REFLEKSI KASUS STROKE LOBUS OCCIPITAL Hemianopsia Homonim I
 I Made Dolly Oktayana – 17767")
REFLEKSI KASUS STROKE LOBUS OCCIPITAL (Hemianopsia Homonim) I Made Dolly Oktayana – 17767

CASE

PATIENT IDENTITY • Name : Mr. A • Age : 48 y. o • Gender : Male • Address : Ponorogo • Occupation : Freelance • Education : S 1 • Religion : Islam • Marriage : Yes • No CM : xx. xx • Admited : 11 September 2020

CHIEF COMPLAIN LOSS OF VISUAL FIELD

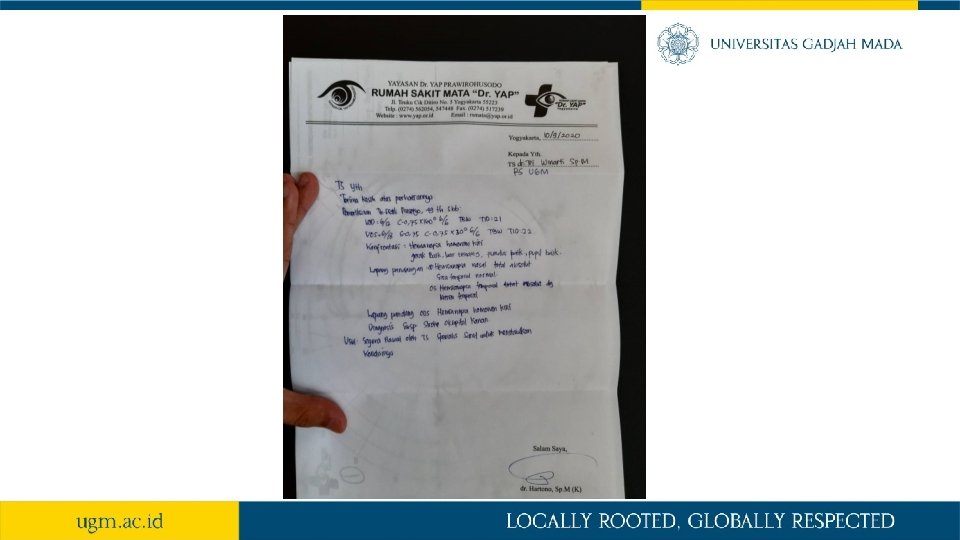
ANAMNESIS CURRENT HISTORY: • 2 days SMRS patient complained that he unable to drive properly dan often hit the road. He described that on the left side of his visual field is covered with black shadow dan while driving object just appeared without he being noticed. Extremity weakness and other complain denied. • Day of MRS patient consult to eye specialist and perimetry test has been conducted and found defect of visual field and refered to neurology department RSA with suspect of occipital stroke dextra. • History of HT (-), DM (-), Dyslipidemia (-), Glasses (-)
, HT (-) • Stroke (-), tumor (-) FAMILY")
ANAMNESIS PAST HISTORY: • DM (-), HT (-) • Stroke (-), tumor (-) FAMILY HISTORY: • History of typical symptoms (-) • DM (-), HT (-), Stroke (-), Tumor (-)

ANAMNESIS SISTEM • Sistem cerebrospinal : loss of left side visual field. • Sistem kardiovaskular : none • Sistem respirasi : none • Sistem gastrointestinal : none • Sistem musculoskeletal : none • Sistem integumentum : none • Sistem urogenital : none

RESUME ANAMNESIS • Male, 48 y. o, with chief complain acute sudden loss of left side visual field since 2 days ago that isn’t improve since. Other symptoms denied. • History of comorbid condition denied

WORKING DIAGNOSIS • CLINICAL DIAGNOSIS: Acute loss of visual field temporal left eye and nasal right eye • TOPICAL DIAGNOSIS: Lesion of primary visual cortex lobus occipital dextra dd Tractus opticus dextra • ETIOLOGICAL DIAGNOSIS: Vascular: stroke non hemorrhagic lobus occipital dextra

PHYSICAL EXAMINATION General Status • Keadaan umum • Kesadaran • Vital Sign • TD • Nadi • Respirasi • Suhu • NPS : Baik : Compos Mentis, GCS E 4 V 5 M 6 : : 130/90 mm. Hg : 75 kali per menit : 20 kali per menit : 36, 5 o C : 0
, SI (-/-) • Leher :")
PHYSICAL EXAMINATION General status • Kepala : CA (-/-), SI (-/-) • Leher : JVP 5+2 • Dada - Paru : Vesikuler (+/+) - Jantung : S 1 -S 2 reguler • Abdomen: bising usus (+) • Ekstremitas: edema (-)
 Status Neurologis • • • Kesadaran Kepala Leher Nn Cranialis Ekstremitas:")
PHYSICAL EXAMINATION (MR) Status Neurologis • • • Kesadaran Kepala Leher Nn Cranialis Ekstremitas: Gerak : CM, GCS E 4 V 5 M 6 : pupil isokor (3 mm/3 mm), RC (+/+), RK (+/+) : meningeal sign (-), kaku kuduk (-) : PN II Kekuatan RF RP TN TR Cl B B 5/5/5 +2 +2 - - N N E E - • Sensorik • Vegetatif : dbn
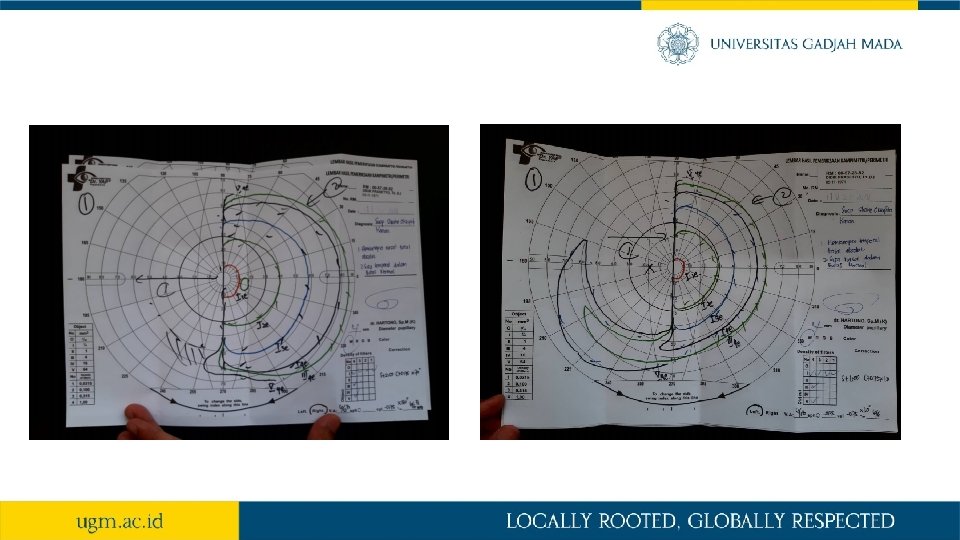

RESUME • KU baik, CM, GCS E 4 V 5 M 6 • Tanda vital : Hypertension stage I • Status generalis: dbn • Status neurologis : • Loss of visual field: • Temporal part of left eye • Nasal part of right eye • Pemeriksaan penunjang • Perimetry: • Hemianopsia temporal total absolut, sisa nasal dbn (LE) • Hemianopsia nasal total absolut, sisa temporal dbn (RE)

DIAGNOSIS • CLINICAL DIAGNOSIS: Acute loss of visual field temporal left eye and nasal right eye • TOPICAL DIAGNOSIS: Lesion of primary visual cortex lobus occipital dextra dd Tractus opticus dextra • ETIOLOGICAL DIAGNOSIS: Vascular: acute stroke non hemorrhagic lobus occipital dextra

MANAGEMENT • Emergency management of ABC support • Establish onset of symptoms and stroke assessment NIHSS • Monitoring vital sign, glucose, ECG 12 lead • Activate stroke team and consult neurologic specialist • Plan of emergency CT-scan or MRI Acute Ischemic Stroke • Planning indication of fibrinolytic rt. PA Alteplase • Aggressive monitor: BP and neurologic deterioration

DISCUSSION

Definition • Stroke: CNS infarction in brain, spinal cord, or retinal cell death attributable to ischemia defined by vascular distribution. Clinical evidence of cerebral, spinal cord, or retinal focal ischemic injury based on symptoms persisting ≥ 24 hours or until death, and other etiologies excluded. • Hemianopsia homonym: involves vision loss on the same side of the visual field in both eyes. This type of visual field loss is indicative of a lesion involving the visual pathway posterior to the chiasm.

Brain

Nervus Opticus CN II anatomy: 1. Retina 2. Optic Chiasm 3. Optic tract 4. Corpus geniculatum lateral (CGL) 5. Optic radiation 6. Cortex occipital CN II examination: 1. Visus 2. Visual field 3. Color blind 4. Fundus

Visual Pathway

Visual Field Defect

Hemianopsia Homonim

Stroke • Ischemic stroke: An episode of neurological dysfunction caused by focal cerebral, spinal, or retinal infarction. • Hemorrhagic stroke: Rapidly developing clinical signs of neurological dysfunction attributable to a focal collection of blood within the brain parenchyma or ventricular system that is not caused by trauma. • Transient ischemic attack (TIA): a brief episode of neurological dysfunction resulting from an interruption in the blood supply to the brain or the eye, sometimes as a precursor of a stroke. Assesment of risk into Ischemic stroke using ABCD 2 score.

ABCDE 2 Score The ABCD 2 score is to help predict short-term stroke risk after a transient ischemic attack (TIA). It is optimized to predict stroke risk within two days after a TIA. 2 days risk for stroke: 0 -3 low, 4 -5 moderate, 6 -7 high

Patophysiology

Patophysiology

Signs and Symptoms Sudden or acute: • numbness or weakness in the face, arm, or leg, especially on one side of the body. • confusion, trouble speaking, or difficulty understanding speech. • trouble seeing in one or both eyes. • trouble walking, dizziness, loss of balance, or lack of coordination. • severe headache with no known cause.

Diagnosis FAST: • F—Face: Ask the person to smile. Does one side of the face droop? • A—Arms: Ask the person to raise both arms. Does one arm drift downward? • S—Speech: Ask the person to repeat a simple phrase. Is the speech slurred or strange? • T—Time: activate stroke team and consult neurologic specialist.

Diagnosis

Diagnosis NIHSS score

Supporting Examination • CT Scan/ MRI Brain • CT/MR Angiografi Brain

Management

Management Iskemik • Trombolisis intravena : alteplase dosis 0. 6 -0. 9 mg/kg. BB, pada stroke iskemik onset <6 jam • Terapi endovascular : trombektomi mekanik, pada stroke iskemik dengan oklusi karotis interna atau pembuluh darah intrakranial, onset <8 jam • Manajemen hipertensi (Nicardipin, ARB, ACE-Inhibitor, Calcium Antagonist, Beta blocker, Diuretik) • Manajemen gula darah (insulin, anti diabetik oral) • Pencegahan stroke sekunder (antiplatelet : aspirin, clopidogrel, cilostazol atau antikoagulan : warfarin, dabigatran, rivaroxaban) • Neroprotektor (citicholin, piracetam, pentoxyfiline, DLBS 1033) • Perawatan di Unit Stroke • Neurorestorasi / Neurorehabilitasi
 • Manajemen")
Management Hemoragik • Koreksi koagulopati (PCC/Prothrombine Complex Concentrate, jika perdarahan karena antikoagulan) • Manajemen hipertensi (Nicardipin, ARB, ACE-Inhibitor, Calcium Antagonist, Beta blocker, Diuretik) • Manajemen gula darah (insulin, anti diabetik oral) • Pencegahan stroke hemoragik (manajemen factor risiko) • Neuroprotektor • Perawatan di Unit Stroke • Neurorestorasi / Neurorehabilitasi

References • Goodwin, D. , 2014. Homonymous hemianopia: challenges and solutions. Clinical Ophthalmology, p. 1919. • Messé, S. and Jauch, E. , 2008. Transient Ischemic Attack: Diagnostic Evaluation. Annals of Emergency Medicine, 52(2), pp. S 17 -S 26. • Stroke, 2019. Correction to: An Updated Definition of Stroke for the 21 st Century: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. 50(8). • Vilela, P. , 2017. Acute stroke differential diagnosis: Stroke mimics. European Journal of Radiology, 96, pp. 133 -144.

Terima Kasih Mohon Asupan
- Slides: 38