RECEPTORTONUS NIMMO TECHNIQUE RAY NIMMO DC PALMER 1931















- Slides: 20
RECEPTOR-TONUS NIMMO TECHNIQUE
RAY NIMMO DC PALMER 1931
EARLY DEVELOPERS • Hans Krus: 1938: Treated Bonnie. Pruden for neck pain during mountain climb • Bonnie Pruden 1976: Manual therapy using elbows, thumbs, knuckles • Janet Travell !942” Spray and Stretch, Injections
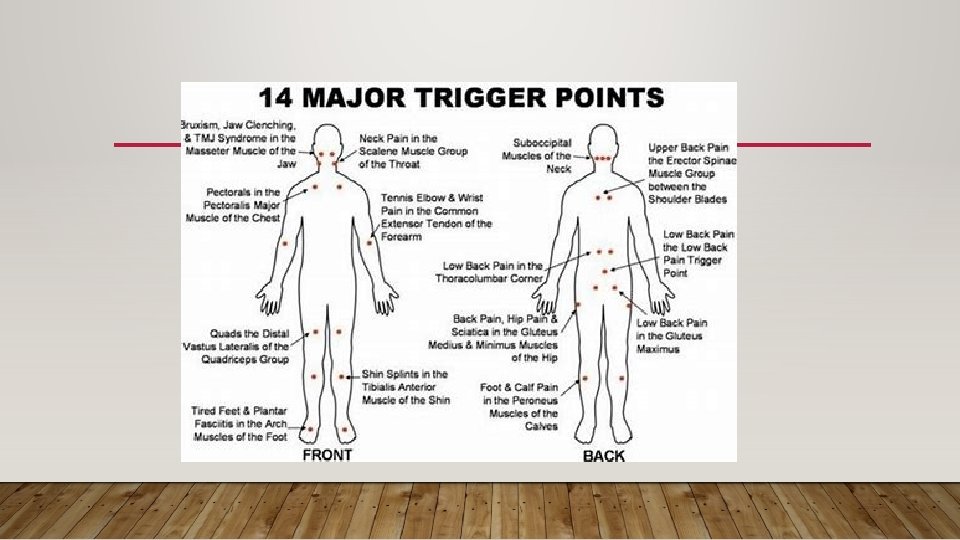
TRIGGER POINTS • Term coined by Janet Travell in 1942: • Pain caused by discrete hyperirriatble points in skeletal muscle or fascia not caused by acute trauma, inflammation, degeneration, neoplasm, or infection • Pain felt as a nodule or band in the muscle and a twitch response can be elicited on stimulation. • Palpation of a TP reproduces the patients complaint of pain and radiation to the muscle harboring the TP.
ACTIVATION OF A TRIGGER POINT • Acute or chronic muscle overload • Psychological Distress • Trauma • Radiculopathy • Smoking • Infection
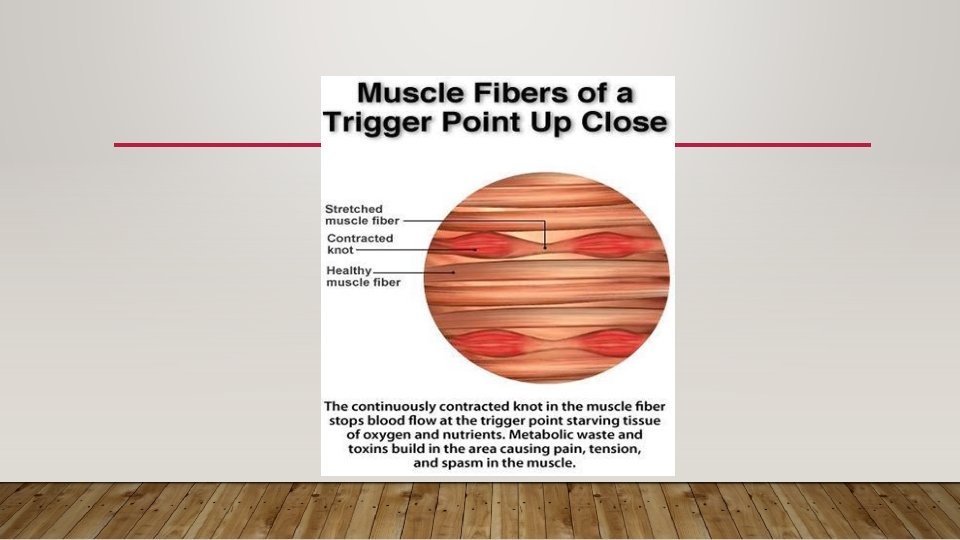
TRIGGER POINTS • Trigger Points form in muscles due to excessive release of acetylocholine producing sustained contraction of a muscle • Trigger Points: Increase Acetylcholine, Increase Norepinephrine, increase serotonin, decrease PH. • Sustained contraction causes Ischemia • Pain pathways follow particular nerve pathways.
INCIDENCE • 75 - 95% of regional pain caused by myofascial pain • 80 -90% of trigger points overly acupuncture points and all overly fascial planes. • Biopsy showed hyperirritable and electrically active muscle spindles • 255 programable trigger points • A. Active • B. Inactive • C. Latent
CAUSE OF SHOULDER PAIN • Mechanical: Impingement RC, Bursa • Pathological: Rotator cuff Tear, Labral Tear • Neurological: Cervical Neuropathy • Myofascial: Trigger Points • Visceral Disease
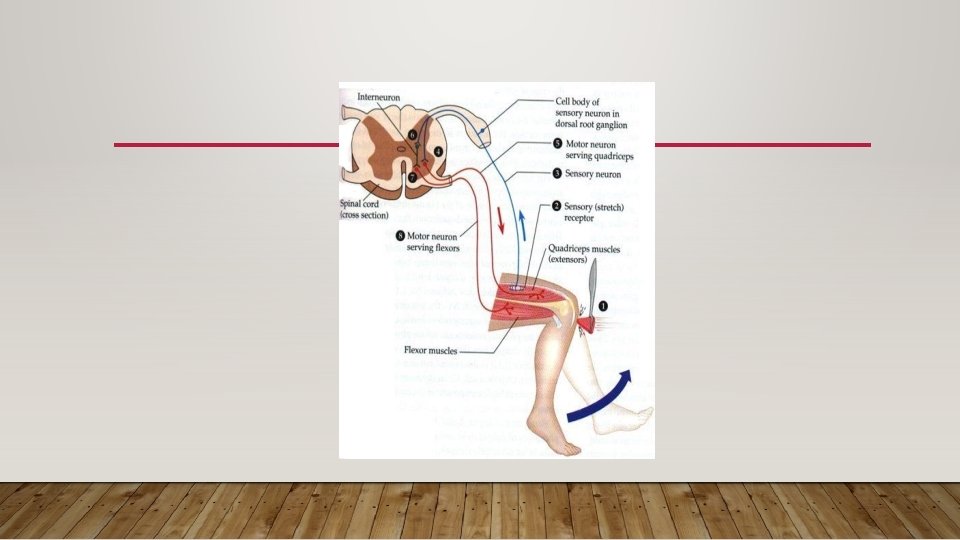
TRIGGER POINTS • Hyperirritable neuromuscular point that is painful when compressed and is associated with dysfunctional neuromuscular circuits. • Refers pain to a distal and predictable area. • By pressing on a trigger point the spinal cord produces pain reducing chemicals that relax the muscle and reduce the pain from the referral pattern
ALPHA MOTOR NEURONS • Most muscle contraction is due to increased alpha motor neuron activity in the extrafusal fibers. • Causes: Increased Calcium ions in tissue, Fibrosis, Ischemia, Referal pattern consistent and predictable • Treatment Goal: Block Alpha motor neuron activity, force Calcium ions out of tissue, block myotatic referal
TRIGGER POINT REFERRAL PATTERNS • Supraspinatus: Deep pain in mid deltoid with radiation down arm to elbow • Biceps Brachi: Shoulder, Posterior Scapula • Teres Major/Minor: Posterior Deltoid, Lateral Arm • Subscapularis: Posterior Shoulder, Posterior Arm, both sides of wrist. • Serratus Posterior Superior: • Latissimus Dorsi: Inferior Scapula. Posterior Arm, Hand. • Triceps: Posterior Shoulder, Lateral Forearm. Tennis Elbow
SHOULDER TRIGGER POINTS
HELENE LANGEVIN MD, PH. D UNIVERSITY OF VERMONT MEDICAL SCHOOL
TECHNIQUE GOALS • Ischemic Pressure: • Neurological: Break myotatic reflex • Physical: Move calcium ions out of the tissue
TECHNIQUE METHODS • Manual Technique: Pressure to patients tolerance. Nimmo taught “ As much as you could tolerate on your eyeball. ” 7 seconds twice. Treatment eventually evolved to use up to 40 pounds of pressure on Lumbar spine. ( I never use that technique). Follow the treatment with a muscle energy technique to lengthen out the muscle. • Spray and Stretch: Ethylchloride ( no loner used due to impact on environment ) • Dry Needling: Use of saline of analgesic did not improve outcome over placebo.