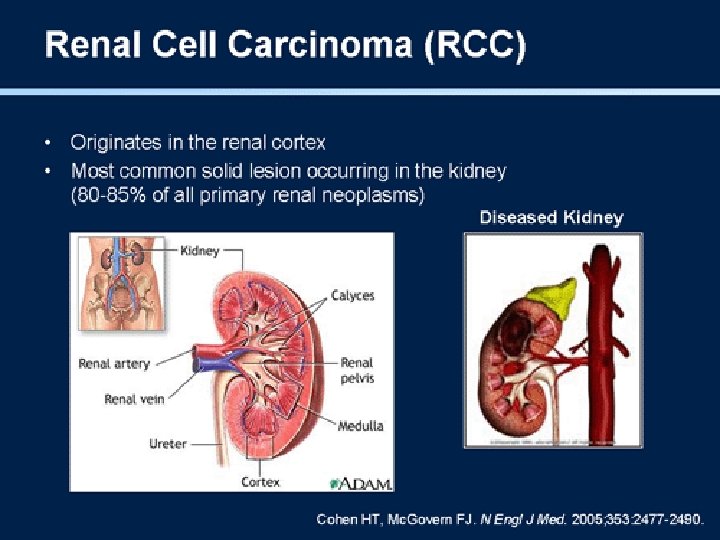
Renal cell carcinoma By Dr Abeer Elsayed Aly

Renal cell carcinoma By Dr. Abeer Elsayed Aly Lecturer of medical oncology SECI 18/3/2013
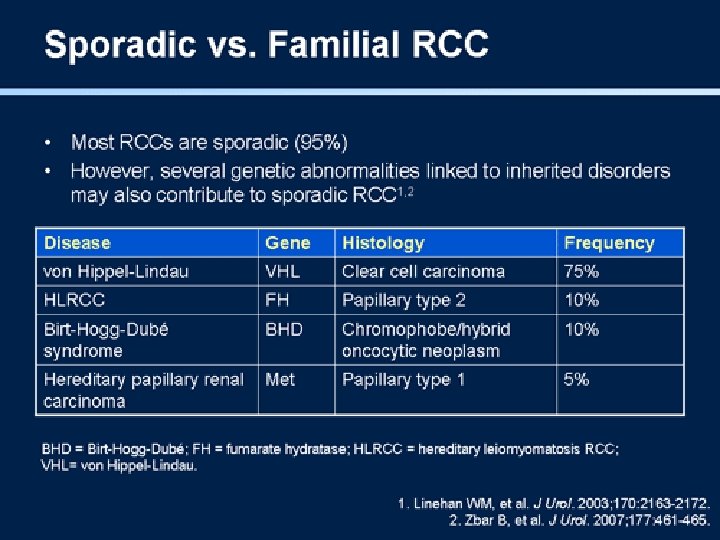

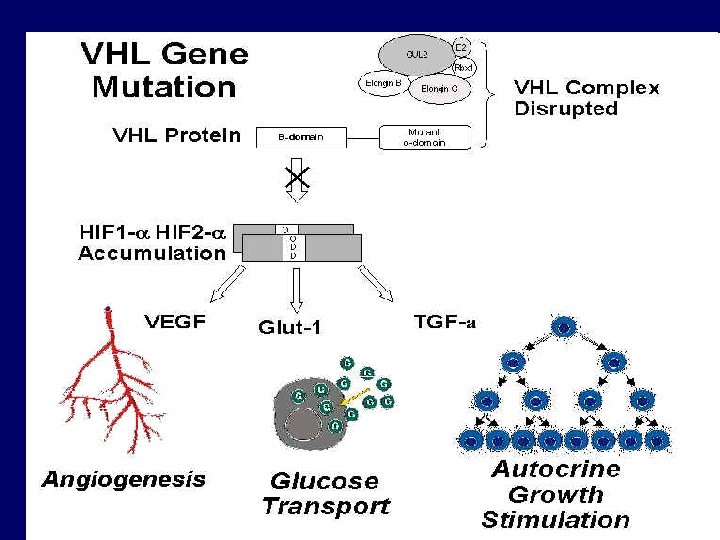
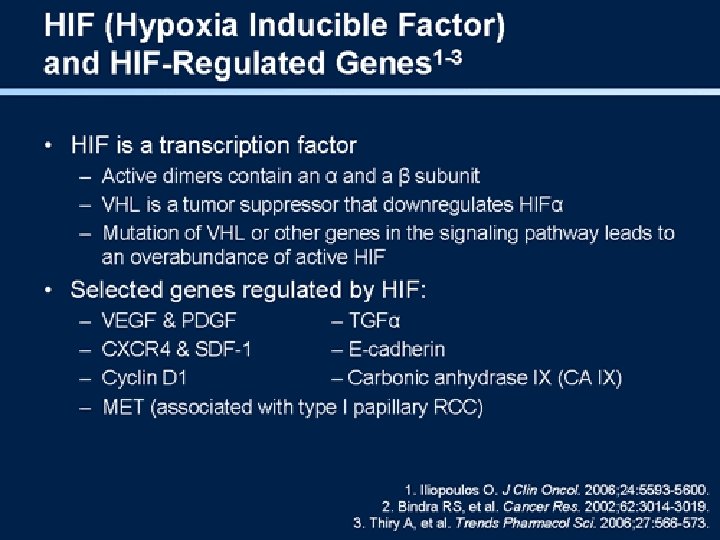
von Hippel-Lindau syndrome • • Autosomal dominant Multiple cancers RCC in nearly 40% of patients del (3 p) or t (3; 6) or t (3; 8) => VHL gene (3 p 26 -p 25) mutated => accumulation of hypoxia inducible factors (HIFs) that stimulate angiogenesis through VEGF and VEGFR

Hereditary papillary renal carcinoma • AD • bilateral, multifocal papillary renal carcinoma • Germline missense mutations in the tyrosine kinase domain of the MET gene (7 q 31) => constitutive activation • TFE 3 mutation • t(X; 1)(p 11; q 21)

MET • β-subunit of c-Met product is the cellsurface receptor for hepatocyte growth factor • amplified during the transition between primary tumors and metastasis • metastatic potential relies on the properties of its multifunctional docking site • PRC commonly show trisomy of ch. 7

Familial renal oncocytoma • usually benign tumors • Ultrastructural characterization exhibits dense packing of the cells with mitochondria that show morphologic differences from those in normal cells [larger, abnormally shaped] • Mutation in mt. DNA within the Cy. C oxidase subunit I gene
![BIRT-HOGG-DUBE SYNDROME • BHD gene 17 p 11. 2 [TS] • Adult onset •](http://slidetodoc.com/presentation_image_h/bae860ff94e8efcb93d87e114409e4d5/image-10.jpg "BIRT-HOGG-DUBE SYNDROME • BHD gene 17 p 11. 2 [TS] • Adult onset •")
BIRT-HOGG-DUBE SYNDROME • BHD gene 17 p 11. 2 [TS] • Adult onset • male-to-male transmission


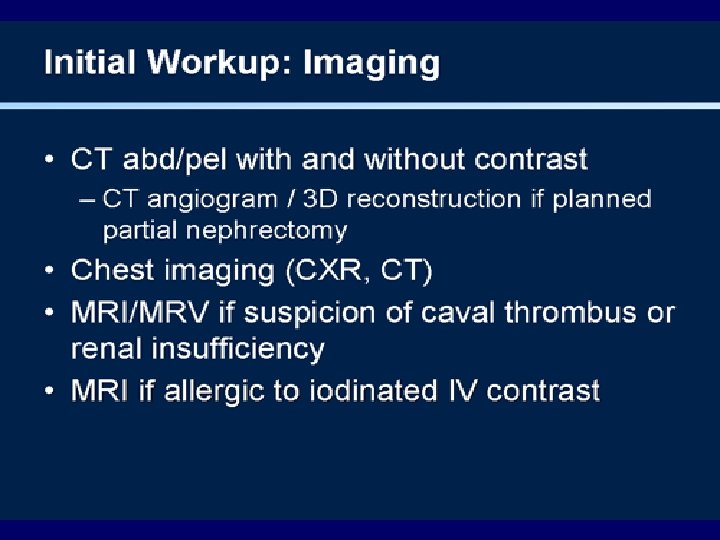
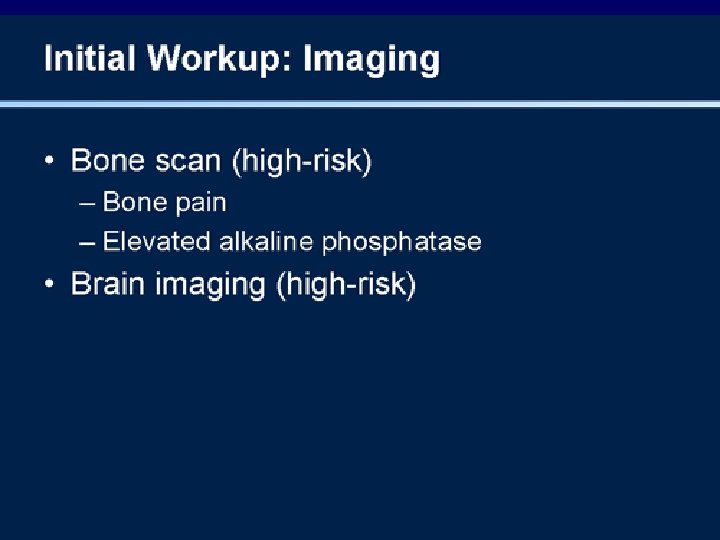
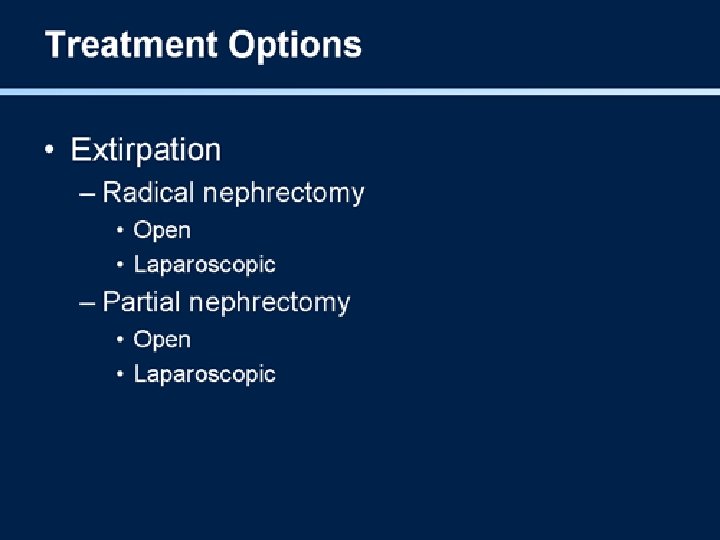
Treatment of early stages

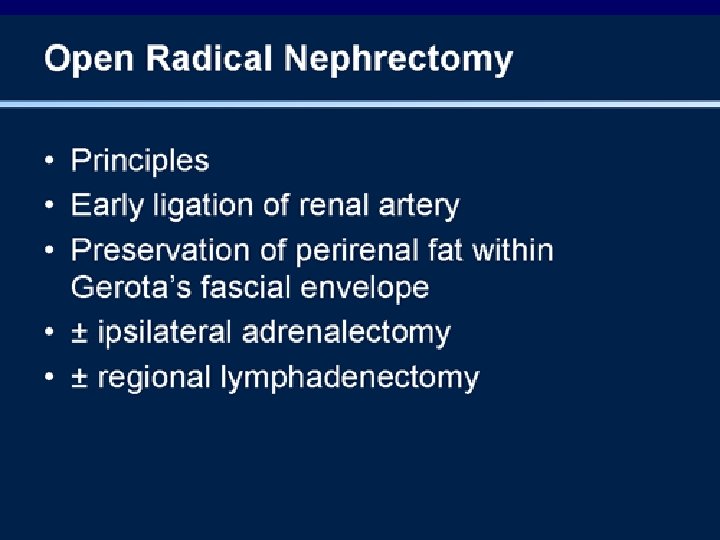
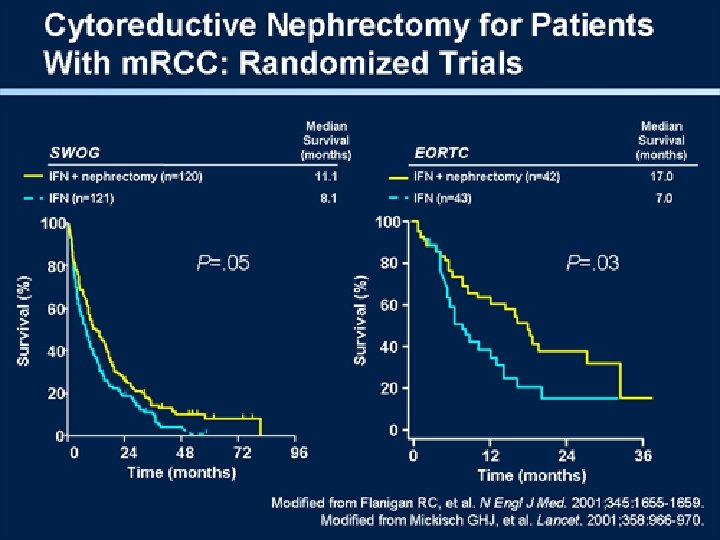
Nephrectomy

What about adjuvant therapy?

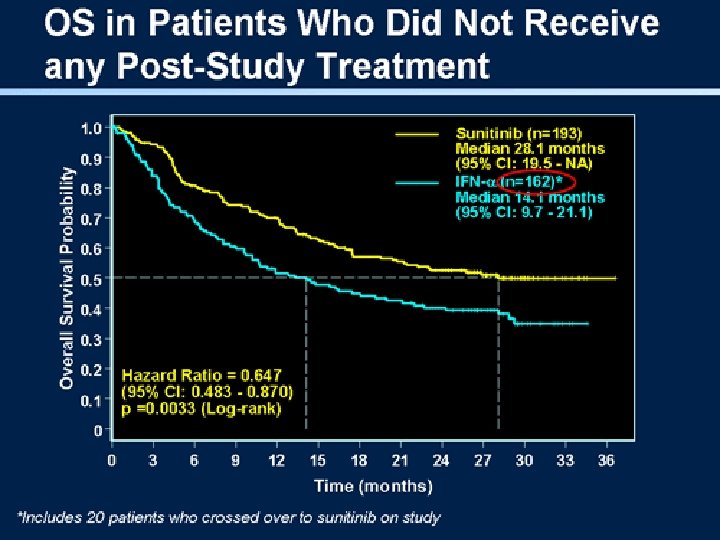
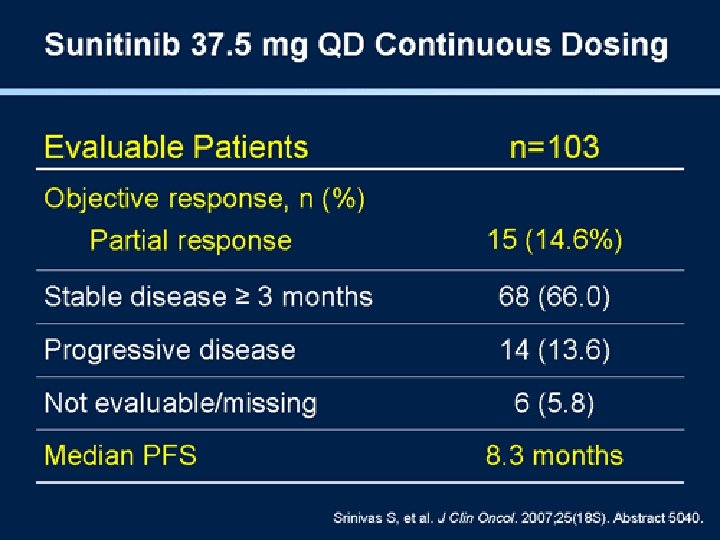
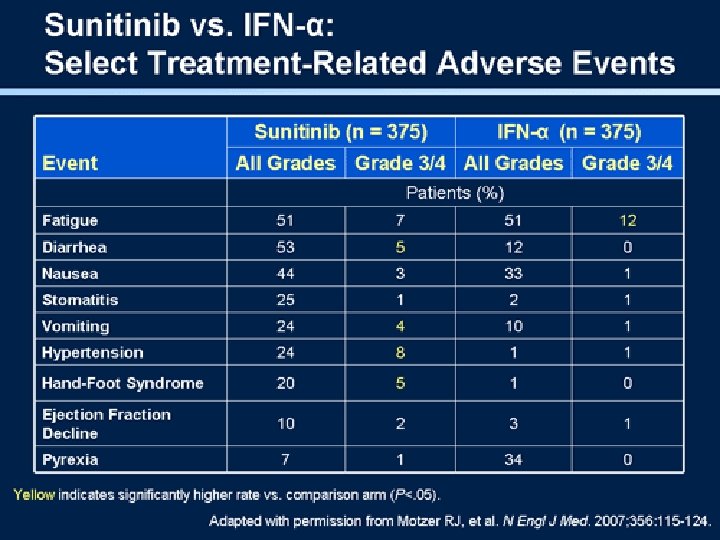
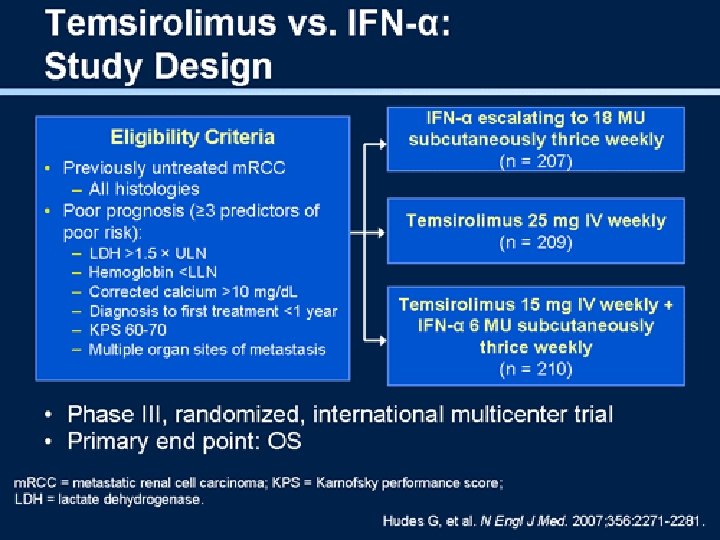
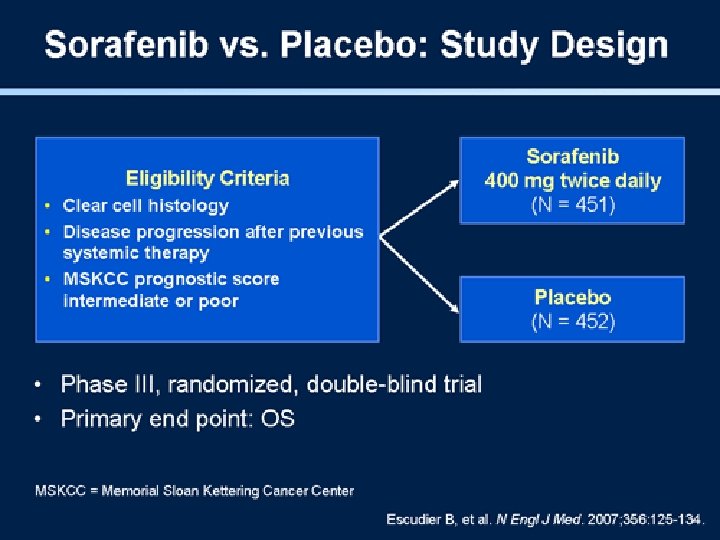
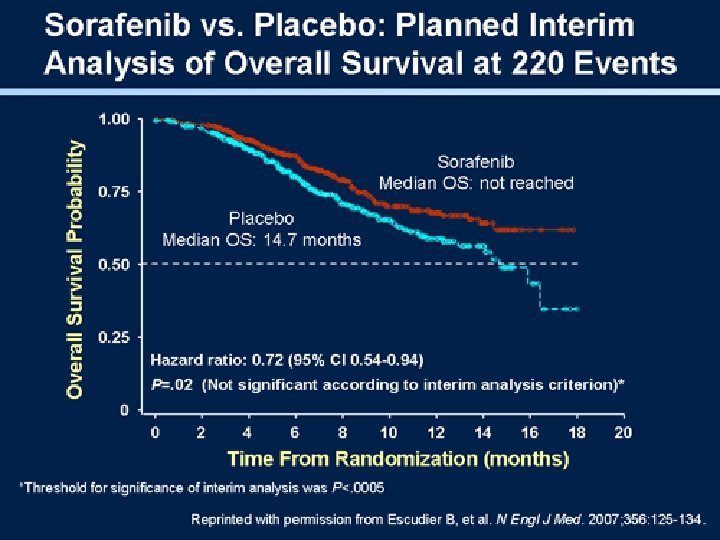
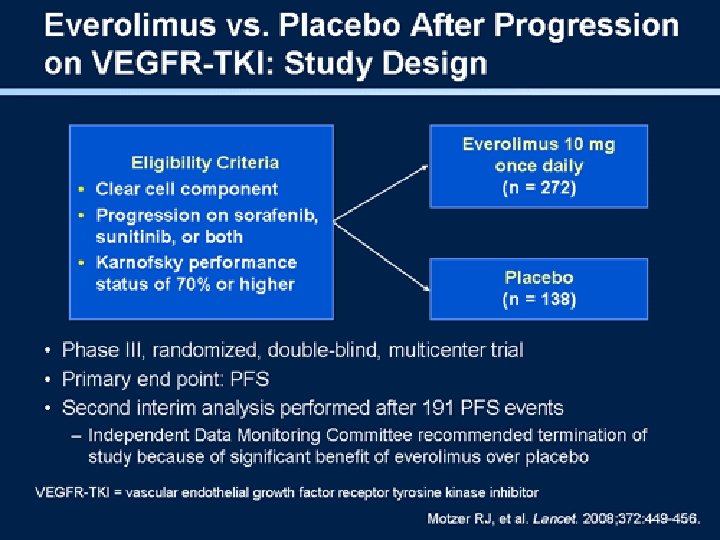
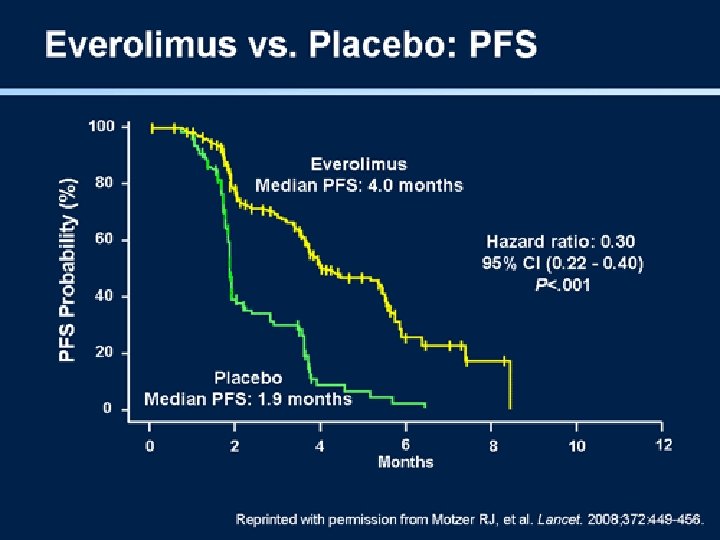
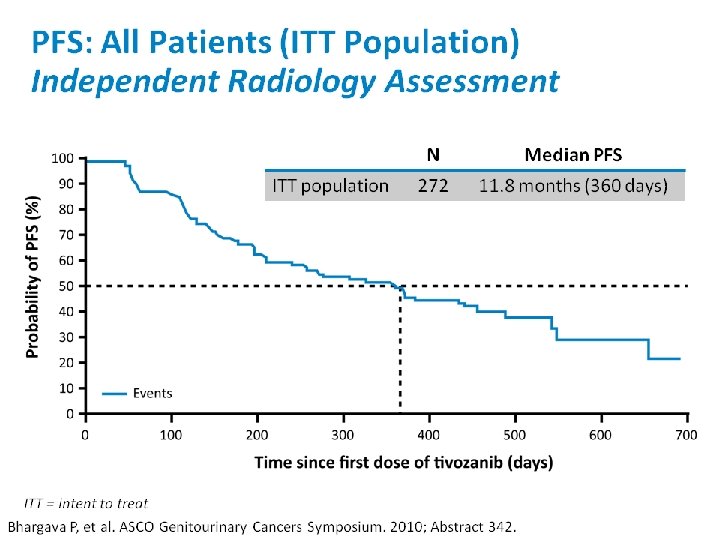
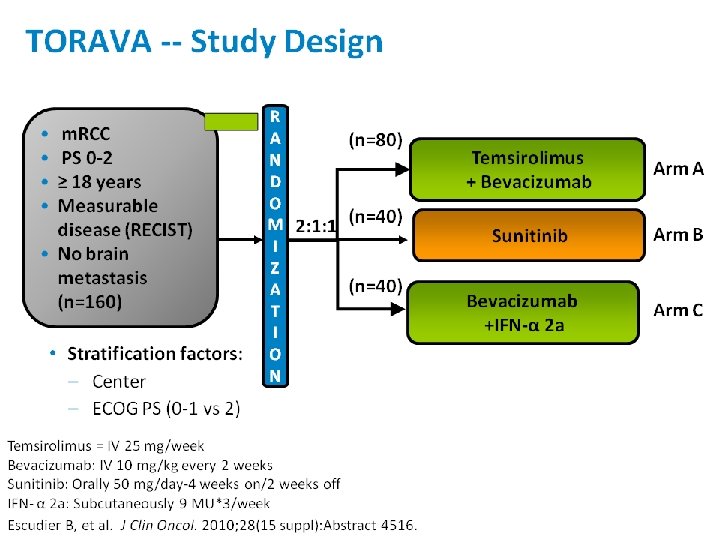
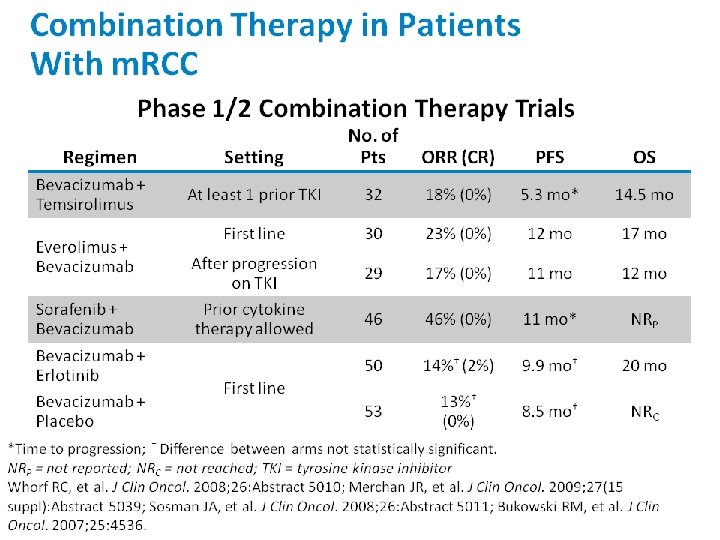
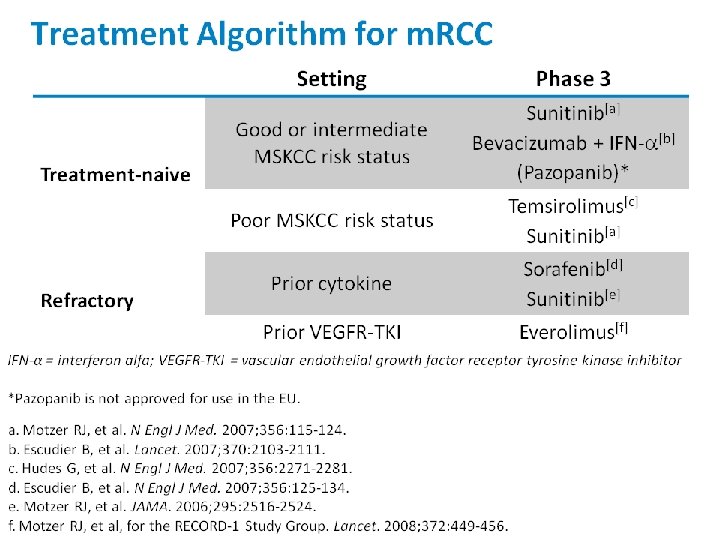
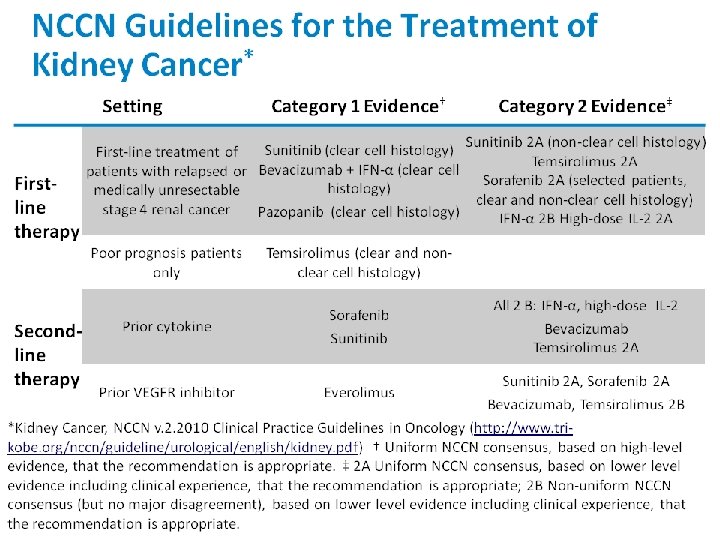
Treatment of metastatic disease

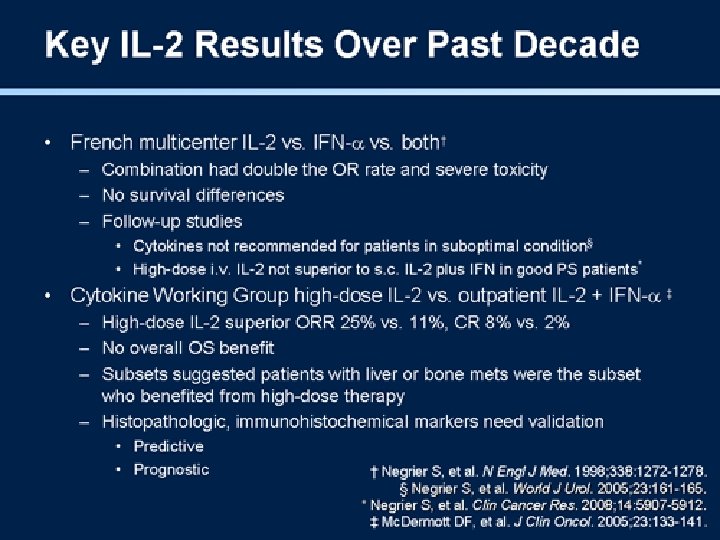
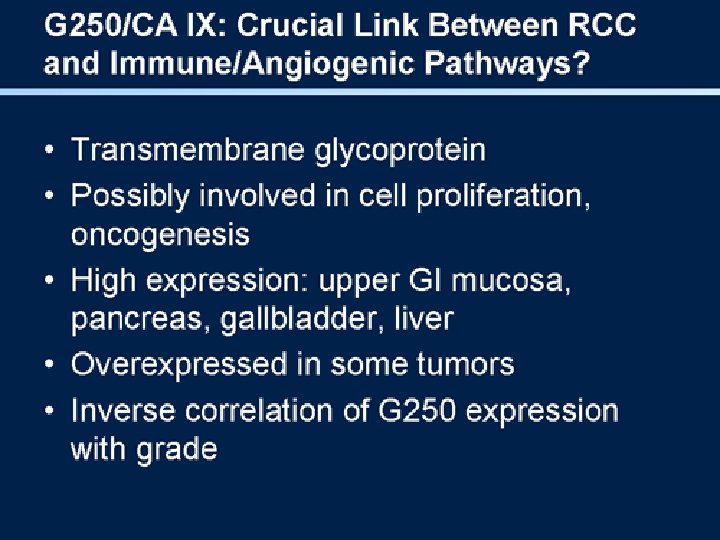
Immunotherapy • IL 2 • interferon alpha
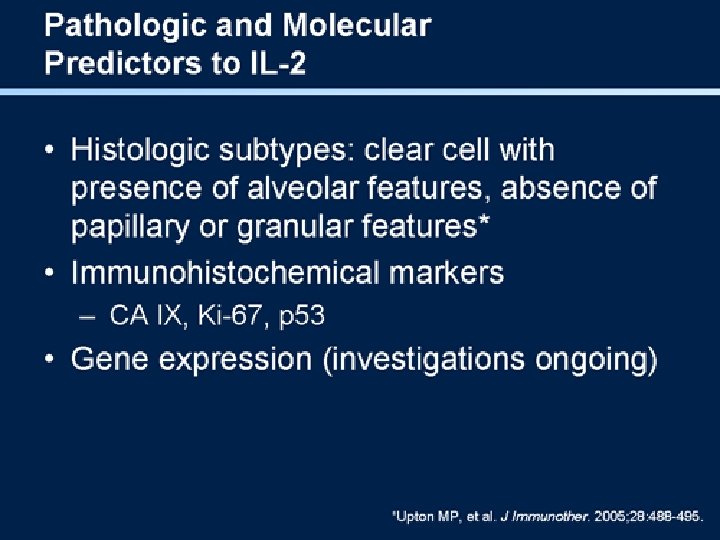

2. Alpha-methylacyl-Co. A racemase – significant increase of AMACR m. RNA levels in papillary renal cell carcinomas only – Also molecular marker for prostate cancer 3. B 7 -H 1 – expression may indicate worse survival, possibly through impaired host antitumor immunity 4. Microsatellite instabilities

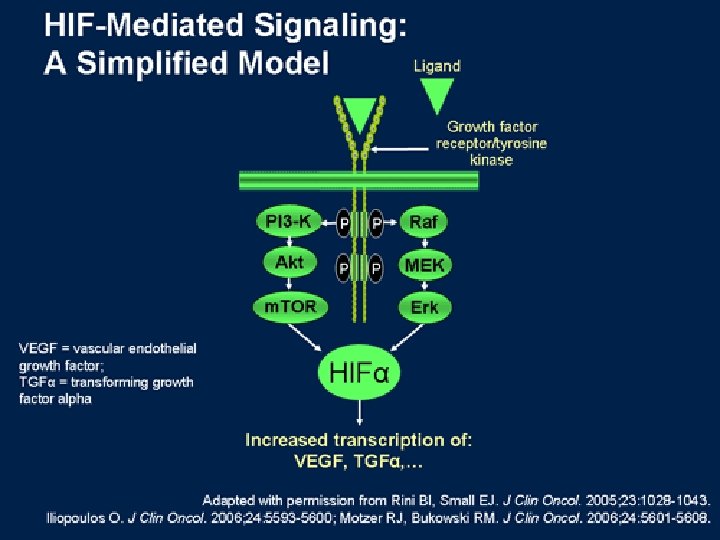
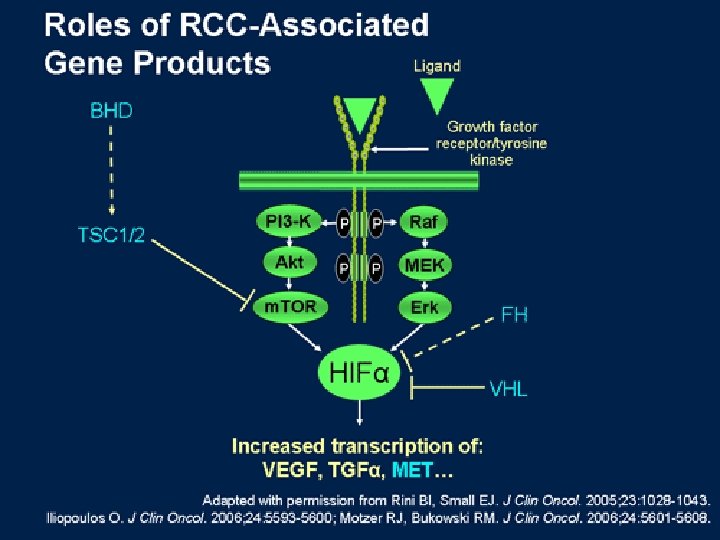
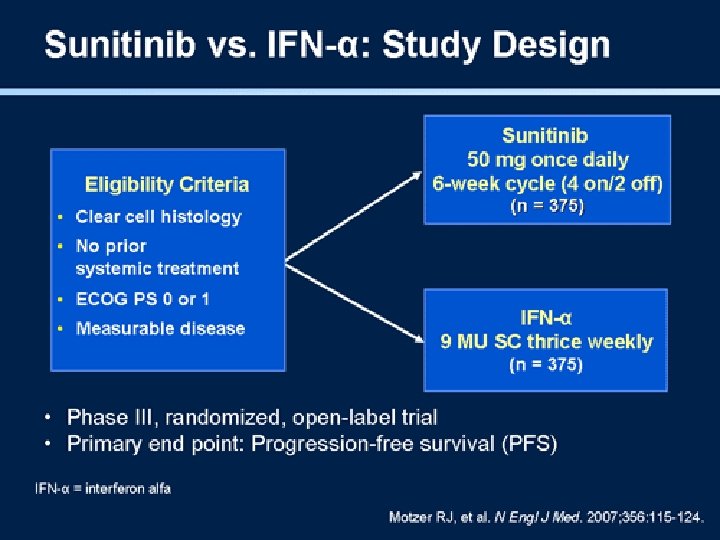
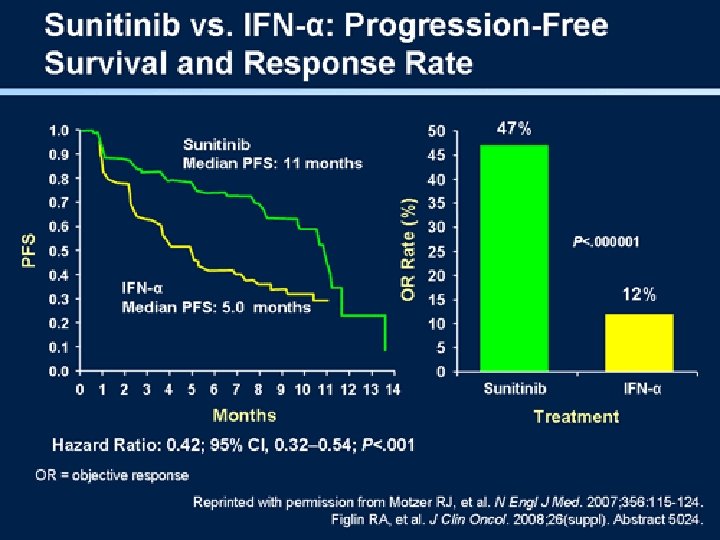
Target Therapy What is my the target?
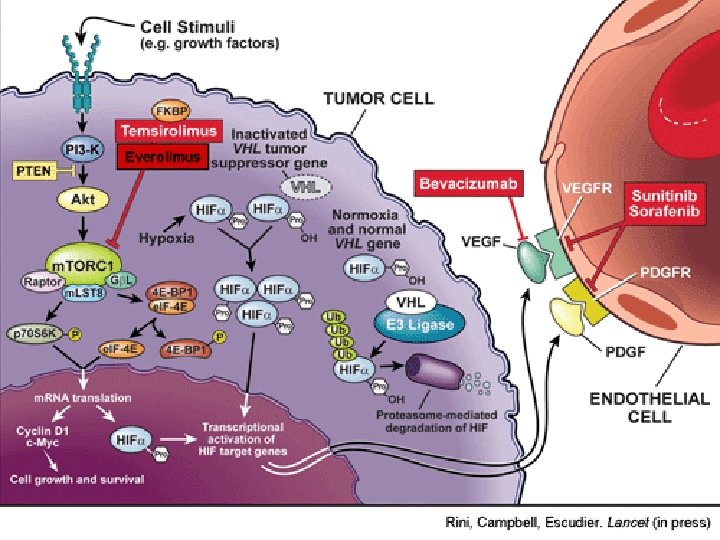


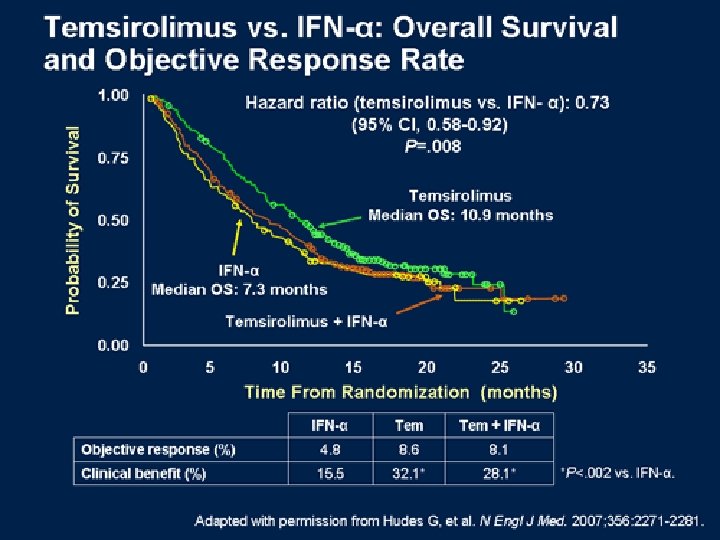
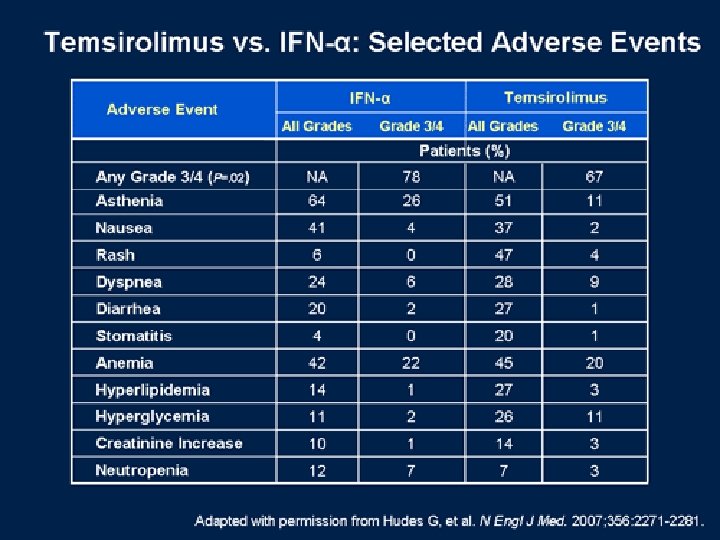
Temsirolimus

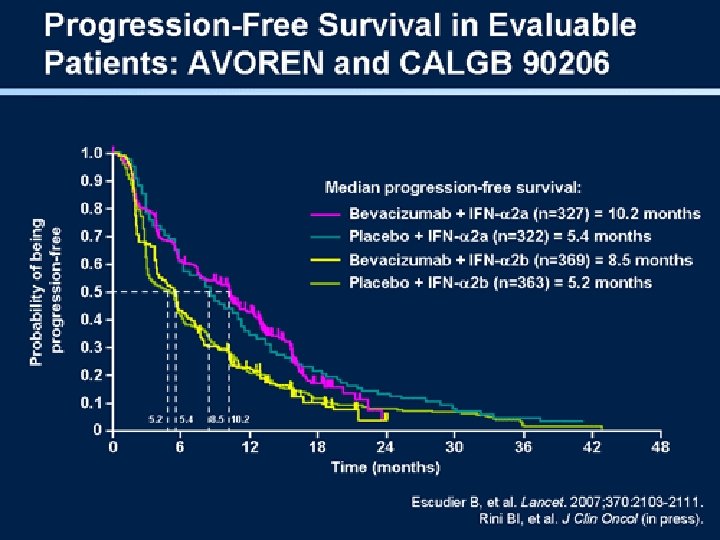
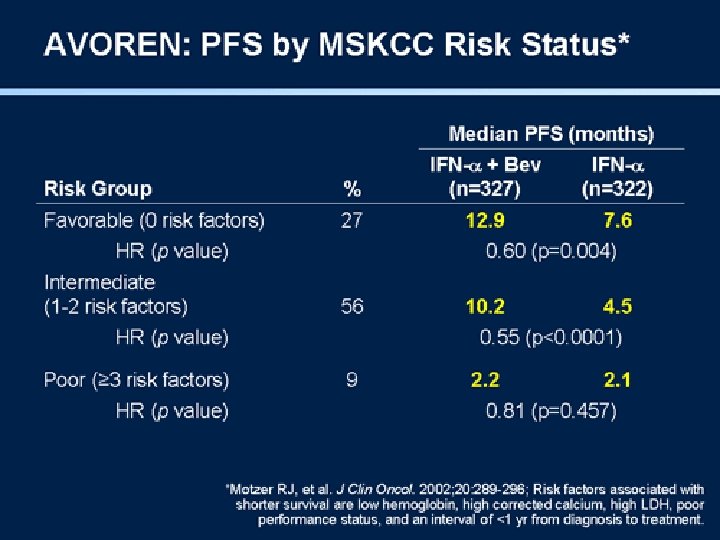
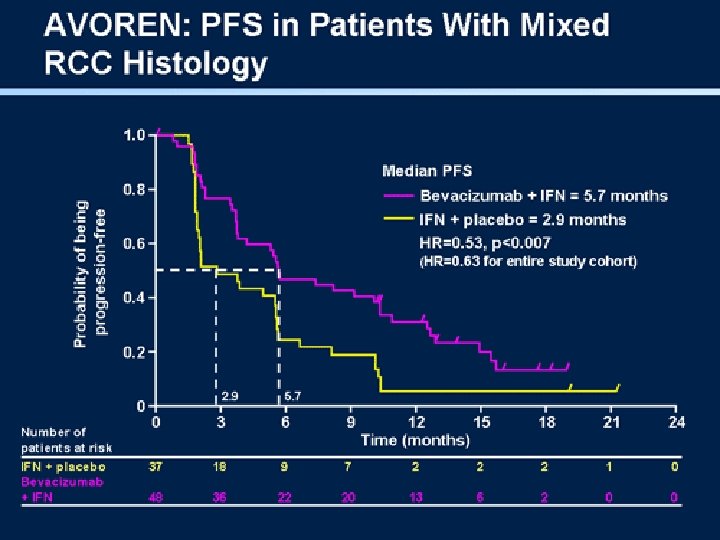
Bevaciziumab

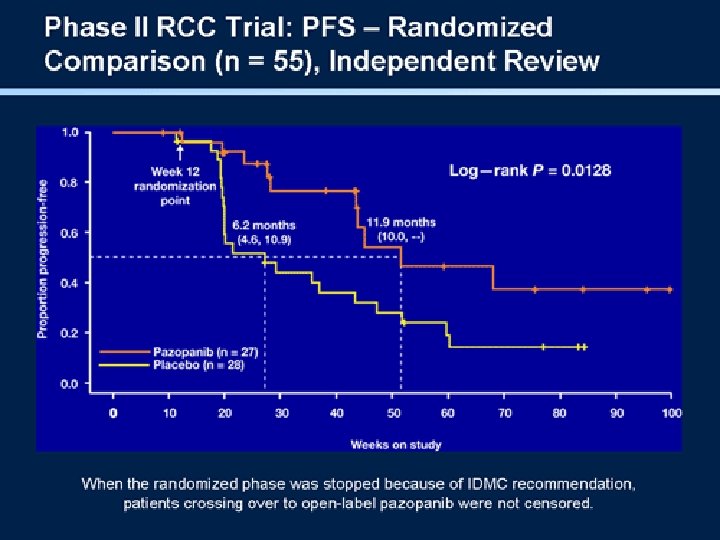
Pazopanib

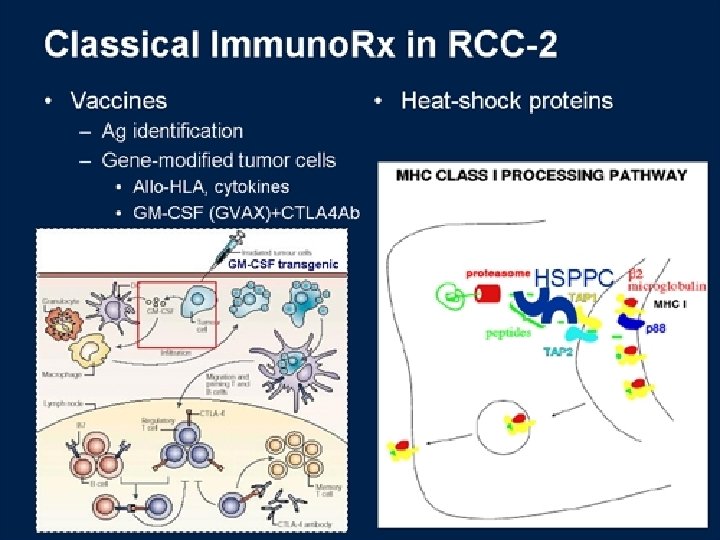
Vaccine

Reduced inteinsty myeloablative bone marrow transplant

Summary

Thank You
- Slides: 92