Removable Prosthodontics Types Acrylic Look For Thin wire

Removable Prosthodontics

Types Acrylic Look For: Thin wire clasps Non metal base on the underside Complete Pa coverage Cobalt Chrome Look For: Bulky metal clasps everywhere Can see metal through the acrylic Generally metal over the Pa Valplast Look For: Pink/Red flexible clasps Absence of metal Not always full arch, can be small sections like above Thinner than acrylic, more translucent Beware of upper and lower
 ● ● ● Anticipate future modifications Abutment teeth aren’t stable Immediate/ denture")
Acrylic (721/722) ● ● ● Anticipate future modifications Abutment teeth aren’t stable Immediate/ denture Displaceable mucosa Labile bone Lots of teeth missing, need to rely on mucosal support Xerostomia (use artifical saliva) Contraindications ● Inability to control own musculature Pros ● ● ● Cheaper Add on teeth easily Good wettability Aesthetic Quicker to make Indications ● ● ● Cobalt Chrome (727/728) Abutment teeth stable “Tight bite” as metal can be cast thinner acrylic needs 2 -3 mm of space Para. Fx (reinforce metal around teeth, acyrlic will #) ● ● Aesthetics bc no metal Immediate/transition denture ● ● ● Rampant caries Abutment teeth aren’t stable Cost (double $$ of acrylic) ● ● Poor denture hygiene Anticipate future modifications ● ● ● Stronger Good thermal conductor Doesn’t warp with heat Doesn’t stain Less bulky ● ● Aesthetic Flexible Good biocompatibility Comfortable ● 5 Cons ● ● ● Poor thermal conductor Warps with heat Bulky Porous → Picks up stains Plaque accumulation 4 5 ● ● ● 5 Valplast Expensive Not aesthetic Longer construction process Can’t add on teeth easily Tarnish and Corrosion ● ● 5 Colour stability fades Retains water Difficult to repair Hard to clean (need special products) 4

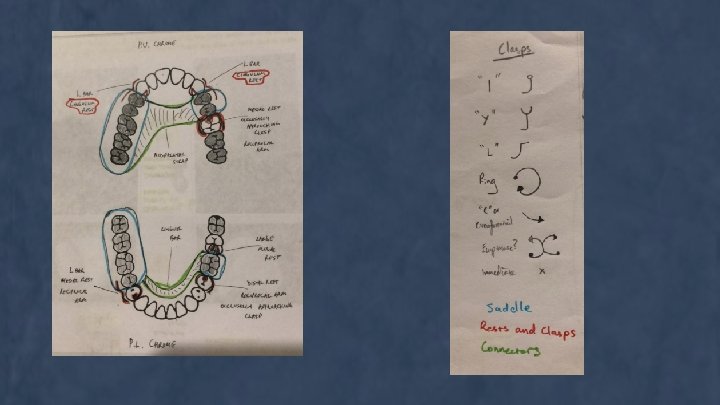
Design Principles → Sa Su. Re is Co. Si Saddle Support Retention Connectors Simplification

Saddle - Kennedy Class I-IV Do you have free end or bounded saddles? Support = Resisting dislodgement or displacement from foundation during Fx Tooth vs Mucosa vs Tooth & Mucosa - Height of dense, non-labile alveolar bone Increase contact SA between denture and mucosa Tooth - Occlusal Rests Free end: Mesial aspect of tooth Bound: Post = Mesial, Anterior = distal

Retention = Resist forces of dislodgement along path of placement Physical Forces: - Increase SA Wettability Cohesive/adhesive/surface tension/Viscosity Physiological Forces: - Musculature Mechanical Forces: - Clasps going into undercuts Connector Acrylic - Mx: Wide variety of choices More SA the better (always try full Pa) Sometimes can leave the middle Pa space open for taste buds or if pt doesn’t like but you’ll lose retention Co. Cr - SA isn’t a big issue Md: Li bar and plate

Simplification - If you don’t need it Pentagon/Triangle/Rectangle

Acrylic partial denture appointment sequence Appointment Sequence 1. Consultation: History, examination, treatment plan, consent. ● ● Primary impressions in alginate in stock trays: assess whether impression can be used as master impression, if not ask for CCA special tray – spaced two thicknesses of wax and perforated for alginate; spaced one thickness of wax for PE or PVS. Lab: pour primary impression in yellow stone: construct CCA special tray. 2. Master impression in alginate, PE or PVS. See if models go together so a bite appointment may not be required. ● Lab: Pour master impression in greenstone; survey, block out undercuts, prepare working cast, construct record base (wax or CCA) with wax rim. 3. Jaw relation (bite) record and tooth choice (mould and shade) ● Lab: mount on articulator and set up teeth. 4. Try in: assess occlusion, aesthetics, neutral zone etc: get patient approval, finalise denture design with positions of wrought wire clasps. Take remount record for retryin if necessary. Carve palatal seal if full palatal coverage. ● Chrome-cobalt partial denture appointment sequence 1. Consultation: history, examination, treatment plan, consent. ● Primary impressions in alginate in stock trays: ask for CCA special tray – spaced two thicknesses of wax and perforated for alginate: spaced one thickness of wax for PE or PVS. ● Lab: Pour impression in yellowstone: survey cast: construct CCA special tray. 2. Preferably before this appointment, plan design of partial and plan any tooth preparation e. g. occlusal rests. ● ● Get tutor to approve design: do any tooth preparation: take master impression. Lab: construct partial chrome and attach wax rim. 3. Try in chrome casting: adjust as necessary: take wax bite: select artificial teeth. ● Lab: Mount on articulator and set up teeth. 4. Try in: Assess occlusion, aesthetics, neutral zone etc: get patient approval. ● ● Take remount record for retryin if necessary. Lab: Process and finish. Lab: Place clasps as designed: process and finish. 5. Insertion: adjust as necessary: instruct patient how to insert and remove: give instructions. 6. Post insertion: generally one week later: check patient progress: adjust as necessary: make further post insertion appointment if necessary. 5. Insertion: adjust as necessary: instruct patient how to insert and remove: give instructions. 6. Post Insertion: generally one week later: check patient progress: adjust as necessary: make further post insertion appointment if necessary. 7. Recall after 6 -12 months.

Questions

Pharmacology Pharmacokinetics versus pharmacodynamics - Pharmacokinetics - how different factors of an individual patient affect the drugs effectiveness - - ADME (absorption, distribution, metabolism, excretion) Pharmacodynamic - “what the drug actually does” and how it does it Australian Medicines Handbook (AMH)
 -")
Absorption From ingested method → absorbed into the bloodstream Measured by bioavailability (F) - indicates the amount of the oral dose that reaches systemic circulation (from 0 -100%) Reasons why drugs have <100% bioavailability: 1. 2. 3. Insufficient time for absorption (in the intestine) Decomposition in gut lumen Liver first pass effect

Distribution - distribution of the drug from the blood into the body’s tissues Dependent on: 1. 2. 3. 4. Drugs lipophilicity Blood flow (rate) Capillary permeability (e. g. larger drugs may not be able to exit the capillary to target tissue) Binding plasma proteins (albumin) Measured by volume of distribution (L) - theoretical volume that would be necessary to contain the total amount of an administered drug at the same concentration observed in the blood plasma A higher Vd indicates a greater amount of distribution into the tissues - to increase the concentration of the drug in the blood, the volume of distribution must be proportionally decreased Vd facilitates in calculation of loading dose:

Elimination - irreversible loss of drug from blood via metabolism and excretion Drug metabolism/transformation: enzymatic conversion of a drug to a metabolite - Metabolites: usually have decreased pharmacological value but some may still be active, therefore need to be careful in patients with renal impairment/elderly patients A process which occurs to make a drug more water soluble so it can be excreted by the kidneys: OCCURS IN 2 PHASES Phase 1 (transformation) - Unmasking/adding a polar functional group to make the drug more water soluble Occurs via oxidation (mainly), reduction and hydrolysis Catalysed by CYP enzymes in the liver Phase 2 (conjugation) - Occurs if metabolites from stage 1 are not hydrophilic enough yet to be excreted by the liver, then in phase 2, an additional polar group may be added Facilitated by transferases

Elimination cont. Total clearance = renal clearance + hepatic clearance Clearance is independent of volume of distribution half life - it depends purely on liver and kidney function Clearance = a pharmacological measure of elimination Clearance helps to determine appropriate maintenance dose rate to achieve target plasma concentration on chronic dosing Half life (t 1/2) = time for blood concentration to reach half after a single dose - Determines time required to achieve steady state + time to eliminate the drug after chronic dosing has stopped Every drug reaches a steady-state after 5 half-lifes

Variability in Drug Response; Drug Interactions Drug to drug interactions: 1. 1. St John’s Wort CYP inducer Increases production of CYP, therefore increasing metabolism of Drug B, thereby reducing its therapeutic effect E. g. cyclosporin Grapefruit CYP inhibitor Decreases metabolism of Drug B = risk of overdose/toxicity E. g. statins and oral contraceptives ‘Triple Whammy’ NSAIDS, ACEI, and diuretics NSADS decrease afferent arteriole rate via vasoconstriction ACEI causes vasodilation of the efferent arteriole Diuretics causes decrease in plasma concentration + GFR Results in overall dramatic decrease in GFR → acute renal failure

Pharmacokinetic interactions 1. Enzyme induction: Drug A induces metabolism of drug B - Anticonvulsants (phenytoin), rifampicin, cigarette smoke, St John’s Wort) 1. Enzyme inhibition: competitive inhibition - Erythromycin + fluconazole, metronidazole, sulphonamides 1. Drugs susceptible to metabolic interactions - Those cleared by metabolism, narrow TI - Anticoagulants, antiepileptics, analgesics, antidepressants

Pharmacodynamic interactions 1. 1. 1. 1. Drug A and B: working on the same target, same effect Amitriptyline (antidepressant) + ipratropium (antihistamine) → used together results in very dry mouth (both work on anticholinergic receptors) Drug A+ B: working on different targets but have the same effect CNS depressants (codeine) + alcohol → increases sedation Warfarin + aspirin → bleeding Herbal medications with drugs St John’s Wort → decreases drug B E. g. cyclosporin + SJW → transplant tissue Food-drug interactions Grapefruit: CYP inhibits = increased blood concentration of drug B (statins) → toxicity (muscle damage) Milk: decreases absorption of AB Oral absorption interactions Antacids decrease GIT absorption of AB Iron tablets decrease absorption of drugs (ciprofloxacin - AB)

Clinically Important Enzyme Inhibitors - Erythromycin, clarithromycin Fluconazole Metronidazole Quinolones Sulphonamides Others: - SSRI antidepressants Grapefruit juice
:")
Endodontic Treatment Aim: TREATMENT/PREVENTION of apical periodontitis Provisional → Definitive Diagnosis (Pulpal + Periapical): ● ● Pt questioning: Symptoms + hx (COLDSPA) ○ Can you localise the pain? ○ Type of pain? I. e. sharp/dull ○ Duration of pain i. e. seconds, minutes, hours “lingers” ○ Exacerbating factors i. e. hot/cold, eating ○ Spontaneity? ○ Does it keep you awake at night? Diagnostic testing ○ Sensibility testing i. e. Cold test ○ Percussion ○ Palpation ○ Probing ○ PA Pulpal diagnosis: ● Reversible pulpitis ● Irreversible pulpitis ● Necrotic pulp Periapical diagnosis: ● Symptomatic apical periodontitis ● Asymptomatic apical periodontitis ● Symptomatic apical abscess ● Asymptomatic apical abscess

Endodontic Treatment: Considerations & Prognosis ● ● ● Strategic value of tooth Periodontal factors ○ Local/generalised perio ○ Endo/perio lesions ○ VRFs ○ Perforation Patient factors ○ Motivation to retain teeth ■ Cost ○ MHx ■ Exo contraindicated: bisphonates, radiotherapy, immunocompromised ■ Possible RCT concerns: ● Latex allergy ● Medication allergies i. e. ABs ● Allergy to sodium hypochlorite ○ ● Age ■ Old: long appts, calcification ○ Compliance ■ Multiple appts ■ Ability to open ■ Gag reflex ■ Anxiety Restorability of tooth AAE Endodontic Case Difficulty Assessment Form!!!

Endodontic Treatment Informed consent: ● Options ○ ○ ○ Do nothing Exo - gap, partial denture, bridge, implant Endo tx ● What RCT entails ● Cost ● Risks ○ ○ ○ Tenderness Files can break Failure

Endodontic Treatment ● ● LA RD ○ Bacteria ○ Sodium hypochlorite ○ Wet/slippery
 Outline Form: project internal anatomy of tooth to")
Endodontics: Access (both physically & visually) Outline Form: project internal anatomy of tooth to outside Relationships of pulp chamber to crown: ● Law of the CEJ ○ Most consistent, repeatable ● Dependent on landmark for locating the ○ Pulp chamber size/shape position of the pulp chamber ○ Number and position of canals ● Law of centrality ● High speed ○ Pulp chamber is (at level of ○ Tapered diamond bur CEJ) going to be equidistant ○ 169 L tungsten carbide bur from every wall ○ Beaver bur ● Law of concentricity ○ Shape of tooth at level of CEJ is going to perfectly Convenience Form: to allow accurate preparation and filling of root mimic what the shape of the canals pulp chamber ● ● Slow speed ○ ¾ shank 3 round tungsten carbide Removal of carious dentine Unobstructed access to the canal orifices Direct access to the apical foramen i. e. Straight line access

Endodontics: Instrumentation Aims: ● ● Remove vital + necrotic tissue from RCS Create enough space for irrigation + medication Preserve integrity/location of apical RC anatomy Establish convenience form to facilitate obturation Technique: Hand files ● ● Negotiate canal to apex (passive ‘watch-winding’ technique) ○ #10 or #15 to EWL (Pre-op radiograph/Apex locator) ○ Take PA → CWL Crown down: prep of the coronal ⅓ or ½ w/ Gates Glidden ⅔ ○ Brushing motion, away from furcation in premolars/molars Apical preparation ○ Enlarge to MAF (usually 2 -3 sizes larger than first file to bind apically) Step back ○ One size up 1 mm shorter

Endodontics: Irrigation Aim: Remove microbes & Dissolve & flush organic & inorganic debris Sodium hypochlorite (Na. OCl) ● Potent antimicrobial agent ● Dissolves vital and necrotic pulp tissue ● Affects ORGANIC part of smear layer EDTA ● Chelating agent - INORGANIC component of dentine (exposes tubules → facilitates preparation medicament effectiveness, cement adhesion) Regime: ● Na. OCl during instrumentation phase (during access, canal exploration, after each file - copiously w/ suction) ● EDTA after instrumentation ● Final flush w/ Na. OCl

Endodontics: Medicaments ● Bacteria cannot be predictably eliminated by combining mechanical instrumentation and irrigation with Na. OCl ● Medicaments eliminate more bacteria Selecting a medicament: ● 90% of situations – Ca(OH)2 ● Re-treatments + dressing changes – CHX useful adjunct (used in conjuction with CHX irrigant) ● Avulsion + Luxation injuries – Odontopaste initially, then Ca(OH)2 ● ROP pulpotomy – Ledermix or Odontopaste, followed by completed preparation + Ca(OH)2

Endodontics: Medicaments Calcium hydroxide: ● Antimicrobial activity: produce a highly alkaline environment incompatible w/ microbial survival ● Promotes PA healing (p. H buffers acidic inflammation in PA tissues) Delivery systems: ● Spiral fillers in a slow speed (4 mm short of WL – rubber stopper) ● Hand files (useful in unprepared canals or canals with sharp curves – spiral fillers have risk of fracture if wound in tight canals, pre-bent hand file for sharp curves) ● Injection systems (greater risk of overfill over apex of tooth)

Endodontic Treatment: Obturation When? ● Asymptomatic ● No clinical signs of pathosis (percussion, palpation, draining sinus, radiographic evidence of healing (? )) ● Negative culture Process: (irrigate - Na. OCl, EDTAC, dry canal w/ paper points) ● ● ● Fit Master GP Point (same size as MAF) to length → take PA Introduce sealant to canal (AH plus - resin based sealer) w/ lentulo spiral Place Master GP Point Lateral condensation (displace GP/sealant laterally to make room for acc pts) Place accessory points (same size as lateral spreader) Take PA before burning off GP

Endodontic Treatment Temporisation: ● “Double - Seal” - Cavit & GIC Permanent Restoration: ● ASAP ● Bonded materials are preferred ● Cuspal coverage should be provided for posterior teeth Take PA

Oral Pathology

Oral Pathology Basic levels of histology

Oral Pathology Describing Pathology and DDx - Yings 5 S’s and 5 C’s Concise Specific - - Polypoid/pedunculated, round, keratotic lesion on R Bu Mucosa approximately 5 -7 mm across. Lesion is well defined, white-pink in colour, exophytic, seemingly fibrotic, chronology unknown DDx - List from MOST COMMON to LEAST COMMON

Oral Pathology Radiography for Hard Tissue Disorders - What radiograph is it? Radiographic descriptors - - DDx Similar to Yings 5 S’s and 5 C’s Colour - RL or RO or Mixed - Uniformly RL = Likely Cystic - Mixed RL/RO = more solid = more neoplastic = fibro-osseous lesion (maybe)

Oral Pathology Diagnostics and Tests - TNM staging - - Histopathology slides - - What to expect if a lesion is ‘Stage 2’ Prognosis? They usually have mercy - Oral Lichen Planus? - Pemphigus vs. Pemphigoid? Histopathology report? - What to include in the report What the diagnosis is based on histopath report - Usually related to neoplasia
 - Gum lumps and bumps?")
Oral Pathology Misc things to think about ; ) - Gum lumps and bumps? - - Note not all of them are soft tissue, can be of HT origins What can cause Desquamative Gingivitis? DDx for Parotid gland swelling? How to tell if a lesion is Benign or Malignant?

OHP Questions?

Questions?
- Slides: 39