Reconceptualizing Pain INSERVICE PRESENTED BY JOSH BOSTICK SPT

Reconceptualizing Pain IN-SERVICE PRESENTED BY: JOSH BOSTICK, SPT

Objectives Review the basic physiologic principles of pain Understand the key points behind the reconceptualization of pain Understand the current evidence associated with use of pain education for patients with musculoskeletal disorders in the clinical setting Understand how pain education can be implemented in the clinical setting for patients with musculoskeletal disorders

What is pain? Definition: an unpleasant sensory and emotional experience Noxious stimulus: stimulus of sufficient magnitude to potentially damage tissue Various types: Mechanical, Thermal, Chemical, Polymodal Nociceptors: high-threshold free nerve endings Various types: cutaneous, joints, muscles, periosteum, visceral organs Neuropathic Pain: pain related to changes in nervous system, not noxious stimuli

Pain Pathway Spinothalamic tract: pain, temperature, crude touch Most prominent tract Terminates in thalamus Somatotopic Organization Facial Pain Spinal trigeminal tract Trigeminothalamic tract http: //nobaproject. com/images/shared/images/000/213/original. png

Gate Control Theory Ascending signals from nociceptors are mediated by inhibitory interneurons Pain becomes unmodulated when inhibition of the inhibitory interneuron occurs Can reactivate inhibitory interneurons through increased input of other sensory systems i. e. rubbing your elbow after hitting it against a wall Noxious stimulus can also be inhibited at level of spinal cord via endogenous analgesic system Release of endorphins that affect neurochemistry https: //t 3. ftcdn. net/jpg/00/87/44/32/240_F_87443289_ITp 8 g. Xjw. Ylv. U 79 bp. R 0 n 3 yw. QG 5 jl 1 A 5 AJ. jpg

http: //embed. wistia. com/deliveries/07 c 5 e 6165990 f 9 b 055368 f 068 f 25 f 38 aa 3 e 53979. jpg

Neuromatrix Theory of Pain is a result of interactions between multiple aspects of the nervous system Includes cognitive, motivational, and sensory inputs

“Reconceptualizing Pain According to Modern Pain Science” Published in 2007 by G. Lorimer Moseley Presents that pain is not a simple biological process and introduces four main points that help define pain and clinical implications of treating pain

Four Key Points “Pain does not provide a measure of the state of the tissue” “Pain is modulated by many factors across somatic, psychological, and social domains” “The relationship between pain and the state of tissues becomes less predictable as pain persists” “Pain can be conceptualized as a conscious correlate of the implicit perception that tissue is in danger”

“Pain does not provide a measure of the state of the tissue” Gate control theory Pain is a result of noxious stimulus and not a representation of the state of the tissue Various studies suggest that nociceptors have varying responses to stimuli which may make subjective ratings inaccurate Small fibers may respond to non-painful changes of internal body state Some fibers are “high-threshold” and may not respond to small changes Research not conclusive

“Pain is modulated by many factors across somatic, psychological, and social domains” History of anecdotal evidence that pain is modulated by various domains i. e. stories associated with sports injuries Other biological factors that modulate pain Inflammatory mediators (increased nociceptor activity) Tissue temperature (increase temp = increase nociceptor activity) Blood flow (decrease flow = increase nociceptor activity) Attention can factor into perception of pain (i. e. attention amplifies pain) Expectations affect perception (i. e. cues associated with pain) Cognitive states can affect pain (i. e. catastrophizing pain) Anxiety can amplify pain

“Pain is modulated by many factors across somatic, psychological, and social domains”

“The relationship between pain and the state of tissues becomes less predictable as pain persists” Sensitization Nociceptors can become more sensitive and responsive as the pain persists Lower action potential threshold, spontaneous firing Hyperalgesia (exaggeration of painful stimuli) Allodynia (non-painful stimuli become painful) Reorganization of primary sensory cortex Chronic pain cause inaccurate body mapping which can lead to altered motor control and disrupt motor planning

“Pain can be conceptualized as a conscious correlate of the implicit perception that tissue is in danger” Neuromatrix Theory Pain is just one output that occurs when body perceives a threat Pain depends on the perception of the threat in terms of severity and degree Implication is to consider how different factors can affect perception of pain Pain may not be representative of tissue damage Consider that pain may be more of a result of a factor that is not directly affected with traditional treatment

Clinical Implications Consider that pain may be result of something other than physical damage The patient’s perception of pain should be assessed and treated in addition to physical impairments May be conflict between nature of therapy and patient’s perception of threat in regards to pain Patient education Alter perception of pain Understand that pain may be coming from factors other than tissue health

“The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature” Includes 13 RCT Evaluating the effect of pain neuroscience education (PNE) on pain, function, disability, psychosocial factors, movement, and healthcare utilization in those with chronic musculoskeletal (MSK) pain Inclusion Criteria English language 1999 -2015 Subjects Age >18 MSK Pain RCT

“The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature” Quality Assessment Level of evidence based on National Health and Medical Research Council Hierarchy of Medicine Methodology assessed using PEDro scale All included studies scored 6/10 or higher Demographics 398/734 qualified subjects received PNE 70% female Mean age: 41. 7 MSK Conditions: low back pain, chronic fatigue syndrome, fibromyalgia, lumbar radiculopathy, chronic neck pain

“The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature” Treatment parameters Longest duration: 4 hours Shortest duration: 30 minutes Range from 1 session per treatment to multiple sessions Primary format: one-on-one between provider and patient One study only included informational booklet

“The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature” Adjunct Treatment Mobilization & manipulation Soft tissue massage Muscle & neural mobilization Trunk stabilization Circuit-based aerobic exercise Movement exercises Trigger point dry needling Neck stabilization exercises Aquatic exercise program

“The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature” Outcomes

“The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature” Conclusion There is evidence to support the use of PNE as treatment for patients with MSK disorders to help reduce pain levels, disability, fear avoidance behavior, limited movement, healthcare utilization, behaviors related to pain, and catastrophizing Limitations Results were compiled in narrative format due to heterogeneity of RCT outcome measures 13 studies PNE was just one of many treatments utilized to treat patients PNE not universally defined with specific parameters

“How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines” Aims to provide guidelines for the use of pain physiology education in patients with chronic musculoskeletal disorders
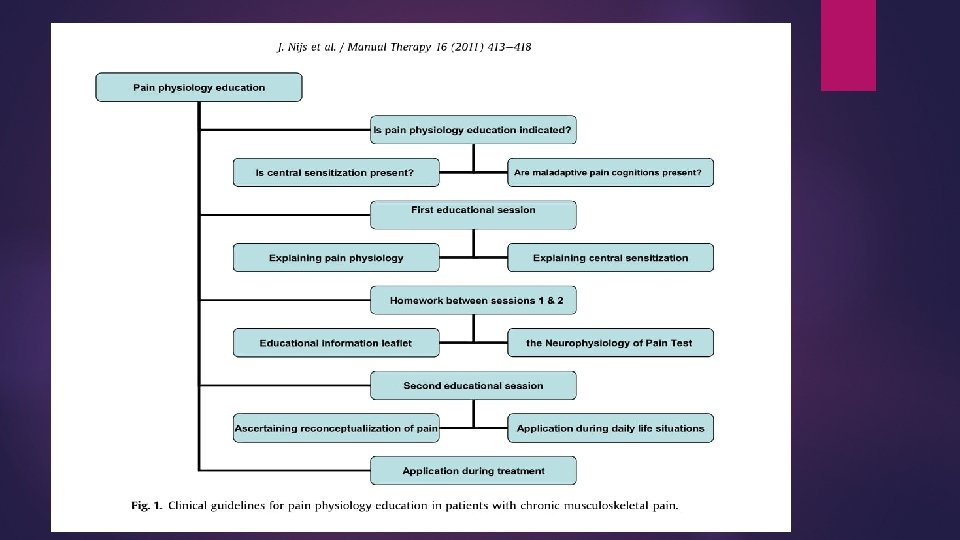

“How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines” Determining eligibility “The clinical picture is characterized and dominated by central sensitization” May not be present in acute phase but possibility of presentation in later stages “Maladaptive pain cognitions, illness perceptions or coping strategies are present” Ask about perception of cause of pain, consequences, and effectiveness of treatment Maladaptive cognitions include ruminating about pain, hypervigilance to somatic signs (can use Pain Catastrophizing Scale or other analog

“How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines” First Educational Session Explain rationale for treatment Explain basic concept of central sensitization Reconceptualize Pain Relationship between pain and cognition/behavior Recommended 1 -2 face-to-face sessions of approximately 30 minutes each Use of educational book “Explain Pain” – Butler & Moseley Describe nature of pain and how acute can become chronic

“How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines” Second session Neurophysiology of Pain Test: identifies what topics need further explanation Insight about somatic, psychosocial, and behavioral factors associated with sensitization that are specific to patient Explain how information can be applied to daily life Discuss patient’s motivation to use information

“How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines” Conclusion The explained guidelines for pain physiology education can be beneficial in treating patients with chronic musculoskeletal disorders Limitations Guidelines were based on existing research and were not explicitly tested by authors Only considers diagnosis and not patient demographics Educational sessions will probably not fit into treatment times used in clinical practice Does not detail treatment used in addition to education

Summary There is a growing base of evidence for reconceptualizing pain and using education in addition to traditional treatment options to improve patient outcomes Evidence is still relatively new and may not be strong enough for immediate integration into clinical practice Understanding that pain may not always be directly related to musculoskeletal health may open new paths to treat chronic pain

References Fitzakerley, Janet. "2014 Somatosensation. " Gate Theory. University of Minnesota Medical School Duluth, 10 Feb. 2015. Web. 02 July 2017. Louw, Adriaan, Kory Zimney, Emilio J. Puentedura, and Ina Diener. "The Efficacy of Pain Neuroscience Education on Musculoskeletal Pain: A Systematic Review of the Literature. " Physiotherapy Theory and Practice 32. 5 (2016): 332 -55. Web. Melzack, Ronald. "Pain and the Neuromatrix in the Brain. " Journal of Dental Education 65. 12 (2001): n. pag. Web. Moseley, Lorimer. "Reconceptualizing Pain According to Modern Pain Science. " Physical Therapy Reviews 12 (2007): 169 -78. Web. Nijs, Jo, C. Paul Van Wilgen, Jessica Van Oosterwijck, Miriam Van Ittersum, and Mira Meeus. "How to Explain Central Sensitization to Patients with “unexplained” Chronic Musculoskeletal Pain: Practice Guidelines. " Manual Therapy 16. 5 (2011): 413 -18. Web.
- Slides: 29