Reciprocal chromosome translocations the basics a tutorial to

Reciprocal chromosome translocations: the basics a tutorial to show chromosomes which have been rearranged as a result of a reciprocal translocation can segregate, and the clinical consequences Professor P Farndon, Clinical Genetics Unit, Birmingham Women’s Hospital 13. 11. 06

Chromosomal Translocations A translocation is formed when there has been transfer of material between chromosomes, requiring breakage of both chromosomes, with repair in an abnormal arrangement. If the exchange results in no loss or gain of DNA (ie genes), the individual is clinically normal and is said to have a balanced translocation. A balanced translocation carrier is, however, at risk of producing chromosomally unbalanced gametes. There are two types of translocation: reciprocal and centric fusion (Robertsonian)

A reciprocal translocation usually involves breakage of two non-homologous chromosomes (ie one chromosome from each of two different pairs) with exchange of the fragments. All chromosomes can take part in reciprocal translocations, which are usually unique to a particular family. The incidence of reciprocal translocations in the general population is about 1 in 500. A separate tutorial considers Robertsonian translocations.

Reminder: chromosomes, genes and heredity FZD 2 AKAP 10 ITGB 4 KRTHA 8 WD 1 SOST • A chromosome is made of DNA (and histones) MPP 3 MLLT 6 STAT 3 BRCA 1 GFAP NRXN 4 NSF • Each chromosome contains its own set of genes in a linear order • There are two copies of each autosomal gene: one on each homologue NGFR Chromosome 17 CACNB 1 HOXB 9 HTLVR ABCA 5 CDC 6 ITGB 3

How do the unbalanced forms of a translocation cause clinical problems? • By altering the amounts of products of the genes involved • Three copies of genes (partial trisomy for a particular chromosome arm) = 1. 5 times normal amount • One copy of genes (partial monosomy for a particular chromosome arm due to deletion of this area) = 0. 5 times normal amount • Altered amounts may cause anomalies directly or may alter the balance of genes acting in a pathway

The pedigree which follows shows the typical pedigree features associated with a reciprocal translocation. What are they?
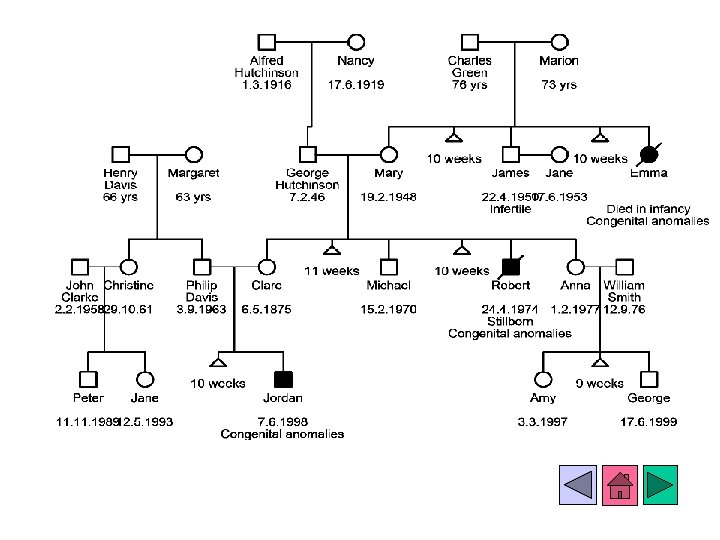

Multiple miscarriages Three children with congenital abnormalities in three generations

Reciprocal translocation Testing Clare Davis showed that she was a carrier of a balanced reciprocal chromosome translocation between the short arm of one chromosome number 7 and the long arm of one chromosome number 13.

Reciprocal translocation The parts of the chromosome arms distal to the breaks have exchanged places, resulting in a chromosome 7 missing part of its short arm but containing part of the long arm of chromosome 13. In a reciprocal translocation, the total chromosome number remains at 46. The chromosome 13 involved in the translocation has lost part of its long arm which now contains part of the short arm of chromosome 7.

In the example which follows, we are using a different translocation - to stress that for reciprocal translocations the breakpoints are different from family to family. . The translocation is between the long arm of one chromosome number 2 (grey) and the short arm of one chromosome number 11 (pink)

Balanced reciprocal translocation carrier Two of these four chromosomes are usually passed into individual gametes at meiosis. The four chromosomes can be passed on (segregate) in several different combinations.

Balanced reciprocal translocation carrier Gametes Gamete with normal chromosomes Zygote For example, the normal chromosome 2 and the normal chromosome 11 can segregate into a gamete When fertilised by a normal gamete, the resultant zygote will have a normal karyotype, and cannot pass the translocation on to future generations.

Balanced reciprocal translocation carrier The translocated chromosome 2 Gametes and the translocated chromosome 11 can segregate into a gamete Zygote Gamete with normal chromosomes When fertilised by a normal gamete, the resultant zygote will have the correct number of genes from chromosomes 2 and 11, and will be a translocation carrier.

Note that as there has been no gain nor loss of chromosomal material, this is a called a “balanced rearrangement”, and the person who has this pattern is a “translocation carrier”. Being a balanced reciprocal translocation carrier will have no effects on the health of this person. He or she, of course, can pass on various combinations of the normal and translocated chromosomes to children.

Balanced reciprocal translocation carrier Gametes Zygote The normal chromosome 2 and the translocated chromosome 11 can segregate into a gamete When fertilised by a normal gamete, the zygote will have three copies of genes from the long arm of chromosome 2 and only one copy of genes from the short arm of chromosome 11. This is trisomy for part of chromosome 2 and monosomy for part of chromosome 11. Gamete with normal chromosomes

Balanced reciprocal translocation carrier Gametes The translocated chromosome 2 and the normal chromosome 11 can segregate into a gamete Gamete with normal chromosomes Zygote When fertilised by a normal gamete, the zygote will have only one copy of genes from the long arm of chromosome 2 and three copies of genes from the short arm of chromosome 11. This is monosomy for part of chromosome 2 and trisomy for part of chromosome 11.

A carrier of a balanced reciprocal translocation can therefore produce unbalanced gametes, resulting in zygotes with partial trisomy and/or partial monosomy for the defined chromosomal regions. This chromosome imbalance may result in abortion, stillbirth, malformation and/or mental retardation. The precise effects will depend on the particular genes in the areas involved in the translocation.

Summary of outcomes Normal no risk to children Normal - but risk to children of having unbalanced translocation Balanced reciprocal translocation carrier Miscarriage, congenital malformation, developmental delay, mental abnormality

The relative frequency of each possible gamete is not readily predicted, because the size and position of the chromosome segments involved in the translocation may have an effect on the pairing of the chromosomes at meiosis, perhaps making some segregant patterns (including some unbalanced segregants not shown here) more likely in the gametes than others. The risk of having a liveborn child with each of the possible outcomes therefore depends on its frequency in the gametes and on the likelihood of the conceptus with that abnormality developing to term. These depend on the effects of the genes on the translocated segments and the amount of chromosome imbalance.

Most families with reciprocal translocations undertake fetal karyotyping (by chorionic villus sampling at about 10 weeks or amniocentesis at 16 weeks in pregnancy) to confirm that the baby has either the normal pattern of chromosomes, or the balanced form.

How does a reciprocal translocation occur in the first place? The majority of reciprocal translocation carriers have inherited the balanced translocation chromosomes from a parent. Occasionally, however, the parents have normal karyotypes. The translocation in the offspring must have arisen de novo during the meiosis which produced the egg or sperm which formed the person with the translocation. Reciprocal translocations probably occur because of mispairing of non-homologous chromosomes at meiosis, with subsequent transfer of material from one non-homologous chromosome to another. Once the translocation chromosomes have been formed they can be passed on to offspring, and future generations.

7 13 To form this reciprocal translocation between the short arm of one chromosome number 7 and the long arm of one chromosome number 13 breaks must have occurred in each arm during one meiosis in an ancestor, probably due to mispairing

Summary: Reciprocal chromosome translocation • Exchange of chromosomal material between two chromosomes • Individual clinically normal if no gain or loss of material (translocation carrier) • Unbalanced products may cause chromosomally abnormal baby, miscarriage, stillbirth, infertility • Other family members should be offered testing for carrier status

The end! • Thank you for completing this revision aid • We are interested in your comments about this aid. Please email Professor Farndon. (p. a. farndon@bham. ac. uk) © P Farndon 2003
- Slides: 25