Reducing and Preventing Medical Errors in your Workplace





: ◦ Omitting key drugs or services as recommended by")













 2. Integration or processing of data (develop and test")

 Cognitive")


 Probability of")
 Types of error that")

 ◦ Skill")






 Self Detection probability = 11%")













- Slides: 49
Reducing and Preventing Medical Errors in your Workplace David Robinson, MD, MS MMM Professor and Vice Chair Department of Emergency Medicine University of Texas Health Science Center at Houston Mc. Govern Medical School at UTHEALTH
I have no financial relationships or affiliations to disclose I will not discuss off label use and/or investigational use in my presentation Disclosures
The aim of science is not to open the door to endless wisdom, but to put a limit on endless error. -Bertolt Brecht The life of Galileo
Define ‘quality’ and ‘error’ as it pertains to health care Identify common types of cognitive strategies responsible for medical error and, Discuss adaptive strategies to help counter these errors Promote open discussion of medical errors that maximizes learning and systems improvement Objectives
“The combined and unceasing efforts of everyone—healthcare professionals, patients and their families, researchers, payers, planners and educators—to make the changes that will lead to better patient outcomes (health), better system performance (care) and better professional development. ” Defining Quality Health Care Quality and Safety in Health Care 2007; 16: 2 -3; doi: 10. 1136/qshc. 2006. 022046
Error in Execution (Commission): ◦ Omitting key drugs or services as recommended by national guidelines ◦ Lack of Management Standards (Protocols) Error in Planning (Omission): ◦ Lack of Process (unable to provide service) ◦ Can’t provide services in a timely manner Errors Identified from Lack of Process From IOM, reported in www. ahrq. gov/qual/errback
Safe, high-quality patient care A culture of honesty, self-assessment, disclosure and trust Memorable educational and clinical experiences that help us train and nurture outstanding physicians What We Really Want
The “Physiology” Of Medical Error
Error-free performance is socialized early in medical school and residency training Most Error Reductive processes are focused on assigning blame rather than identifying root cause and educating all This culture increases the likelihood of developing maladaptive strategies for dealing with errors Historical Failure
§ 80% of errors occur as a result of multiple small system check omissions § An average of 8 sequential errors must occur to result in an AE (Swiss Cheese phenomenon) § Blaming the physician for multisystem error is similar to ‘killing the messenger’ How Adverse Events Occur
Medical Errors involve many organizational layers
Systems Influences Contribute to Significant Errors
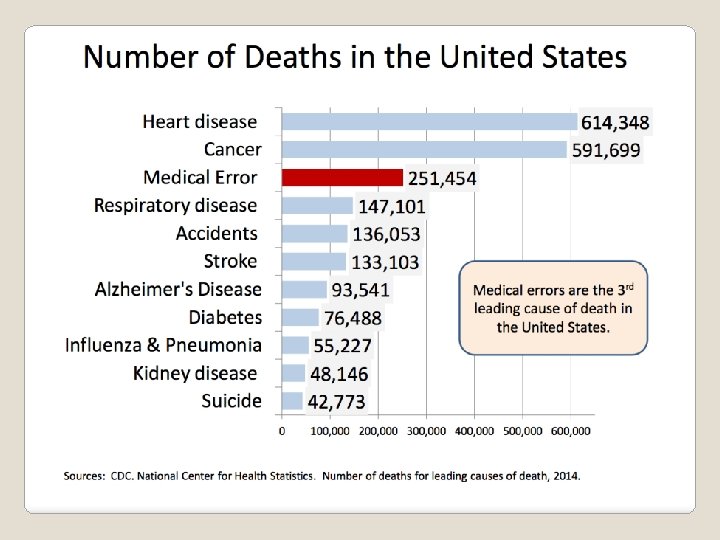
44, 000 – 98, 000 deaths in U. S. hospital each year related to medical errors 7, 000 errors deaths related to medication Errors frequently result from basic flaws in the way the health care system is organized 1999 Institute Of Medicine Report Institute of Medicine: To Err is Human: Building a Safer Health System; 1999.
“More lethal than vehicular trauma, breast cancer, or AIDS. ” “More Americans killed in hospitals every 6 months than in the Vietnam War. ” “Three fully loaded jumbo jets crashing every other day. ” The Media’s Influence on Error
• Overall rate of misdiagnosis 40% to 60% • Stable across time, hospitals, countries and areas of clinical practice • Errors with ‘significant implications’ =10% • Error rates not influenced by new technology Errors Are Common and Unchanged over last 50 years Goldberg, RM, Annals of Emergency Medicine 2002; 39: 287.
◦ Errors are defined in terms of failed processes without link to subsequent harm ◦ Few studies actually measure error ◦ No trials directly examine the relationship between error and adverse events ◦ The value of pursuing latent error has not been proven Conclusion: ‘Medical Error should be defined in terms of failed processes that are clearly linked to adverse outcomes’ The Definition of ‘Error’ is blurred, used out of context Eff Clin Prac 2000 Nov-Dec; 3(6) 261 -9
True Medical Error Represents the inner circle of a Complex Medical System www. quic. gov/summit/savitzfig 1. htm
Promote a ‘Systems’ reporting structure for Adverse Events and Medical Error Discuss AE/ME in terms of Root Cause and: Develop a systems analysis approach promoting error correction and not blame Hospital Goals for Medical Error Identification and Reporting
Review how we practice medicine Where to Begin?
Data gathering (H & P) 2. Integration or processing of data (develop and test DDX) 3. Confirmation of Diagnosis (reduce to most common diagnosis(es)) 4. Treatment 1. The Process of Medical Decisionmaking has 4 phases Goldberg, RM, Annals of Emergency Medicine 2002; 39: 287.
Cognitive tasks we use for decision-making Level Skill Based Rule Based Knowledge Based Activity Wound repair, endotracheal intubation, fracture reduction Algorithms, ACLS, decision rules, clinical practice guidelines Clinical decision making Diagnostic reasoning Croskerry P. Annals of Emergency Medicine 2003; 41: 110 -120.
Identifying Error becomes more difficult with more mentally complex tasks Procedural (skill based) Cognitive (rule based) Affective (knowledge) Visibility High Low Moderate Awareness High Low Documented Yes Rarely No Preventability High [difficult] Amenable Difficult Very Difficult Analysis
Simple ------- moderate ---- complex Skills based Rule based Knowledge based The higher the level of cognitive complexity, the more difficult it is to identify the error Summary: Level of Cognitive Complexity
Definition: Skill so familiar, we can do it ‘without thinking’ Types of Error: ◦ Slip: without intending it we do the wrong thing ◦ Lapse: without intending, we fail what we intended to do Error rate: 3/1000 acts (0. 3%) Skill-Based Errors
Each day we perform 10000 acts/day (30 skill errors / day) Probability of detecting error = 60% Prevention of Skill Based Error: ◦ *** Pause and self check*** Skill-Based Errors
Responding to a situation using a learned principle (rule /protocol) Types of error that occur: 1. Using the wrong rule 2. Misapplied a rule 3. Chose not to follow a rule Rules Based Errors
Rules Based Errors Probability of rule based error: 1/100 Type of Error Prevention Strategy Wrong Rule Educate about the Correct Rule Misapplied Rule Think again Chose not to follow rule Reduce cause of poor choice, risk awareness, coaching From medical Error review MHH, 3/07
Problem solving a new or unfamiliar situation (many acute medical encounters) ◦ Skill set not immediately applicable ◦ No apparent rule set or no rules at all We use several problem solving ◦ Heuristics - use what we know ◦ Take a guess ◦ Trial and Error strategies Knowledge-Based Errors
From Greek definition: “serving to find out and discover” Strategies that guide information search and modify problem representations to facilitate solutions Heuristics: “short cuts”
A Cognitive Process that simplifies clinical decision-making operations, describing everyday intuitive decisions that [EM] physicians make without resorting to formal decision analysis. A mental ‘short cut’ Modern Definition of Heuristics in Medicine
Pattern recognition results in faster and more efficient thinking than other cognitive analytic strategies Requires less resources Improves with experience Requires much less knowledge based mental energy Benefits of Heuristics
When employed with knowledge-based decision-making, may cause: ◦ Early closure in decision process ◦ Premature (and potentially wrong) conclusion ◦ Mistake Downside of Heuristics
• RUQ Abdominal pain and ‘fat, female, fertile, forty’: gallbladder Heuristics or Anchoring Bias? (accepting your initial impression as your final impression) has RUQ tenderness with 16 k WBC with 10 bands, cough and fever… Belief Bias? – additional feedback not received objectively or completely ignored Ultrasound + for bowel wall thickening, stones, +Mc. Burneys Confirmation Bias? (obtaining tests or strategies to further support a diagnosis and exclude others you don’t want) Error or Error recovery? (metacognition) What else can it be? • Dx: Posterior pneumonia Case Example
Wrong synthesis ◦ Arriving at the wrong conclusion because of a lack of knowledge about the process Premature Closure ◦ Not considering a broad enough ddx – resulting in an early conclusion / diagnosis Inadequate synthesis ◦ Data organization does not support diagnosis Omission ◦ Missing or important information not obtained (or is unobtainable) Common Sources of Cognitive Error Voytovich, et all. Premature Conclusions in Diagnostic Reasoning. J Med Educ. 1985; 60: 302 -307
Probability of knowledge based error is 3/10 (30%) Self Detection probability = 11% Type of Error: Mistake (not slip or lapse) Ways to prevent this error: ◦ Don’t make knowledge-based decisions alone…. . use consults ◦ Metacognitive thinking process Knowledge-Based Errors
‘Thinking about thinking’ An individual’s ability to stand apart from his or her own thinking, to observe it, and to recognize opportunities for using interventional thinking strategies A solution to cognitive error: Metacognition Croskerry P. Annals of Emergency Medicine 2003; 41: 110 -120.
The term cognitive forcing strategy describes a deliberate, conscious selection of a unique cognitive intervention, employed in a specific situation to optimize decision making and reduce the probability of error. Features Of Metacognition Croskerry P. Annals of Emergency Medicine 2003, 41: 110 -120.
Encourage Cognitive Forcing Strategies Data 1 st Impression CFS 35 y/o with migraines Drug seeking Is this a SAH? 65 y/o with back pain Lumbar strain Is this a AAA? 90 y/o with confusion Dementia Is this sepsis? 5 y/o with vomiting Gastroenterits Is this appendicitis?
Self awareness Recognition of the limitations of memory Ability to appreciate perspective Capacity for self critique Ability to select “cognitive forcing strategies” Features Of Metacognition Croskerry P. Annals of Emergency Medicine 2003, 41: 110 -120.
Errors are likely when care is transferred from one clinician to another A critical time to avoid: • Transfer of biases and/or defective cognition • Premature closure • Moralistic judgment Develop a Cognitive Transfer Approach
Before you sign the chart, ask yourself the following very simple questions… Is there another diagnosis I that I have not considered? Are my treatment decisions correct? Is my disposition decision correct? Have I passed on all the information? Apply Cognitive Forcing Strategies
Considering a System. Wide Error Free Approach New opportunities for Medical Errors Research
Patient Factors Environmental Factors • Overcrowding or Overloading • Limited ancillary services • Chaotic environment • Physical plant layout • Limited information • Inflexible information systems • Diagnostic uncertainty • Maladaptive policies / procedures • High decision density • Fatigued staff • Limited access to critical data • Multiple care transitions • Time pressure for decision making • External and Internal Influences High Cognitive Load Threats To Cognition Clinical Decision Making / Experience Of The Clinician Modern Informatics Research Increased Risk for Error Traditional EM Errors Research
First, Identify where error occurs in the hospital Develop Sound Feedback System Inspire all to want to participate in change – not forced Open dialogue about safety Develop a ‘Culture’ of Change
Fear of perceived incompetence Worry about litigation Concern about patient well being Isolation, depression… Few Systems Are in Place To Deal With The Human Consequences Of Error Understand The Perceived Consequences of Error Hevia A. Annals of Emergency Medicine 2003; 42 -565 -570.
Identify the various types of cognitive errors that occur in our practice Consider the error reductive strategies listed to counter these errors Promote a systems approach to error reporting and review Summary
Who makes more errors? Residents in training or Experienced ‘Attending’ Physicians? Attendings!. . but Experienced physicians identify and recover errors faster than less experienced providers leading to far less adverse events or bad outcomes Lesson: Teach yourself to look for errors in your practice and correct them early – we call this ‘experience’ Final Quiz Translational cognition for decision support in critical care environments: A review (Patel & Zhang 2008)
Questions?