar after Atenolol 2 -min of NTP at -80 mbar after RDN Linz D et al, Hypertension 2012

RDN reduces AF inducibility Normal breathing 2 -min of NTP at -80 mbar after Atenolol 2 -min of NTP at -80 mbar after RDN Linz D et al, Hypertension 2012
 SHAM RDN p=0. 002 ECG SHAM n. s. Atrial MAPs Atrial")
Atrial CL (ms) SHAM RDN p=0. 002 ECG SHAM n. s. Atrial MAPs Atrial Tachypacing Linz D et al, Hypertension 2012
 SHAM RDN p=0. 002 ECG SHAM n. s. Atrial MAPs RDN")
Atrial CL (ms) SHAM RDN p=0. 002 ECG SHAM n. s. Atrial MAPs RDN Ventricular CL (ms) Atrial Tachypacing RDN ECG SHAM p=0. 002 p=0. 001 Atrial MAPs Atrial Tachypacing 1 sec. Linz D et al, Hypertension 2012

• Key inclusion • • Paroxysmal or persistent AF Resistant hypertension (SBP >160 mm. Hg) • Randomization (n=27) • 1: 1 PVI alone vs. PVI + RDN

PVI + RDN in Afib – 12 months results • RDN resulted in • BP reduction -25/-10 mm. Hg • 69% of patients after RDN were AF-free compared to 29% in the PVI-only group

Pleiotropic effects of renal denervation Efferent Afferent OSA Diabetes Mahfoud F, Circulation 2011 Schlaich M, J Hypertens 2011 Witkowski A, Hypertension 2011 Linz D, Hypertension 2012 Witkowski A, Hypertension 2011 Myocardial function Brandt MC, Mahfoud F, JACC 2012 Ukena C, Mahfoud F, Int J Card 2012 Renal function Linz D, Mahfoud F, Hypertension 2012 Hering D, Mahfoud F, JASN 2012 Davis J, Int J Card 2012 Mahfoud F, Hypertension 2012 Pokushalov E, JACC 2012

Quo vadis. . . Chronic kidney disease Obstructive sleep apnea Chronic heart failure Insulin resistance and diabetes Arrhythmias Hypertension

Thank you! Dr. Felix Mahfoud Klinik für Innere Medizin III Universitätsklinikum des Saarlandes Homburg/Saar, Germany Tel. +49 6841 -16 -21346 Fax. +49 6841 -16 -13211 felix. mahfoud@uks. eu
- Slides: 30