Remission In Rheumatoid Arthritis RA How Will The
: How Will The New Criteria Change Our Approach To")







")
 • TCZ 8 mg/kg (n=412) vs PBO (n=207), 1°")
")




 • Established in 2005 • All consecutive")


")
 – RAPID 3 • MDHAQ")




 • Prospective, consecutive patient data since")



![ACR Core Dataset by Remission Age (Years) Duration (Years) Function [0 -10] Pain [0](https://slidetodoc.com/presentation_image/31ba64bf0cd313f24755448e255c95ad/image-31.jpg "ACR Core Dataset by Remission Age (Years) Duration (Years) Function [0 -10] Pain [0")

- Slides: 32
Remission In Rheumatoid Arthritis (RA): How Will The New Criteria Change Our Approach To RA Treatment? Yusuf Yazıcı, MD NYU Hospital for Joint Diseases, New York
Disclosures • • • Abbott BMS Celgene Centocor Genentech Janssen Merck Pfizer Roche Takeda UCB
Background • • Early, aggressive treatment Measurement tools Treat to target Routine monitoring
Why Do We Need to Measure? • 102 patients with RA on conventional treatment, judged by their rheumatologist to be in remission % Meeting remission criteria 54 DAS 28 remission criteria Mean score 2. 53 % Remission, <2. 6 56 % Low disease activity, 2. 6– 3. 2 20 % Moderate disease activity, 3. 2– 5. 1 23 % High disease activity, >5. 1 1 Association between baseline findings and radiographic progression over 12 months Baseline variable No radiographic progression, n=73 Radiographic progression, n=17 Odds ratio (95% CI) P RF + (n) 28 11 2. 95 (0. 98, 8. 86) 0. 054 ESR, median, mm/h 10 13 1. 01 (0. 96. 1. 06) 0. 667 CRP, median, mg/L 5 0 1. 01 (0. 93, 1. 10) 0. 765 Met ACR remission (n) 41 5 0. 33 (0. 10, 1. 02) 0. 054 Met DAS 28 remission (n) 44 6 0. 36 (0. 12, 1. 08) 0. 068 2. 48 2. 89 1. 54 (0. 89, 2. 65) 0. 122 Total US PD score, median 1 1 1. 36 (1. 02, 1. 81) 0. 038 Dominant hand US PD score, median 0 0 1. 64 (1. 03, 2. 61) 0. 036 DAS 28 score, mean Brown AK et al. Arthritis Rheum. 2008; 58: 2958 -2967.
ACR Core Data Set 1. Swollen joint count 2. Tender joint count 3. Physician Global Assessment 4. ESR or CRP 5. Physical Function (HAQ, MDHAQ) 6. Pain 7. Patient Global Assessment 8. Radiographs
Clinical Measurement Tools Outcome Measures in RA ACR 20 DAS 28 SDAI CDAI GAS Patient function + + Patient pain + + Patient global + MD global + # Tender joints + # Swollen joints ESR or CRP + ERAM RADAI RADARA + + + + + + + RAPID 3 + + SDAI=Simplified Disease Activity Index; CDAI=Clinical Disease Activity Index; GAS=Global Arthritis Score, ERAM=Easy Rheumatoid Arthritis Measure; RADAI=Rheumatoid Arthritis Disease Activity Index; RADARA=Real-Time Assessment of Disease Activity in Rheumatoid Arthritis; RAPID=Routine Assessment of Patient Index Data. Cush JJ. Presented at: 2005 ACR Annual Scientific Meeting. November 12 -17, 2005. San Diego, CA. Abstract 1854; Sesin CA et al. Semin Arthritis Rheum. 2005; 35: 185 -196; Makinen H et al. Clin Exp Rheumatol. 2006; 24: 22 -28; Yazici Y. Bull NYU Hosp Jt Dis. 2007; 65(suppl 1): 25 -28; Call S et al. Presented at : 2007 ACR Annual Scientific Meeting. Boston, MA. Abstract 425. Fransen J et al; Rheumatol. 2000; 39: 321 -327.
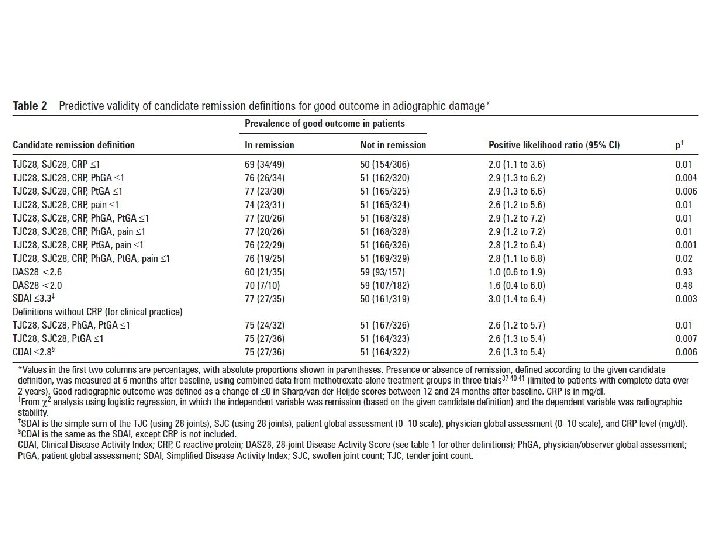
New ACR/EULAR RA remission criteria • Developed by committee using data from clinical trials • Assessed ability of candidate measures to predict: damage (change 0 in vd. H/S score) and function (change in HAQ 0; HAQ 0. 5) over 2 ys • Best results obtained by 2 proposed definitions: – TJC and SJC and CRP and Pt Global all 1 OR – SDAI 3. 3 • [SDAI = TJC (28) + SJC (28) + Phys global (0– 10 cm VAS) + Pt global (0– 10 cm VAS) + CRP (mg/d. L) Felson DT, et al. Ann Rheum Dis 2011
New remission criteria • New remission criteria for RA – “more stringent than DAS 28, CDAI or RAPID 3 remission” • Little information regarding – Feasibility of use in routine clinical care – If it is better than RAPID 3 remission • a very simple, patient friendly tool and easily implemented in everyday patient care.
% Change from Baseline Improvement Patient-Reported Outcomes: Placebo Response at 6 Months Pain (VAS) SJC TJC HAQ DI ESR CRP Phys Pt Global Physician-derived Strand V et al. Rheumatol. 2004; 43: 640 -647. HAQ (mean) Patient-derived Laboratory
TCZ in DMARD-IR RA (ROSE) • TCZ 8 mg/kg (n=412) vs PBO (n=207), 1° EP: ACR 50 Week 24 • 62 patients, subset analysis for 1 -week results • DAS 28, CRP, pain, PGA improved at 1 week; not joints or MDGA TCZ 8 mg/kg + DMARDs PBO + DMARDs P=0. 007 DAS 28 Pt Pain P=0. 007 P=0. 01 PGA P=0. 005 P=0. 001 MDGA MDHAQ-PF TJC P=0. 005 SJC VAS MD Global (P=0. 0502) NS Pt Pain. NS NS VAS Patient, not physician, measures show improvement at 1 week Yazici Y, et al. ACR 2010, Atlanta, #1808 Copyright 2010, TREG Consultants LLC
CATCH: Remission prevalence in early RA new criteria vs other criteria RF/ CCP (+) Bio % CRP DAS 28<2. 8 56/62 7 0. 33 DAS 28<2. 0 55/61 7 0. 26 SDAI<3. 3 59/64 9 0. 32 CDAI<2. 8 58/64 10 0. 38 ACR/ EULAR 54/65 8 0. 27 • ACR-EULAR criteria agrees w/ SDAI (k=0. 77) & CDAI (k=0. 75) • Fair agreement w/ DAS 28<2. 6 (k=0. 40) & DAS 28<2. 0 (k=0. 40) All remission is not the same 1, 2 1. Kuriya B, et al. EULAR 2011, London, #SAT 0405; 2. Bernard M, et al. Ibid, #OP 0027 Copyright 2011, TREG Consultants LLC
Utility of 2011 ACR/EULAR 2011 remission criteria • US VA and community practice cohort study 1 – 1341 VA patients / 9700 visits (91% men) – 1168 community practice patients / 6362 visits (28% men) – Remission: • Cross sectional: 8. 9% / 8. 3% • Cumulative: 24. 4% / 19. 0% over 2. 2 y • 1. 9– 4. 6% patients met remission at ≥ 2 visits • Among all patients, <3% had remission lasting 2 y • DREAM: ↑ Pt. G most common reason for failure to meet remission 2 • Non-inclusion of feet may overestimate remission 3 • Patients in ACR/EULAR remission have function capacity = to normal 4 Remission is uncommon in the clinic, especially long term 1. Michaud K, et al. EULAR 2011, London, #FRI 0333; 2. Vermeer M, et al. Ibid, #OP 0311; 3. Bakker MF, et al. Ibid, #SAT 0376; 4. Listing J, et al. Ibid, #THU 0351 Copyright 2011, TREG Consultants LLC
HAQ improvement and time in remission in RA patients using various criteria • BRASS Registry: pts with >2 y F/U; more time in remission better HAQ with respect to F/U visits 0 1 2 DAS 28 <2. 6 DAS 28 <2. 3 SDAI CDAI ACR/EULAR – 0. 05 md. HAQ 3 – 0. 15 4 0 – 0. 25 1 2 4 4 4– 11 11– 22 >22 No. of yearly visits in remission Duration of time in remission regardless of measure correlates with HAQ improvement; patients with early RA do better Prince FHM, et al. ACR 2011, Chicago, #333 3 dd – 0. 6 No. of yearly visits in remission 0 – 0. 2 – 0. 4 – 0. 2 md. HAQ according to dd by DAS 28 -CRP <2. 6 rem 0. 2 md. HAQ 0 Copyright 2011, TREG Consultants LLC
Impact of different remission criteria on functional ability • 5788 RA pts from NOR-DMARD registry: starting DMARDs (n=3875) or biologics (n=1913) DAS 28 CDAI RAPID 3 ACR/EULAR % remission, 3 mo 19. 1 8. 1 17. 0 9. 3 % no Δ m. HAQ, 3– 12 mo 65. 7 64. 9 65. 2 63. 6 % remission, 6 mo 24. 7 11. 3 19. 8 12. 3 % no Δ m. HAQ, 3– 12 mo 69. 6 73. 6 69. 8 72. 6 Different numbers of patients achieve remission, but no difference in predicting physical function Uhlig T, et al. ACR 2011, Chicago, #1229 Copyright 2011, TREG Consultants LLC
www. TREGdocs. com BRASS: Radiological progression in remission by new ACR/EULAR criteria vs other criteria
NYU Arthritis Registry Monitoring Database (NYU ARMD) • Established in 2005 • All consecutive patients • ~800 RA patients, – ~6500 all dx patients • MDHAQ completed at each and every visit by all patients as part of routine care and part of the medical record – “if there is a reason to visit the doctor, there is a reason to complete a questionnaire” Ted Pincus, MD
MDHAQ page 1
MDHAQ page 2
RAPID 3 (Routine Assessment of Patient Index Data 3)
RAPID 3 (Routine Assessment of Patient Index Data 3) – RAPID 3 • MDHAQ functional score(0 -10) • Pain VAS (0 -10) • Patient Global Assessment VAS (0 -10) – RAPID 4 and RAPID 5 • RADAI - Patient Reported Joint Count (0 -10) • Physician Global Assessment (0 -10)
DAS 28 and RAPID 3 RA Categories DAS 28 Categories <2. 6 -3. 19 3. 2 -5. 1 >5. 1 = = Remission Low DAS Moderate DAS High DAS RAPID 3 Categories < 3. 01 -6 6. 01 -12. 0 >12. 0 = = Near Remission Low Severity Moderate Severity High Severity
RAPID 3 vs DAS 28 in 285 RA Patients Spearman correlation rho = 0. 657 24 Pincus T, et al. J Rheumatol. 2008; 35: 2136 -2147.
RAPID 3 & DAS 28 Categories are Correlated Significantly in 285 Patients at 3 Sites RAPID 3 Scores > 6. 1 = High or moderate severity < 6. 0 = Low severity or remission Total > 3. 2 = Moderate or high activity 114 (81%) 26 (19%) 140 (49%) < 2. 6 = Low activity or remission 47 (32%) 98 (68%) 145 (51%) Total 161 (56%) 124 (44%) 285 DAS 28 25 Pincus T, et al. J Rheumatol. 2010
Time Needed to Score Various RA Measures 26 Yazici Y, et al. J Rheumatol. 2008; 35: 603.
Methods • NYU Arthritis Registry Monitoring Database (ARMD) • Prospective, consecutive patient data since 2005 – all patients seen in routine care • Each patient with any diagnosis completes a 2 -sided, 1 -page MDHAQ at every visit as part of routine clinical care • MDHAQ includes scales for – – – • • physical function pain patient global estimate fatigue self-report RADAI painful joint count Last visits of RA patients seen between July 2005 and April 2011 were studied. Differences in self-report MDHAQ scores, RAPID 3 and the new ACR remission criteria were analyzed
NYU ARMD Registry
Results • 704 RA patients (mean age 53. 9, disease duration 5. 5 years, 80% female) • 16% (116) were in remission as defined by RAPID 3 – 9% low, 27% moderate, and 48% were high disease activity • 17% (118) were in remission by the new ACR/EULAR criteria • Percent agreement between remission by RAPID 3 and new ACR criteria was 96% – with a very strong agreement beyond chance (kappa = 0. 86, p < 0. 001).
RAPID 3 components
ACR Core Dataset by Remission Age (Years) Duration (Years) Function [0 -10] Pain [0 -10] Global [0 -10] MD Global [010] Swollen [0 -28] Remission Criteria ACR/EULA RAPID 3 R 52. 7 (15. 6) 56. 1 (8. 1) 4. 8 (6. 2) 0. 3 (0. 5) 0. 6 (0. 6) 0. 4 (0. 6) 3. 9 (2. 6) 0. 5 (0. 6) 0. 6 (0. 6) 0. 3 (0. 4) 1. 0 (1. 1) 0. 1 (0. 4) 0. 6 (0. 6) 0. 2 (0. 4)
Conclusion • RAPID 3 definition of remission performs similarly to the new ACR remission criteria and can likely be used in routine care with similar benefits as part of treat to target strategy • The ease of use of RAPID 3 compared to the new criteria may make it a good option for busy clinics and clinicians • More important to use an outcome measure and target remission/low disease activity accordingly