Rehabilitation of Post Mastectomy Syndrome Eric Wisotzky MD

Rehabilitation of Post. Mastectomy Syndrome Eric Wisotzky, MD Director of Cancer Rehabilitation Med. Star National Rehabilitation Network Assistant Professor of Rehabilitation Medicine Georgetown University School of Medicine

Disclosures • None

Objectives • Therapy techniques for post-mastectomy syndrome • Rehabilitation precautions for post-mastectomy syndrome • Medications for post-mastectomy syndrome • Interventional procedures for post-mastectomy syndrome • Prevention of post-mastectomy syndrome

Therapy Techniques Effectiveness of Postoperative Physical Therapy for Upper-Limb Impairments After Breast Cancer Treatment: A Systematic Review De Groef, An et al. Archives of Physical Medicine and Rehabilitation 2015; 96: 1140 -53.

Therapy Techniques: Passive Mobilization • One study showed beneficial effects of passive mobilization on shoulder pain and ROM – Followed patients for 8 -24 months post-op Le Vu B, Dumortier A, Guillaume MV, Mouriesse H, Barreau-Pouhaer L. Efficacy of massage and mobilization of the upper limb after surgical treatment of breast cancer. Bulletin du Cancer 1997; 84: 957 -61.

Therapy Techniques: Stretching • One study investigating pectoral stretching program compared to a home exercise program consisting of ROM exercises – Followed patients for 7 months – No difference in pain or ROM Lee TS, Kilbreath SL, Refshauge KM, Pendlebury SC, Beith JM, Lee MJ. Pectoral stretching program for women undergoing radiotherapy for breast cancer. Breast Cancer Res Treat 2007; 102: 313 -21.

Therapy Techniques: Exercise Therapy • Five studies investigated the effectiveness of exercise therapy (shoulder exercises) – All found beneficial effect on shoulder ROM – One found positive effect on pain • Active physical therapy vs home exercise program – Great variability in terms of type of exercises, frequency, intensity, and duration of programs De Groef, An, et al. Effectiveness of Postoperative Physical Therapy for Upper-Limb Impairments After Breast Cancer Treatment: A Systematic Review. Archives of physical medicine and rehabilitation (2015)

Therapy Techniques: Multifactorial • Two studies showed multifactorial therapy consisting of manual stretching and active exercises effectively treated impaired shoulder ROM at 6 months post-op De Groef, An, et al. Effectiveness of Postoperative Physical Therapy for Upper-Limb Impairments After Breast Cancer Treatment: A Systematic Review. Archives of physical medicine and rehabilitation (2015)
 more beneficial")
Therapy Techniques: Timing of Therapy • Three studies showed early start (POD#1) more beneficial for recovery of ROM • Four studies showed greater incidence of seromas and wound drainage in group with early start vs those starting >7 days post-op De Groef, An, et al. Effectiveness of Postoperative Physical Therapy for Upper-Limb Impairments After Breast Cancer Treatment: A Systematic Review. Archives of physical medicine and rehabilitation (2015)

Therapy Techniques: Authors’ Recommendations • First week post-op: low-intensity program involving elbow/wrist • 7 -10 days post-op: gradually increase intensity – Passive mobilization, manual stretching, active exercises • No recommendations can be made on length of time, content, intensity De Groef, An, et al. Effectiveness of Postoperative Physical Therapy for Upper-Limb Impairments After Breast Cancer Treatment: A Systematic Review. Archives of physical medicine and rehabilitation (2015)

Post-mastectomy Syndrome: Occupational Therapy • Patients need help with ADLs • Difficulty with household chores, dressing Thomas-Mac. Lean, Roanne L. , et al. "Arm morbidity and disability after breast cancer: new directions for care. " Oncology nursing forum. Vol. 35. No. 1. 2008
")
Therapy Techniques for Specific Syndromes: • • • Incisional pain Axillary Web Syndrome (cording) Shoulder dysfunction Post-Reconstruction Pain Syndrome Neuropathic syndromes – Intercostobrachial neuralgia – Phantom breast pain

Therapy Techniques: Incisional Pain From local adherence of incision to chest wall Presents with incisional hypersensitivity Decreased mobility of incision

Therapy Techniques: Incisional Pain • Scar massage/mobilization • Desensitization techniques
 • • • Often spontaneously resolve Soft tissue")
Therapy Techniques: Axillary Web Syndrome (Cording) • • • Often spontaneously resolve Soft tissue techniques Nerve glides ROM May have audible “snap”

Shoulder Dysfunction: Impingement Protective posturing/radiation Shortening of pec muscles Decreased size of subacromial arch due to forward depressed shoulder girdle Rotator cuff dysfunction/impingement

Shoulder Dysfunction: Range of Motion in Breast Cancer • Decreased planes of motion: – flexion – abduction – external rotation Levangie PK, Drouin J. Magnitude of late effects of breast cancer treatments on shoulder function: a systematic review. Breast Cancer Res Treat 2009; 116(1): 1– 15

Shoulder Dysfunction: Scapular Mechanics • Scapulothoracic motion altered in all planes Shamley, et al. Three-dimensional scapulothoracic motion following treatment for breast cancer. Breast Cancer Res Treat (2009) 118: 315 -322

Shoulder Dysfunction: Muscle Strength • Multiple studies have shown weakness in: – – – Abduction Flexion Extension External/internal rotation Scapular upward rotation/depression/adduction

Based on above findings, a sensible PT rx might include: • Pec stretching • Scapular stabilization/mechanics exercises • Strengthening in all planes
 • Neuromuscular symptoms including: paresthesias, dysesthesias, cramping, spasms, or other")
Post-Reconstruction Pain Syndrome (PRPS) • Neuromuscular symptoms including: paresthesias, dysesthesias, cramping, spasms, or other characteristically neuropathic discomfort in the chest wall, shoulder, upper arm, abdomen, and/or back following breast surgery with reconstruction for breast cancer.

Therapy Techniques: PRPS • Stretching of pectoralis and serratus • Manual release of tissues around implant/tissue expander

Intercostobrachial Neuralgia
 • Supplies")
Intercostobrachial Nerve • Cutaneous branch of 2 nd intercostal nerve (T 2) • Supplies the posterior and medial upper arm, axilla, and lateral chest wall – Much anatomic variation • Increase risk of injury during ALND

Therapy Techniques: Intercostobrachial Neuralgia • Desensitization

Therapy Techniques: Phantom Breast Pain • Desensitization • Mirror therapy

Therapy Precautions • Caution with manual therapy around tissue expander/implant • Common sense lymphedema precautions – Avoid aggressive deep tissue work to lymphedematous limb or limb at risk of lymphedema

“ABSOLUTE” Precautions • Avoid physical agents or e-stim directly over active tumor • Avoid heat/ice in potentially ischemic or insensate areas • Avoid heat in patients at high bleeding risk • Avoid heat/ice, e-stim, TENS in areas at risk for fracture • Avoid traction in area of malignancy – Fracture risk

Post-mastectomy Syndrome: Medications

Post-mastectomy Syndrome: Oral Medications • Anti-depressants – Venlafaxine showed significant pain relief vs placebo Tasmuth, Tiina, Brita Härtel, and Eija Kalso. Venlafaxine in neuropathic pain following treatment of breast cancer. European journal of pain 6. 1 (2002): 17 -24. – Amitriptyline 25 -100 mg daily resulted in >50% pain relief in 8/15 patients • Randomized placebo controlled crossover study Tasmuth, Tiina. Amitriptyline effectively relieves neuropathic pain following treatment of breast cancer. Pain 64. 2 (1996): 293 -302.

Post-mastectomy Syndrome: Topical Medications • Capsaicin – Randomized, placebo controlled trial – 5/13 patients using capsaicin had >50% pain relief – 1/10 in placebo group had >50% pain relief Watson, C. Peter N. , and Ramon J. Evans. The postmastectomy pain syndrome and topical capsaicin: a randomized trial. Pain 51. 3 (1992): 375379

Post-mastectomy Syndrome: Topical Medications • Lidocaine patch – 28 patients randomized to lidocaine patch vs placebo patch – No difference in pain scores between the two groups Cheville, Andrea L. , et al. Use of a lidocaine patch in the management of postsurgical neuropathic pain in patients with cancer: a phase III doubleblind crossover study (N 01 CB). Supportive care in cancer 17. 4 (2009): 451460.

Post-mastectomy Syndrome: Other Medications Anti-inflammatories: topical or oral Nerve stabilizers: gabapentin, pregabalin Duloxetine Opioids Topical compounds

Post-mastectomy Syndrome: Modalities • TENS no better than placebo for postmastectomy pain Robb, Karen A. , Di J. Newham, and John E. Williams. "Transcutaneous electrical nerve stimulation vs. transcutaneous spinal electroanalgesia for chronic pain associated with breast cancer treatments. " Journal of pain and symptom management 33. 4 (2007): 410 -419.

Post-mastectomy Syndrome: Acupuncture • Randomized controlled trial of acupuncture vs usual care showed decreased pain and improved ROM in the acute postoperative period after breast surgery He, J. P. , et al. "Pain-relief and movement improvement by acupuncture after ablation and axillary lymphadenectomy in patients with mammary cancer. " Clinical and experimental obstetrics & gynecology 26. 2 (1998): 81 -84.

Injections in Post-mastectomy Syndrome Can they be performed?

Injections in Post-mastectomy Syndrome Can they be performed? Yes for the most part…

Injections in Post-mastectomy Syndrome Can they be performed? Yes for the most part… Precautions to consider: -Wounds -Skin issues during radiation -Blood counts during chemotherapy -Lymphedema/infection risk

Injections in Post-mastectomy Syndrome: Musculoskeletal • Rotator cuff impingement subacromial injection • Adhesive capsulitis glenohumeral injection • Myofascial pain trigger point injection

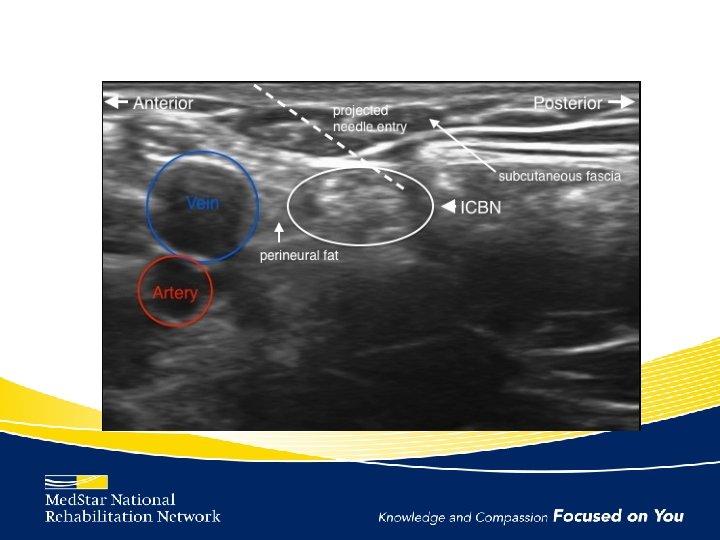
Intercostobrachial Neuralgia Management • Intercostobrachial nerve block

Intercostobrachial Nerve Block Technique

Case Series for Intercostobrachial Nerve Block Patient Baseline A 6/10 B 6/10 C 10/10 2 weeks 4 weeks 6 weeks 3 months 4/10 (2 nd inj) 2/10 0/10

Neuroma Injections • 19 patients injected • 93% had complete relief of pain after injection of T 4 and/or T 5 neuromas with bupivicaine and dexamethasone Tang CJ, Elder SE, Lee DJ, Rabow MW, Esserman LJ: 2013 San Antonio Breast Cancer Symposium Abstract P 3 -10 -03. Presented December 12, 2013. http: //cancer. ucsf. edu/videos/Esserman_v 4. mp 4

Neuroma Injections

Neuropathic Chest Wall Pain • • • Intercostal Nerve Block Paravertebral Nerve Block Intercostal Neurolysis Thoracic Nerve Pulse Radiofrequency Ablation Intrathecal Pump Gulati, Amitabh, et al. A retrospective review and treatment paradigm of interventional therapies for patients suffering from intractable thoracic chest wall pain in the oncologic population. Pain Medicine 16. 4 (2015): 802 -810.

Botulinum Toxin for Post-Reconstruction Pain Syndrome • Consider injecting pectoralis major, serratus anterior • Don’t pop the implant! – Can use ultrasound

Botulinum Toxin for Post-Reconstruction Pain Syndrome: Evidence • 100 units botulinum toxin A in pec major resulting in 100% pain relief for 6 weeks • 250 units of abobotulinumtoxin A into pec major resulting in 100% pain relief for 4 weeks O'Donnell, Casey J. Pectoral muscle spasms after mastectomy successfully treated with botulinum toxin injections. PM&R 3. 8 (2011): 781 -782.

Botulinum Toxin for Radiation Fibrosis Syndrome • 87% of patients reported self-reported benefits from the injections Stubblefield, Michael D. , et al. "The role of botulinum toxin type A in the radiation fibrosis syndrome: a preliminary report. " Archives of physical medicine and rehabilitation 89. 3 (2008): 417 -421.

Post-mastectomy Syndrome: Prevention Regional anesthesia • 40 patients assigned to general anesthesia vs general anesthesia plus paravertebral nerve block • Patients in the nerve block group had significantly less chronic pain than general anesthesia alone 4 -5 months post-op Ibarra, M. M. , et al. Chronic postoperative pain after general anesthesia with or without a single-dose preincisional paravertebral nerve block in radical breast cancer surgery. Revista espanola de anestesiologia y reanimacion 58. 5 (2011): 290 -294.

Post-mastectomy Syndrome: Prevention EMLA › 46 patients randomized to chest wall EMLA cream vs placebo peri-operatively › 5 min before surgery and then daily for 4 days post-op › Placed on sternum, supraclavicular region, and axilla › Pain intensity significantly less in EMLA group 3 months post-op Fassoulaki, Argyro, et al. EMLA reduces acute and chronic pain after breast surgery for cancer. Regional anesthesia and pain medicine 25. 4 (2000): 350 -355

Post-mastectomy Syndrome: Prevention Gabapentin peri-operatively › Single dose of 600 mg gabapentin one hour preoperatively › Treatment group had less post-op pain and less opioid consumption in first day after surgery Grover, V. K. , et al. A single dose of preoperative gabapentin for pain reduction and requirement of morphine after total mastectomy and axillary dissection: randomized placebocontrolled double-blind trial. Journal of postgraduate medicine 55. 4 (2009): 257.

Post-mastectomy Syndrome: Prevention Minimizing pre-op pain/ROM restrictions PREHAB!!

Post-mastectomy Syndrome: Prevention – Psychological Factors • Depression • Anxiety • Catastrophizing Schreiber, K. L. , et al. (2014). "Predicting, preventing and managing persistent pain after breast cancer surgery: the importance of psychosocial factors. " Pain Manag 4(6): 445 -459

Intercostobrachial Neuralgia Prevention • Prevention: – Nerve sparing surgery may or not help prevent this pain syndrome • Meta-analysis showed that complaints when nerve is severed are typically numbness which may be less bothersome Warrier S, Hwang S, Koh CE, Shepherd H, Mak C, Carmalt H, Solomon M. Preservation or division of the intercostobrachial nerve in axillary dissection for breast cancer: Meta-analysis of Randomised Controlled Trials. Breast. 2014 Feb 24

Post-Reconstruction Pain Syndrome Prevention • Botulinum toxin injected into pec major, serratus, rectus abdominus intra-operatively during mastectomy and tissue expander placement – Botulinum toxin group had significantly less post-op pain and narcotic use than control group at initial and final tissue expansions Layeeque, Rakhshanda, et al. Botulinum toxin infiltration for pain control after mastectomy and expander reconstruction. Annals of surgery 240. 4 (2004): 608.

Summary • Post-mastectomy syndrome rehabilitation often requires a multimodal approach • Patient assessment should look for specific cause of symptoms which will dictate treatment options • Much is still not known so many research possibilities

Questions? ? ? Eric. m. wisotzky@medstar. net
- Slides: 58