RED FLAGS CAUDA EQUINA Stuart Fraser Physiotherapist Wessex



















 w. Disc 45% w. Tumour 29% w.")

 Interview Examination w. Bladder 74% w. Bowels")





 Majority View (51 – 74%) Category Pathology")



- Slides: 37
RED FLAGS & CAUDA EQUINA Stuart Fraser Physiotherapist Wessex Neuro Department Southampton University Hospitals NHS Trust
Background WHAT IS A RED FLAG ?
Background Patient response or finding on history taking and physical examination that are associated with a serious spinal pathology.
Background w LITERATURE SEARCH n 40 Papers Specifying Red Flags w INTERNATIONAL GUIDELINES n 8 International Guidelines
Red Flags 100% 75 – 99% 51 – 74% 0 – 50% Unanimity Consensus Majority view No consensus Source: CSP Guidelines Development Group
Guideline Findings Unanimity 100% w. Weight Loss w. Previous History of Cancer w. Systemic Steroids
Guideline Findings Consensus w. Violent trauma 75 – 99% w. Difficulty with micturition w. Reduced anal tone w. Saddle anaesthesia w. Widespread/progressive neuro
Guideline Findings Majority view w. Age <20 or > 55 51 – 74% w. Constant progressive pain w. IV drug use / HIV w. Systemically unwell w. Gait disturbance w. Structural deformity
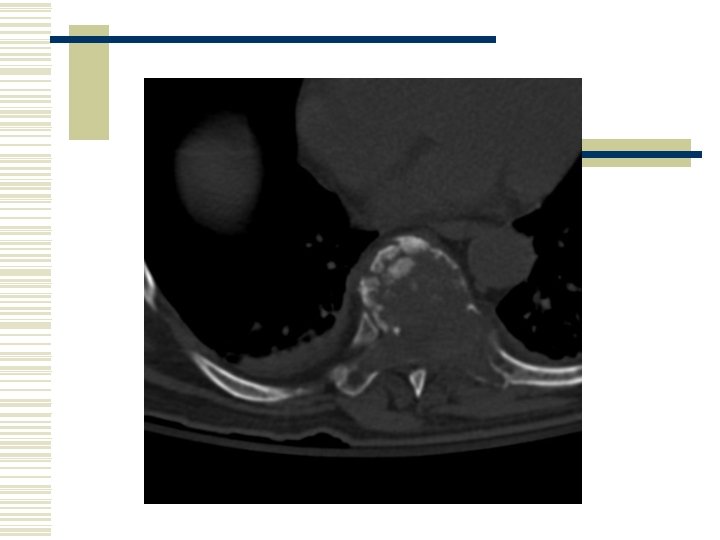
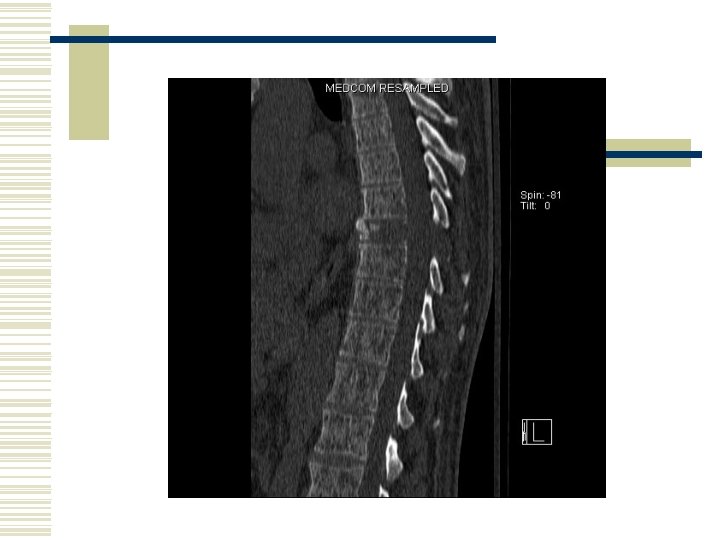
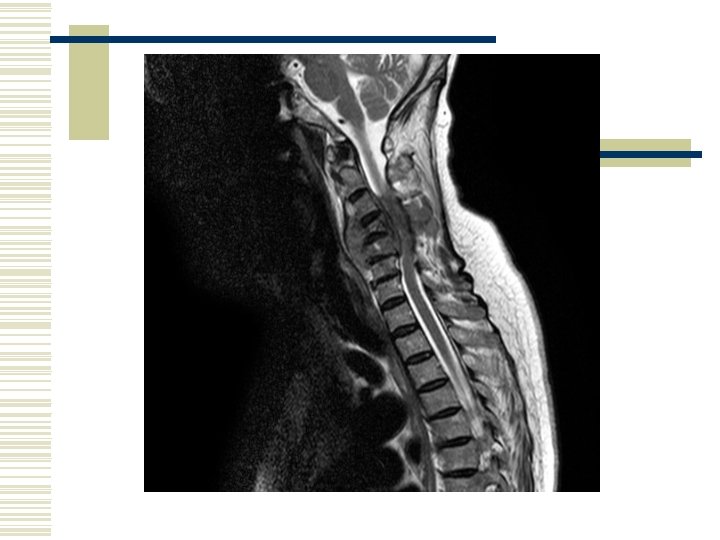
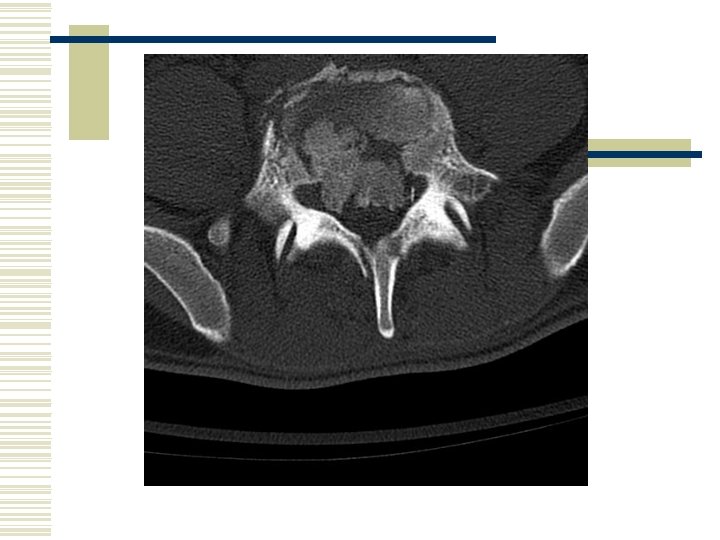
What do Red Flags Signify ? w Possible serious spinal pathology w Tumour / malignancy w Infection w Fracture
Literature Consensus 75 – 99% w. Weight loss w. Previous history of cancer
Literature Majority view w. Night pain w. Age > 50 years 51 – 74% w. Violent trauma w. Fever w. Saddle anaesthesia w. Difficulty with micturition w. IV drug abuse w. Progressive neuro w. Systemic steroids
Conclusion w Inconsistency in the literature as to what red flags signify w Inconsistency in identifying true red flags
Cauda Equina Syndrome
Cauda Equina What is Cauda equina syndrome ?
Literature 118 PAPERS REVIEWED
Definition “A complex of low back pain, bilateral sciatica, saddle anaesthesia, motor weakness in the lower extremities with bowel and bladder incontinence. (Kostuik 1986)”
Definition w General Statement w Pathomechanical w Clinical presentation
Cauda Equina 100% 75 – 99% 51 – 74% 0 – 50% Unanimity Consensus Majority view No consensus Source: CSP Guidelines Development Group
Pathology 86% No Consensus (0 – 50%) w. Disc 45% w. Tumour 29% w. Infection 28%
Pathology w 65 Pathologies identified w Metastatic w SOL w Specific - vertebral - medullary / dural - chordoma - sarcoma - chondroblastoma
Literature Findings Majority View (51 – 74%) Interview Examination w. Bladder 74% w. Bowels 57% w. Pain 57% w. Sensation 66% w. Power 53% No Consensus w. Sexual Function 13% (0 – 50%) w. Reflexes 33%
Bladder w 40 – Subcategories w Retention w Incontinence w Dysfunction 41% 36% 32%
Sensation w 42 - Subcategories w Specific Location w Non Specific 59% 17%
Bowels w 15 – Subcategories w Sphincter Tone w Dysfunction w Incontinence 34% 25% 21%
Pain w 42 – Subcategories w. Specific Location w. Nature 42% 13%
Power w 35 – Subcategories w Non Specific w Bilateral w Specific muscle / location 29% 18% 14%
Summary of Findings Consensus (75 – 99%) Majority View (51 – 74%) Category Pathology Bladder Sensation Specific Location Bowels Pain Power
Clinical implications w Acute or Chronic w Pathological process
Clinical Implications w So what can you do? w Should you change your clinical practice?
Thank You Any Questions ? Stuart. Fraser@suht. swest. nhs. uk