REFRACTORY PERIODONTITIS contents Introduction Definition Etiology Clinical features




 is the most enigmatic and difficult to treat among different")

 Refractory periodontitis is a distinct entity different from other types of periodontitis. Refractory")


























- Slides: 34
REFRACTORY PERIODONTITIS
contents Introduction Definition Etiology Clinical features Difference between recurrent and refractory Diagnosis Treatment consideration conclusion
What is refractory means
Refractory 1. stubborn or unmanageable. 2. resistant to a process or stimulus. 3. a substance that is resistant to heat.
Introduction Refractory Periodontitis (RP) is the most enigmatic and difficult to treat among different categories of inflammatory periodontal diseases. . Fortunately it is relatively rare but still remains a significant clinical challenge.
DEFINITION According to AAP, Refractory periodontitis has been defined as those cases of periodontitis which do not respond to any type of conventional periodontal therapy whatever the thoughness or frequency
1) Refractory periodontitis is a distinct entity different from other types of periodontitis. Refractory Periodontitis results from different bacterial agents, specific alteration of the host response or a combination of these factors. According to this view, multiple categories or subtypes of refractory patients may exist. √ 2) Refractory periodontitis is not a distinct entity and all cases of refractory periodontitis can fall into some of other categories of periodontitis. Refractory periodontitis are most often seen during the management of aggressive and chronic forms of periodontitis.
Refractory periodontitis is not currently considered a separate disease entity, patients who fail to respond to conventional therapy are considered to have periodontitis that is “ refractory” to treatment It is possible to characterize any form of periodontal disease( e. g. , chronic periodontitis, aggressive periodontitis) as refractory to the treatment.
Etiology: Etiology behind lack of response to therapy is unknown Contributing factors Refractory periodontitis may be due to an abnormal host response, or an universally pathogenic and virulent microflora or smoking. high proportion of a A. actinomycetemcomitans and P . intermedia have been reported in refractory periodontitis.
Walker et al have indicated that atleast two patterns or rates of attachment loss may be associated with refractory periodontitis. Pattern associated with rapid loss of attachment was characterized by a gram negative form that contained Spirochetes, P. intermedia and Fusobacterium species. A slow continuous rate was associated with a predominantly gram positive flora
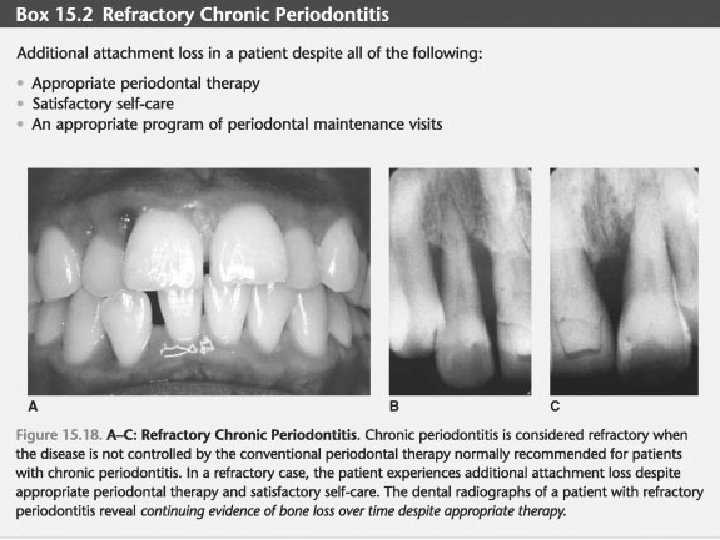
Clinical features: Pretreatment clinical findings and severity are not diagnostic of refractory periodontitis. Continuous/progressive attachment loss , bone loss inspite of adequate treatment and good oral hygiene maintained by the patient. Deterioration in cases of refractory periodontitis occurs either by new involvement of additional teeth or by increased bone and attachment loss in previously located areas.
Diagnosis Difficult to rule out After the treatment , if patient has not responded as expected , the clinician should rule out the following conditions 1. Inadequately treated periodontitis 2. Poor plaque control 3. Endodontic infection A case may be considered as refractory periodontitis only when loss of periodontal attachment and bone continues after well executed treatment in a good oral hygiene and no other infections or etiologic factors
Difference between Refractory periodontitis Recurrent periodontitis Any inflammatory type of periodontitis which does not respond to conventional therapy Any type of periodontitis which initially responds well to the conventional therapy but recurrs within no time Progressive attachment loss inspite of adequate conventional therapy and presence of good plaque control Occurs due to either inadequate treatment, poor plaque control, or presence of endodontic infection which prevent normal periodontal healing Etiology unknown , contributing factors are etiology known…. Inadequate removal of 1. abnormal host response pathogenic mos 2. pathogenic and virulent microflora or 3. smoking. Difficult to manage Easy to manage Systemic antibiotics, frequent recalls needed Adequate treatment and good plaque control needed.
TREATMENT CONSIDERATIONS Once the diagnosis of “refractory” periodontitis has been made, the following steps may be taken: 1. Collection of subgingival microbial samples from selected sites for analyses, possibly including antibiotic-sensitivity testing. 2. Selection and administration of an appropriate antibiotic regimen. 3. In conjunction with the administration of an antimicrobial regimen, conventional periodontal therapies may be used.
4. Reevaluation with microbiological testing as indicated. 5. Identification and attempt to control risk factors (e. g. , smoking). 6. Intensified periodontal maintenance program which may include shorter intervals between appointments with microbiologic testing if indicated (Parameter on Periodontal Maintenance
Management Frequent and intensive recall maintenance and home care programm is necesarry Systemic antibiotics is adminitered to support the host immune system The most common recommended regimens utilize monotherapy administrations of Doxycycline, Clindamycin, Metronidazole or Ciprofloxacin, or with a combination of Metronidazole and Amoxicillin or Ciprofloxacin
Antibiotics and its dosage antibiotic Dose and frequency Amox clavulanate potassium metronidazole 250 mg amox 150 mg clav tid for 14 days 500 mg tid for 7 days clindamycin 150 mg qid for 7 days
Combination therapy Combinations of antibiotic Amox clav/ metro clav Metro and ciprofloxacin Amox and dox Mos AA associated periodontitis Enteric rods and pseudomonads Aa and pg
Host modulating agents Periostat®, a low dose 20 mg. Doxycycline formulation taken twice daily, therefore, is an important new therapy to combat against Refractory Periodontitis when used as an adjunct to scaling and root planing. This low dose doxycycline, part of the tetracycline family does not create bacterial resistance
ATRIDOX® Atridox, a Doxycycline Hyclate based bioabsorbable gel formula is the only localized slow release agent It may be used as a monotherapy but preferably in combination with scaling and root planing. The advantage of this treatment method is that it delivers a high dose of concentration of agent directly to the site, while avoiding the drawbacks of systemic administration The advantage of Atridox is its capacity to release into the crevicular fluid a high concentration of antibiotic (940 times higher than that achieved by a systemic antibiotic) for a period of seven to 10 days,
PHOTODYNAMIC DISINFECTION . This technique uses a non-thermal diode laser which is absorbed into a photosensitizing solution that is irrigated into the subgingival environment. The activated photosensitizing solution, which is mucoadherent, attaches to the cell wall of the bacteria, creating a free radical of oxygen and through the peroxidation of lipids, ruptures the bacterial cell wall. Being photodynamic in nature rather than a systemic antibiotic, it does not result in bacterial resistance
TOOTH EXTRACTION WITH DENTAL IMPLANT REPLACEMENT When treatment measures fail to arrest the progression of periodontal disease, the extraction of the affected tooth may predictably solve the periodontal problem. The replacement of this tooth can be considered if sufficient alveolar support remains to facilitate the satisfactory integration of a root form analogue into the existing alveolar housing.
OUTCOMES ASSESSMENT 1. The desired outcome for patients with “refractory” periodontitis includes arresting or controlling the disease. 2. Due to the complexity and many unknown factors of “refractory” periodontitis, control may not be possible in all instances. In such cases, a reasonable treatment objective is to slow the progression of the disease.
CONCLUSION The concept of periodontal disease as localized entities affecting only the teeth and supporting apparatus is over simplified and needs to be revised. Refractory periodontitis should be treated vigorously and combination therapies should be tried to avoid progression of disease.
1. Refractory periodontitis is not a distint entity and therefore removed from classification of periodontal diseases in year 1. 1989 2. 1947 3. 1999 4. none of the above
2. Periodontitis which does not respond to conventional periodontal therapy is known as 1. Chronic periodontitis 2. Recurrent periodontitis 3. Refractory periodontitis 4. Aggressive periodontitis
3. Recurrent periodontitis is different from refractory periodontitis in following aspect 1. continuous Loss of attachment 2. Inadequate therapy and poor plaque control 3. Post treatment diagnosis 4. All of the above
Systemic antibiotics are not indicated in 1. refractory periodontitis 2. chronic periodontitis 3. aggressive periodontitis 4. recurrent/chronic periodontitis
Atridox is local antibiotic drug of following family 1. tetracyclin 2. penicillin 3. aminoglycosides 4. fluroquinolones
One of the contributing cause of refractory periodontitis 1. poor oral hygiene 2. inadequate scaling 3. presence of systemic disease 4. smoking
Organisms suspected to play rapid attachment loss in refractory periodontitis is 1. gram positive aerobic 2. gram positive anerobic 3. gram negative aerobic 4. gram negative anerobic
Periostat is host modulating agent prescribed in following dosage 1. 100 bd 2. 200 od 3. 20 bd 4. 20 tid
Thank you