Remission in Established RA Patients Definition of Remission

Remission in Established RA Patients

Definition of Remission Clinical Remission n ACR/DAS criteria, or normal acute phase response, no clinical synovitis Imaging Remission n No radiographic damage progression n No significant synovitis on sensitive imaging True Remission n A state of low disease activity with no progression of structural damage

New Therapeutic Possibilities for RA – Remission is a Realistic Goal Tools n Optimized MTX n Combination therapy n Anti-TNF therapy Processes n Early treatment – Avoid treatment delay – Take advantage of “window of opportunity” n Patient monitoring – DAS

Clinical Remission by DAS 28 Score Disease Activity Severe 5. 1 Moderate 3. 2 2. 6 Low Remission DAS 28 <2. 6 Based on VAS of 100 mm Prevoo MLL et al. Arthritis Rheum 1995; 38: 44 -8. van Gestel AM et al. J Rheumatol 1999; 26: 705 -11.

Remission in RA n. Importance of Structural Damage n. Determinants of Structural Damage n Interrelationship synovitis and damage n. Remission Clinical and Imaging n Impact of DMARDs n Effect of TNF antagonists

Why Is Structural Damage Important? n Cummulative measure, reflects disease control n Surrogate marker for long-term outcome (physical function, employment) n In cohorts ~ stable disease activity – Very slow increase in HAQ score – Constant progression in structural damage

ACR Goals of Therapy in RA n. Symptom relief n. Improvement in physical function n Reduce physical disability n. Slowing/arresting progression of structural damage Guidelines for the Management of RA. Arthritis Rheum. 1996; 39: 713 -22.

Schematic Representation of the Course of RA Over 30 Years Inflammation Disability Radiographic Scores Kirwan J. J Rheumatol. 1999; 26: 720 -5.

Relationship Between X-ray Progression and Physical Function - TEMPO Trial X-ray progression and HAQ scores were determined at baseline, Year 1 and Year 2 After adjustment for covariates, Sharp-score was a statistically significant determinant of HAQ-score (p<0. 0001) Progression of radiographic damage over a relatively short period of time leads to deterioration of physical function Negative Zero Mild Severe Progression van der Heijde D, et al. Abstract 1456, ACR 2005.

Cumulative Probability Plot of Radiographic Progression Unchanged Lower Score Moderate Progression

Cumulative Probability Plot of Radiographic Outcome Rapid Progressors Progression Unchanged Lower Score Moderate Progressors

What Factors Will Predict Persitemt and Erosive RA? Visser et al, Arth Rheum, Feb 2002

Stepwise Logistic Regression Analysis of Predictive Factors of Radiographic Progression • Conclusion: early destruction, high ESR, Ig. M RF positivity and DR type predict destruction during 3 years of disease Combe B, et al: Arthritis Rheum. 2001; 44: 1736 -1743.

Treatment Goals for RA Today TREAT EARLY n Any delay impacts on outcomes TREAT OPTIMALLY n Combination of traditional DMARDS TARGET CLINICAL REMISSION n Targeted outcomes / Tight control EARLY USE OF BIOLOGICS

Very Early DMARD Intervention Improves Outcomes Median Sharp Score Delayed treatment (median treatment lag time, 123 days; n=109) Early treatment (median treatment lag time, 15 days; n=97) *P<0. 05 vs delayed-treatment group. Lard LR et al. Am J Med. 2001; 111: 446 -451. *

Mean DAS score TICORA Study of Intensive vs Routine Treatment: DAS Scores 6 Routine 5 Intensive 4 *P < 0. 001 3 * 2 * * 1 * * * 15 18 0 0 3 6 9 12 Months Grigor C, et al. Lancet. 2004; 364: 263 -269

TICORA Aim for a Target –TICORA Trial Clinical Results at 18 Months Routine Care (n=53) Intensive Care (n=50) P-value Mean Fall in DAS -1. 9 -3. 5 p<0. 0001 EULAR Good Response (DAS ≤ 2. 4 and fall of 1. 2 from baseline) 44% 82% p<0. 0001 EULAR Remission 16% 65% p<0. 0001 ACR 50 40% 84% p<0. 0001 ACR 70 18% 71% p<0. 0001 Change in CRP (mg/d. L) -14 -30 p=0. 09 -0. 47 -0. 97 p=0. 0025 4. 0 9. 3 p=0. 021 Change in HAQ SF 12 Physical Summary Score Grigor C et al Lancet 2004; 364: 263 -269.

TICORA Aim for a Target –TICORA Trial Radiographic Results at 18 Months Routine Care (n=53) Intensive Care (n=50) P-value 3 0. 5 p=0. 002 Joint space narrowing* 4. 5 3. 25 p=0. 331 Total Sharp score* 8. 5 4. 5 p=0. 02 Erosions score* * Median (IQR) increase in score Grigor C et al Lancet 2004; 364: 263 -269.

Control of Structural Damage is Greatest with Continuous Control of Disease Activity* Const. Low DAS Fluct. High DAS 160 140 120 100 Sharp Score 120 80 60 40 Baseline TSS = 20 20 0 Const. High DAS 0 3 6 Time (Yrs) * RF Positive Patients Welsing et al. Arthritis Rheum 2004; 50: 2082 -93 9 80 60 40 Baseline TSS = 0 20 0 0 3 6 Time (Yrs) 9

Does good clinical control translate into NO radiographic progression?

Radiological Damage in RA Patients on Sustained Remission Grégory C, et al. Abstract 346, ACR 2006. ? is their radiological progression over 5 -years in recent RA patients with persistent remission (Between Y 3 and Y 5) 191 RA patients <1 year on SSZ, MTX or Both Available patients: 134 30 (22. 4%) Remission with DAS 44 <1. 6 at 3 and 5 years n 6 (20%) patients had radiographic progression or new erosions between Y 3 and Y 5

Remission on DMARDs n. DMARDs frequently produce clinical remission n. DMARDs rarely produce imaging remission n. Hence DMARDs rarely produce true remission n. Explains progression of damage in patients in clinical remission on DMARDs? n. What happens with TNF antagonists?

Predictors of radiographic progression in early RA patients treated with MTX

CRP Change And Radiographic Progression - PREMIER Trial % with No Radiographic Progression CRP Levels: van der Heijde DF, et al. Ann Rheum Dis 2005; 64(Suppl III): 436 -7 (SAT 0085)

CRP Change And Radiographic Progression - PREMIER trial % with No Radiographic Progression CRP Levels: van der Heijde DF, et al. Ann Rheum Dis 2005; 64(Suppl III): 436 -7 (SAT 0085)

Predictors of radiographic progression of patients treated with MTX in the ASPIRE trial n Baseline CRP n Baseline ESR n Week 14 DAS n Mean CRP over 52 weeks n Mean ESR over 52 weeks Smolen J et al. Arthritis Rheum 2006; 54: 702

DAS 28 after 14 wks of MTX Tx Predicts Rapid Radiographic Progression If a ERA subject continues to have a DAS 28 score > 4 after 14 weeks of MTX 20 mg the subject can expect to experience rapid radiographic progression. Smolen J et al. Arthritis Rheum 2006; 54: 702

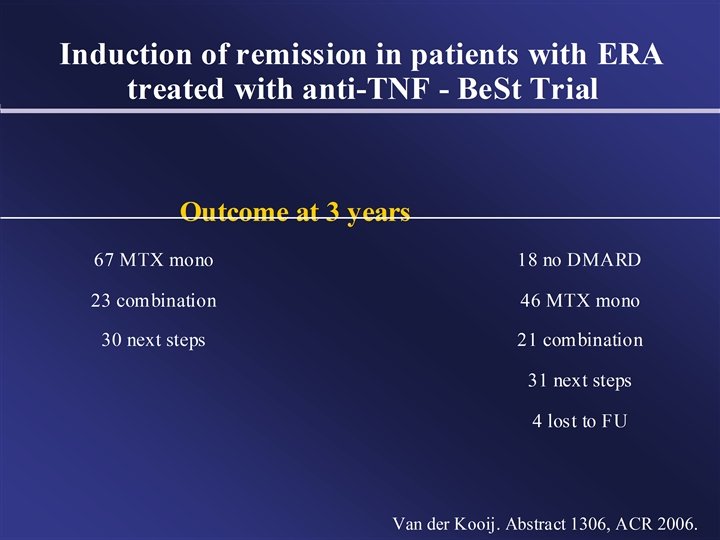
Induction and Maintenance of Remission in Early RA

Be. St Treatment Strategies in Early RA Sequential MONO-Therapy STEP-UP Therapy Initial COMBO Therapy Initial BIOLOGIC Therapy 1. MTX MTX + SSZ + PRED MTX + Biologic 2. SSZ MTX + CSA + PRED SSZ 3. LEF MTX + SSZ + HCQ MTX + Biologic LEF 4. MTX + Biologic MTX + SSZ + HCQ + PRED 5. MTX + Biologic MTX + CSA + PRED

Early DMARD Intervention - Be. ST Trial Year 2 Outcomes Radiographic Progression p = 0. 003* * Overall P-value, SDD = smallest detectable difference Goekoop-Ruiterman YPM, et al. Abstract L 4 ACR 2004.

Be. St Trial - Disposition of patients in the anti-TNF arm: n 120 enrolled n 8 stopped for side effects n 22 did not achieve response n 13 continued n 77 stopped because they achieved a DAS 44 <2. 4 – 46 were on 3 mg/kg – 22 on 6 mg/kg – 6 on 7. 5 mg/kg – 3 on 10 mg/kg Van der Bijl AE, et al. ACR 2005, Abstract 876.

Sustainability of response

TEMPO Trial Failure on 1 DMARD No recent MTX Baseline Endpoints ACR-N 24 Weeks Total Sharp Score 52 Weeks Enbrel® (etanercept) + MTX (n=231) Randomized (N=686) ITT Population (N=682) ENBREL (n=223) MTX (n=228) – Withdrawals: MTX, 30%; ENBREL, 24%; ENBREL + MTX, 16% Klareskog et al. Lancet 2004; 363: 675 -81

TEMPO Trial - Year 3 Results ACR Response 86 † ‡ 90 Percent of Patients 80 70 71 75 71 † ‡ 60 MTX (n=228) Etanercept (n=223) Etanercept + MTX (n=231) 54* 50 49† ‡ 42 40 27 30 21 20 10 0 ACR 20 van der Heijde D, et al. ACR 2005, Abstract L 10. ACR 50 ACR 70 * p<0. 05, etanercept vs. MTX † p<0. 05 combination vs. MTX ‡ p<0. 05 combination vs. etanercept

TEMPO Trial - Year 3 Results DAS 44 Remission †‡ van der Heijde D, et al. ACR 2005, Abstract L 10. * p<0. 05, E vs. MTX † p<0. 05, combination vs. MTX ‡ p<0. 05, combination vs. E

What about Radiographic Progression ?

Primary Radiographic Endpoint: Change in TSS From Baseline - Year 3 5. 95 (CI 2. 96, 8. 94) 1. 61* (CI 0. 41, 2. 81) * p < 0. 05, Etanercept vs MTX † p < 0. 05, combination vs MTX ‡ p < 0. 05, combination vs Etanercept van der Heijde D, et al. ACR 2005, Abstract L 10 -0. 14†‡ (CI – 1. 07, 0. 78)

Long-term Safety & Efficacy TEMPO Trial - Year 3 Results No Radiographic Progression van der Heijde D, et al. ACR 2005, Abstract L 10

TEMPO trial - Disconnect between Disease Activity / Inflammation and Radiographic Progression (2 year data) Patients were startified according to: n CRP levels: < 5 mg/L ; 5 -15; > 15 n DAS 44: – <1. 6 (remission) /1. 6 -2. 4 (Low disease activity) – 2. 4 -3. 7 (moderate diseaseactivity) – >3. 7 (high disease activity) Results: n In the MTX group only the High CRP and High DAS progress n In the MTX + ETN no progresson regardless of CRP level and disease activity Landewé R et al. ACR 2005, Abstract 867.

TEMPO trial - Disconnect between Disease Activity Radiographic Progression Change in Sharp Score by Treatment Group Stratified For Subcategories of ta-CRP* * Time-averaged CRP Landewé R et al. Abstract 867, ACR 2005.

Disconnect Between Disease Activity and Radiographic Progression Change in Sharp Score by Treatment Group Stratified for Subcategories of ta-DAS* * Time-averaged DAS Landewé R et al. Abstract 867, ACR 2005.

Conclusions n Halting of radiographic progression is achievable for many patients n DMARDs produce clinical remission but structural damage may progress, due to incomplete suppression of synovitis n TNF blockade (with MTX) can halt structural damage due to more complete suppression of synovitis, and ? direct osteoclast effect
- Slides: 43