Regulation of the Glomerular filtration and renal blood

Regulation of the Glomerular filtration and renal blood flow Dr. Waleed R. Ezzat

Lecture Objectives: 1. Understand the autoregulation and tubulo-glomerular feedback 2. Understand the juxtaglomerular apparatus and its role in reninangiotensin system 3. Understand the glomerulo-tubular balance

Introduction: • Both kidneys receive about 22% of the cardiac output (about 4 ml/min. gm). This is the highest blood flow compared with other organs (except for neurohypophysis and carotid bodies). • This high rate of flow is not a result of excessive metabolic demands. • Renal medulla receives only 1 -2% of total renal blood flow through the vasa recta. Vasa recta play an important role in allowing the kidneys to form a hyperosmolar environment in the medullary region, and thereby to form concentrated urine. • Regulation of the renal blood flow leads to the regulation of glomerular filtration rate (GFR). • The highest renal vascular resistance is in the efferent arteriole (≈ 45%), then the afferent arteriole (≈ 25%) of the total resistance.

Renal Blood Flow Control: • Renal blood flow control is believed to be due to: 1. Intrinsic mechanism (Autoregulation) 2. Extrinsic mechanism (nervous and blood-borne hormones) • Substances cause vasoconstriction in the kidneys include adenosine (A 1 receptor), angiotensin II, endothelin, epinephrine, norepinephrine, thromboxane A 2, and vasopressin. • Substances cause vasodilation in the kidneys include atrial natriuretic peptide (ANP), dopamine, histamine, kinins, nitric oxide (NO), PGE 2 and PGI 2.
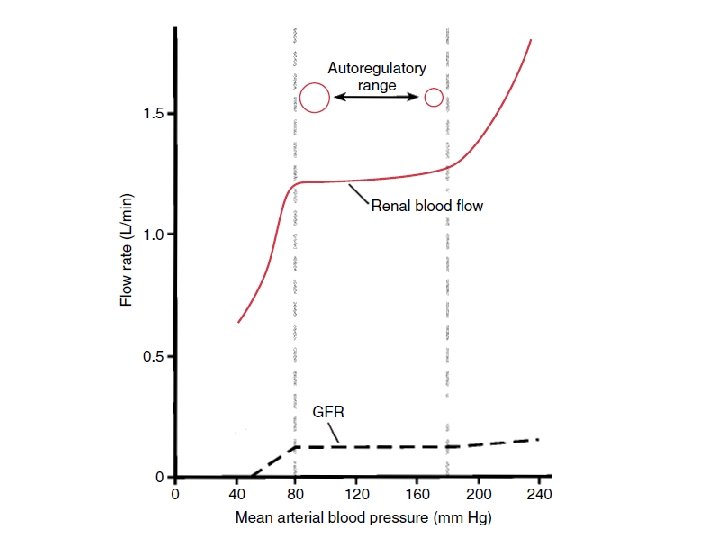
: • Renal autoregulation mechanism maintains renal blood flow")
Renal Blood Flow Control (cont. ): • Renal autoregulation mechanism maintains renal blood flow and GFR relatively constant over an arterial blood pressure range of 80 -170 mm. Hg. • Autoregulation is an intrinsic property of the kidneys and is observed in an isolated perfused kidney devoid of external nerves. • Although all renal arterioles are richly innervated by sympathetic nerves, reflex sympathetic stimulation has an unimportant role in long-term control of renal blood flow. Sympathetic stimulation is important in reducing GFR during severe disturbances (e. g. severe hemorrhage). The same concept is applied to plasma levels of adrenaline and noradrenaline (released from adrenal medulla). • Local release of Nitric Oxide (NO) and prostaglandins and bradykinin may damper the renal vasoconstrictor effects of the sympathetic nerves and angiotensin II (as seen in chronic heart failure), especially their effects to constrict the afferent arterioles. • Administration of NSAIDs in chronic heart failure can cause acute renal failure by negating the renal protective effects of the renal prostaglandins.

Autoregualtion of renal blood flow: • Autoregulation is evident even in isolated, denervated, perfused kidney. • Renal autoregulation tends to maintain a relatively constant GFR to allow precise control of renal excretion and blood volume. • Changes in arterial pressure still have significant pressure diuresis or pressure natriuresis effects. • Two mechanisms account for renal autoregulation. Both regulate the tone of the afferent arteriole. These two mechanisms are; – The myogenic mechanism – The tubuloglomerular feedback mechanism • In the myogenic mechanism; an ↑ blood pressure → opening of stretch activated cation channels in smooth muscle cells → opening of voltage-dependent Ca 2+ channels → ↑ intracellular Ca 2+ concentration → smooth muscle contraction

Tubuloglomerular feedback Mechanism: • In this mechanism the macula densa serves as the detector and the glomerulus acts as the effector. • Macula densa is a collection of densely packed epithelial cells at the junction of the thick ascending limb and distal convoluted tubule. • ↑ Na+ delivery to macula densa →↑ release of ATP form macula densa → metabolized to adenosine in juxtaglomerular interstistium → afferent arteriolar vasoconstriction -ve feedback ↓ GFR -ve feedback Dilation of afferent arteriole ↓ Na. Cl delivery to Macula densa ↑ renin release from juxta-glomerular cells of afferent & efferent Constriction of efferent Angiotensin II

Proposed mechanism of adenosine acting as a mediator of the tubuloglomerular feedback. ADO= intra- and/or extracellular generation of adenosine 5’-NT= ecto-5’-nucleotidase MC= mesangium cells VSMC= vascular smooth muscle cells of the afferent arteriole NOS I= neuronal nitric oxide synthase COX-2= cyclooxygenase-2

• In decreased arterial pressure or volume depletion, angiotensin II increases GFR and decreases flow through the peritubular capillaries (it constricts efferent arterioles). This reduction in renal blood flow (and pressure) in the peritubular capillaries leads to ↑ reabsorption of Na+ and water.

The glomerulotubular balance: It is the intrinsic ability of renal tubule to increase their reabsorption rate when GFR rises (i. e. increased tubular load). Thus, it buffers the effect of spontaneous changes in GFR on urine output.

Test Question: Q. Renal autoregulation? A. Is associated with increased renal vascular resistance when arterial blood pressure is lowered from 100 to 80 mm. Hg B. Mainly involves changes in the caliber of efferent arterioles C. Maintains a normal renal blood flow during severe hypotension (blood pressure, 50 mm. Hg) D. Minimizes the impact of changes in arterial blood pressure on renal Na+ excretion. E. Requires intact renal nerves
- Slides: 12