Rectus femoris transfer Rectus femoris muscle Origin Anterior













 •")





- Slides: 26
Rectus femoris transfer 분당서울대학교병원 이승열
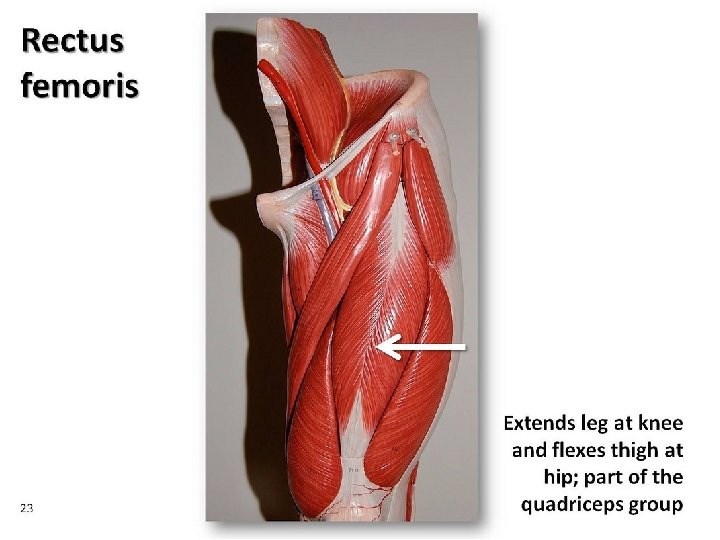
Rectus femoris muscle • Origin – Anterior Inferior Iliac Spine and Ilium above toe acetabulum
• Insertion – Quadriceps tendon to base of patella and onto tibial tuberosity via the patellar tendon • Nerve to muscle – Femoral nerve (L 2 -L 4)
Stiff knee gait
• One of m/c gait abnormality in patients with spastic CP • Typical finding – Decreased ROM of knee during swing phase • Foot clearance problem • Reduced gait velocity • Reduced step length
Rectus femoris transfer • Conventional treatment
Indication • Positive Duncan-Ely sign
• Gait analysis Decreased knee flexion in swing Decreased and delayed peak knee flexion in sweing
• Dynamic electromyography – Pathological increased activity of the rectus femoris muscle
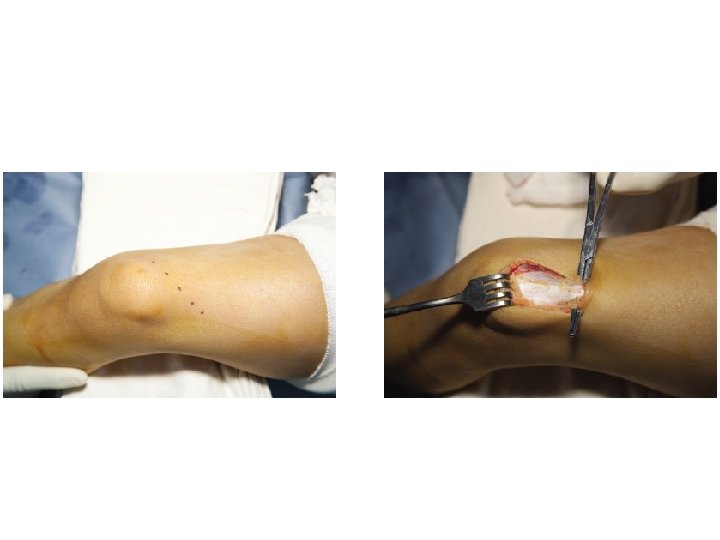
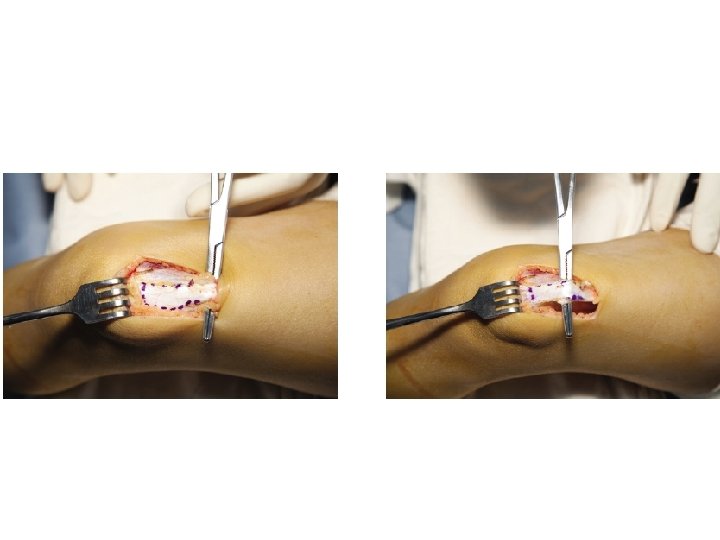
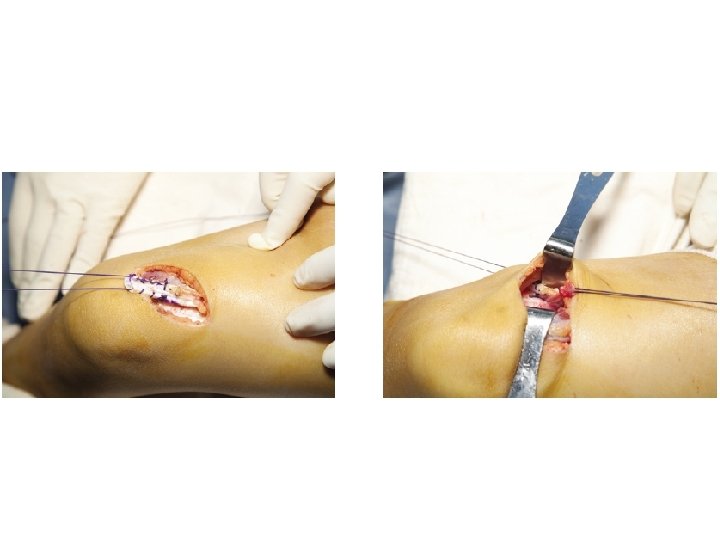
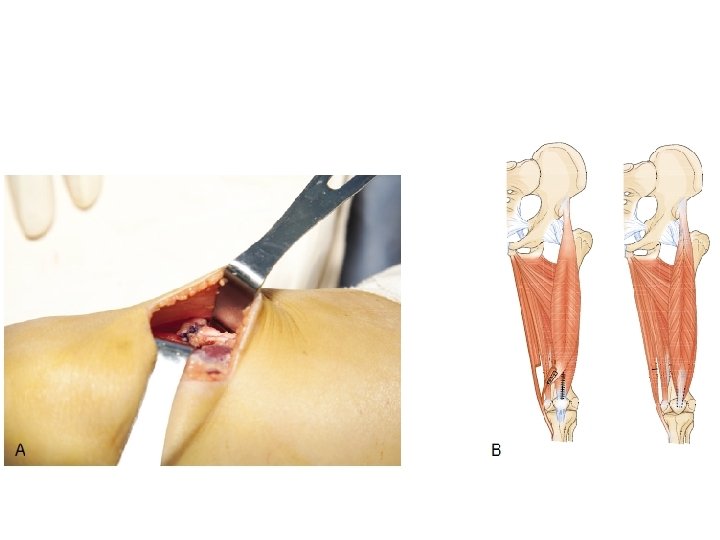
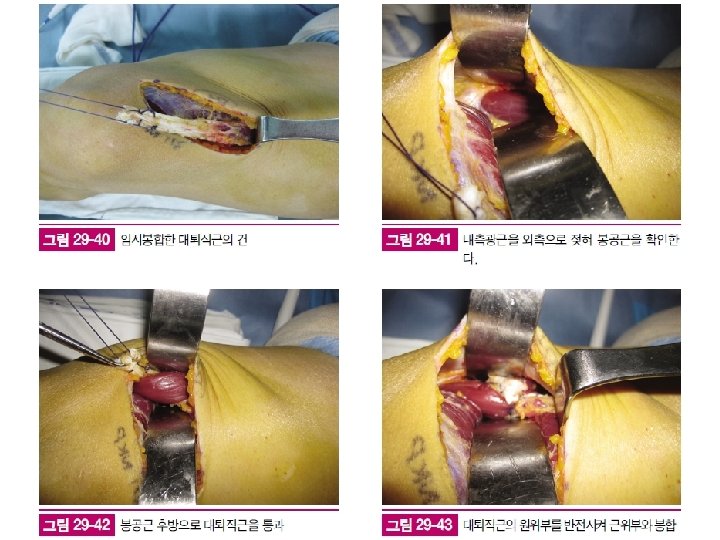
OP technique
Outcome
• Keep the rectus as a hip flexor • Convert the rectus into a knee flexor? ? ? • Elimination of the rectus femoris activity
Study plan • Patients – 321 pts • Factors affecting the results of RFT – Age – Gender – Anatomical type – Functional scale (GMFCS level) – SEMLS concomitant with RFT
• Long term results – LMM? • Gait analysis (knee sagittal motion) • GDI
MRI study 진행상황
• Isokinetic muscle strength • Isometric muscle strength
• Hip – Flexion/extension – Adduction/abduction • Knee – Flexion/extension • Ankle – Dorsiflexion/plantarflexion – Inversion/eversion
Thank you!!