Recognising the Deteriorating Patient Antoinette Broad Oxford Health

Recognising the Deteriorating Patient Antoinette Broad Oxford Health NHS Foundation Trust

Objectives • Recognise that patients have complex health care needs this is especially pertinent among care home residents • Discuss some common causes for deterioration and becoming acutely unwell including COVID-19 • Recognise the importance of early warning tools in calculating the risk of deterioration (Nursing beds) • Recognition of the signs of deterioration and when to escalate • Explain where to seek appropriate support from and how to communicate effectively when escalating concerns

Common presentations • Falls / worsening mobility • Increased confusion – ‘Delirium’ • Short of breath • High Temperature/fever • More Agitated • Apathy, new fatigue, exhaustion • Oedema / swelling typically lower legs • Chest pain

What could be wrong ? • • • • Dehydration Obvious Infection: chest, urine, skin Infection that is not obvious Stroke Drug side effects Syncope – falling blood pressure Seizures / fits Depression Malnourishment/weight loss Malignancy / cancers Undiagnosed neurological disease Low blood sugar – ‘hypos’ Undiagnosed fracture (spine, pelvis) COVID-19
 either or")
COVID-19 signs and symptoms (Remember might not be typical in older people) either or both: • a high temperature. 37. 8 C – this means they feel hot to touch on their chest or back (If you can use a thermometer – even better) • a new, continuous cough – this means coughing a lot for more than an hour, or 3 or more coughing episodes in 24 hours (if you usually have a cough, it may be worse than usual) Remember: Not everyone with a fever has Covid-19 Not everyone with breathlessness has Covid-19

• Incubation period of 3 -10 days, probably most commonly 5 days • Patients infectious for 2 -3 (up to 5 days) prior to symptoms and then for 7 days from onset symptoms. • Persistent Cough is most common first symptoms, then fever; headache, anorexia, sweats, muscle aches and exhaustion common symptoms. • Diarrhoea may occur in about 10%. • Both Hypo- and Hyperactive delirium is seen.

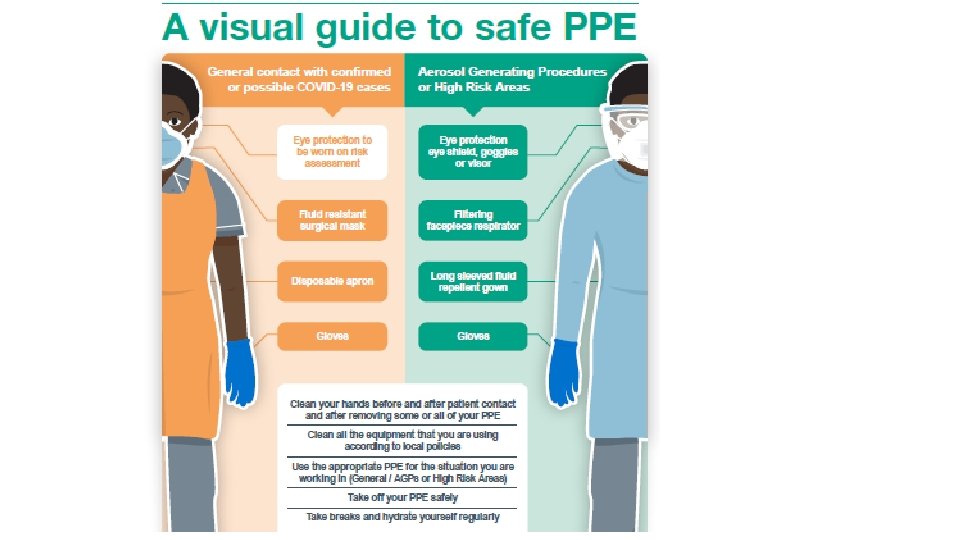
• Cough typically is dry, but some will have sputum, especially if secondary bacterial infection. • 80% will recover in a week, other than persistent post-viral cough, (& not considered infectious from day 8). • Fever &/or flu like symptoms persisting more than 7 days. • People can become suddenly very unwell days 7 -9 from onset of disease. • PPE

Recognising Deterioration • Easy as ………………. . Airway Breathing Circulation Disability Exposure

Questions to ask • AIRWAY Is the patient talking? • BREATHING Does the patient look comfortable? Are they struggling to breath? Is their respiratory rate increasing/decreasing? Do they have blue lips? Are they making any additional sounds? • CIRCULATION Do they look pale? Do they look sweaty and clammy? Do they have chest pain? Do they feel dizzy? Can they feel their heart beating strongly?

Questions to ask • DISABILITY Are they alert, or drowsy? Do you need to speak to them before they will open their eyes? Are they confused (or more confused)? Are they agitated or restless? Has their posture changed or are their limbs weak? • EXPOSURE Are they bleeding? Can you see a rash? Are there any injuries? Are they hot or cold to the touch?
 • Respiratory rate • Oxygen saturation • Systolic blood pressure")
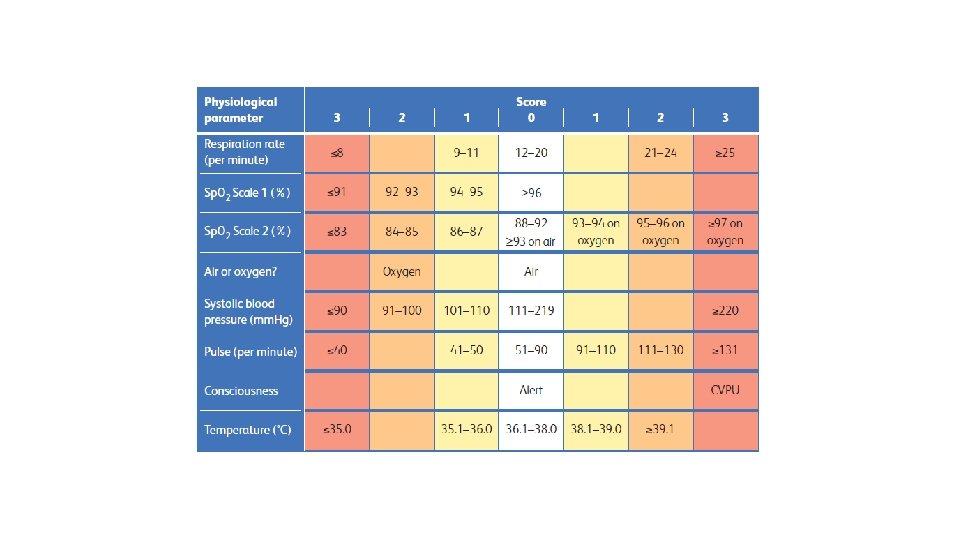
Vital signs (NEWS 2) • Respiratory rate • Oxygen saturation • Systolic blood pressure • Pulse • Consciousness or new confusion • Temperature

Who should assess for deterioration • Care Staff • Nurses • Family members • Doctors • Anyone who performs observations/reviews patients YOU know your residents best!

Chain of survival Early Recognition Effective Communication Early Treatment Improved outcome

Barriers to communication What are these? How do you overcome them?

Communication tools SBARD – well established, structured method for communicating information that requires immediate attention and action Why?
 a (role) with (organisation). I am calling about (resident")
S Situation: I am (name) a (role) with (organisation). I am calling about (resident name) because I am concerned that they are unwell (e. g. they have difficulty breathing, chest pain). B Background: I am involved with resident (X) because (reason). Their medical history is (if known). Their condition in the last (X) mins/hours. A Assessment: On assessment, report findings e. g. they feel really hot, their blood sugar is 5 mmol, their respiration rate is 20, pulse is 90, oxygen saturations are 90%” R Recommendation: Can I have some advice from you about what to do next? D Decision: So we have agreed that I will or that you will……

Who to escalate to/help available • GP, in hours and Out of Hours • CHSS They in turn can request help from • Hospital at home • Community nurses/therapists/AHP • AAU/EMU

Technology • Phone • i. Pad • Skype • Zoom GDPR guidance has been reviewed during COVID-19 https: //edpb. europa. eu/sites/edpb/files/news/edpb_sta tement_2020_processingpersonaldataandcovid-19_en. pdf

Proactive care planning • Discuss how COVID-19 may cause residents to become critically unwell. Make a clear decision about whether hospital admission would be considered • These discussions should also include plans for other serious health problems (for example, if they had a head injury; or a stroke; or chest pain)

COVID-19 and deteriorating … Admission to Hospital now? Take into account the patients advanced care plan &: • the severity of pneumonia, or signs of other severe illness • the benefits of hospital admission (access to tests, oxygen, critical care if it is appropriate) • the risks and disadvantages (catching or spreading covid; no visitors; distress due to unfamiliar surroundings and staff) • the care that may be offered in hospital compared with what can be delivered in the home • Whether it is thought that the patient may not recover this time despite everything that hospital can offer. • the patient's wishes now • What other local NHS resources could be used (H@H? )

Covid-19 Care in the Home For residents with Mild disease: Isolate them for 7 days minimum Paracetamol for fever Keep them well hydrated. Use PPE correctly. Use good Infection Control Measures (e. g. double bagging waste)

Additional Health Interventions Medication Review by a Prescriber If someone is not eating or drinking much, or if they are vomiting, ask GP to review the drugs. They may decide to stop: • water tablets, • blood pressure pills or • metformin at this time. Sometimes switching antibiotics from tablets to suspension will make it easier for the resident to swallow them.

Additional Health Interventions Drip Treatments From time to time it may be appropriate for someone to have • fluids, • antibiotics or • other medications via a drip at home to see if it helps improve the situation. This is usually for a trial period of up to 3 days max and the GP can refer to the right team to do this.

Recovery after COVID-19 Is Variable! Many people have a mild illness for a week. But: Dry Cough may persist 3 weeks Great fatigue can persist 10 -14 days Delirium can last many weeks. Deconditioning comes through lack of exercise

Impact of isolation • Anxiety • Agitation • Loss • Loneliness • Depression

COVID-19 • Escalation decisions to hospital will be taken in discussion with paramedics, general practitioners and other healthcare support staff • Transfer to hospital may not be offered if it is not likely to benefit the resident and if additional supportive or palliative care within the home is deemed more appropriate

Additional Health Interventions Good Palliative Care The harms and benefits of drip treatments must be considered carefully and they should not be used in place of good palliative care.

Covid 19 Symptom management Mary Walding Katharine House Hospice Jane Stickland Sobell House Hospice

World Health Organisation definition: What is palliative care? Palliative care is an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.

We need to treat everyone as individuals – in life and death

Dying with Covid 19 • May be quicker than usual deaths • You may be coping with several at once BUT The aim is still for the best possible death for that individual

What is the best possible death?

A “best possible” death • Recognising that it is happening • Providing comfort – physical, reassurance (psychological/spiritual) and family • Ensuring the family are involved • Staff support
")
Comfort measures for cough • Fluids • Honey and lemon • Sweets (hard boiled) • Sit upright • Discourage smoking
 • Reduce")
Comfort measures for breathlessness • Positioning • Cool air (fans not recommended) • Reduce room temperature • Distraction • Cool face using a wet flannel

Comfort measures for high temperature • Loose clothing • Cool room • Cold flannel

Comfort measures for agitation • Calm environment • Keep light on • Reassure • Known people around

Comfort measures for pain • Repositioning • Reassurance • Distraction

Medications you may be able to give as carers

Paracetamol will reduce temperature and relieve pain. It may relieve any agitation related to this so is worth giving if your resident is able to swallow.

Oramorph - liquid morphine. Make sure the patient can swallow and they are sitting up enough to do so. Measure using an oral syringe (NB check amount to be measured) and squeeze gently into the side of the mouth, not directly down the throat. Will help breathlessness, cough and pain

Lorazepam Relieves anxiety and can be given for breathlessness or panic/distress. Usually half a tablet under the tongue – it will dissolve.

Haloperidol Tablets for agitation if the patient is able to swallow

Hyoscine patches For chestiness – 5 -6 hour delay in effect so will not help immediately. It can make some people more agitated

In addition, nursing staff will be able to give prescribed sub- cutaneous medication

Verification of Death for Non Medical Health Care Professionals during COVID 19 Kathy Clarke Oxford Health Foundation Trust

Objective To provide information and guidance to promote confidence and competence to verify death looking at the following issues • Last days of life - communicating and anticipating death and supporting family • Who can verify a death? • Difference between Verification and Certification • How to verify death • Vo. D form • Contacting Funeral director and GP. Community Health Oxfordshire
 are in place and")
Last days of life • DNACPR, ACPS (Advanced Care Plans) are in place and communicated appropriately • Support for relatives family visiting restrictions and risk assessment prior to death • Consider cultural and spiritual needs and manage expectations – guidance on intranet Burial or cremation+ • Property – rings Sentimental mementos and infection control advice Community Health Oxfordshire

Legal background • “There is no legal requirement for the medical practitioner to attend to verify that death has occurred, only to issue a death certificate stating the cause of death” (BMA 1999)

Who can verify a death during COVID 19: During COVID 19 Care workers are able to verify a death : • If an agreed local pathway and training to support • Can access remote support if they don’t feel competent from a GP or nurse via IT video link • GP is informed and VOD form is emailed to them • In suspicious circumstances, there is a responsibility to contact the police and leave the body and room as it is.

Verification and Certification • Verification is confirming that someone is dead. • Verification of death differs from certification of death, which is signing a Medical Certificate of Cause of Death (MCCD), commonly referred to as Death Certificate; this can only be done by a medical practitioner. During COVID-19 the process of certification by a medical practitioner has changed; • Any doctor may complete a Death Certificate/ MCCD so long as they are able to give a cause of death to the best of their knowledge • Relaxation of the 14 -day requirement so that the deceased need only be seen by any doctor (not just the certifying doctor) in the preceding 28 days • If a doctor has seen the patient in the preceding 28 days by video link, the patient is considered to have been “seen” as if they had been seen face to face Ref. Coronavirus Bill: Managing the deceased

Determining death for verification • Position patient for examination and verification of death Steps to be followed in order Step 1 Ensure you are wearing PPE Gloves apron and mask. Establish patient is in a collapsed state with no signs of life for period of 15 minutes or more before preceding to step 2. place mask or cloth over the mouth of the deceased Step 2 No palpable carotid or femoral pulses for one minute Step 3 No cardiac sounds (listen with a stethoscope for one minute) Step 4 No signs of spontaneous respiration by observation over the 5 minutes v Step 5 Absence of pupillary responses to light Step 6 No response to trapezius squeeze (shoulder)

Verification of death form -
 •")
Guidance for care of the deceased with suspected or confirmed coronavirus (COVID 19) • Place a cloth or mask over the mouth • Respect patients spiritual and cultural wishes where possible - Expectations may need to be managed • Remove syringe pump if able or seek advice - Keep safe for return to DN base • Other devices remain (catheters, stoma bags etc)- advise funeral director if pacemaker ICD in place • No requirement to wash or lay out the deceased as funeral directors will respectfully care for the deceased once at the mortuary • Once death is verified, contact funeral directors to transfer the deceased to a mortuary Community Health Oxfordshire

Communication • Take a photograph of the VOD form for records and send to the GP via email • Once death is verified, the deceased will be collected by the funeral directors and transferred to a mortuary For family information: • The medical practitioner will email the death certificate to the Registry office • The registry office will contact the NOK or designated other by telephone to complete the Registration of Death • The registration of death will then be forwarded to the Funeral Directors to allow burial or cremation to proceed Community Health Oxfordshire

https: //www. gov. uk/government/publications/covid-19 -guidance -for-care-of-the-deceased/guidance-for-care-of-the-deceasedwith-suspected-or-confirmed-coronavirus-covid-19 https: //www. bma. org. uk/media/2324/bma-verification-of-deathvod-april-2020. pdf Community Health Oxfordshire

Support You are important

All cope differently – what works for individuals Talking Take your breaks Ask when unsure

Colleagues GP Who you can ask for advice? DN Care Home Support Team Palliative care team

24 hour Covid 19 end of life resource line Can ring at any time – 0300 561 1900.

E-Learning for Healthcare Learning resources https: //www. e-lfh. org. uk/programmes/coronavirus/ You do not need to log in, but if you want your learning recorded so you can demonstrate in appraisal/revalidation, then you will need to do so

Breaking bad news over the phone • Prepare for the conversation before making the call • Be honest and sensitive during the conversation • Document what you have said and the recipient’s reaction

If you are upset who can you turn to? Afterwards • Colleagues • Managers • Care Home Support Team, • Palliative care team • National support line - 0300 131 7000

Staff Testing : Staff who are presenting with Covid 19 symptoms can access testing for themselves by contacting Ouh-tr. covid@nhs. net if the staff member does not have an email address please call 01865 222890. Outbreak: If the home has any residents who present with Covid Symptoms advise them to call Public Health England Health Protection Team for guidance and to arrange testing: 0344 225 3861 option” Thames Valley”. Anticipatory medication: If the home has a case of COVID-19 or if a residents condition deteriorates for any reason please contact the GP and request anticipatory medication. EMU: Link with our colleagues RACU, AAU, EMU, hospital at home for treatment/advice. Staffing issues and Emergency PPE: If they report staffing issues advise them to contact our local Authority: email asccovid 19@oxfordshire. gov. uk Safeguarding: Refer through normal routes. https: //www. osab. co. uk/public/reporting -concerns
- Slides: 66