Reading the CXR Frank Schembri Pulmonary Critical Care

Reading the CXR Frank Schembri Pulmonary / Critical Care

Types of Densities

Basic Principles of the CXR • Types of views – PA – Lateral – AP – Apical lordotic – Decubitus (R & L)

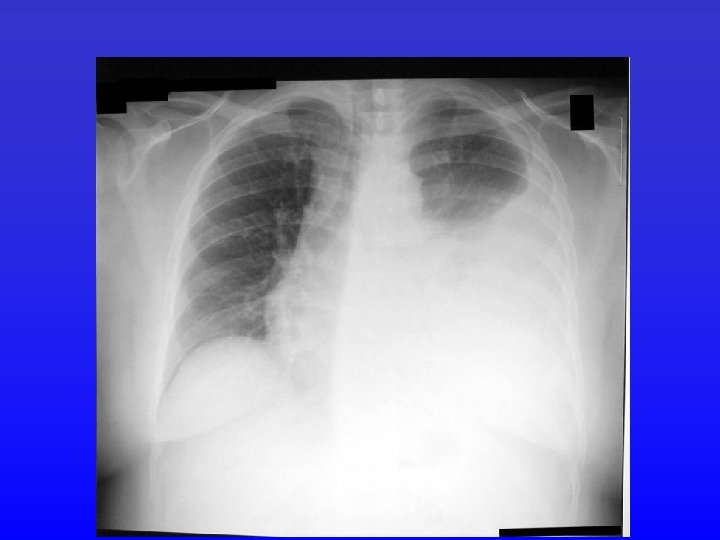
PA vs AP

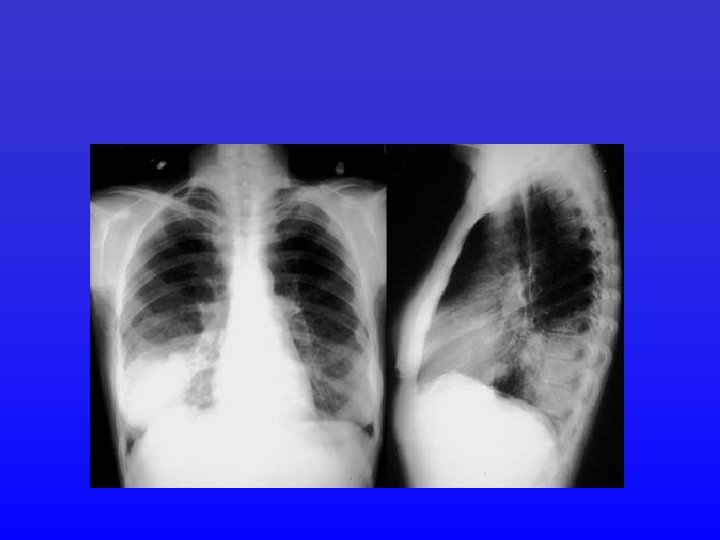
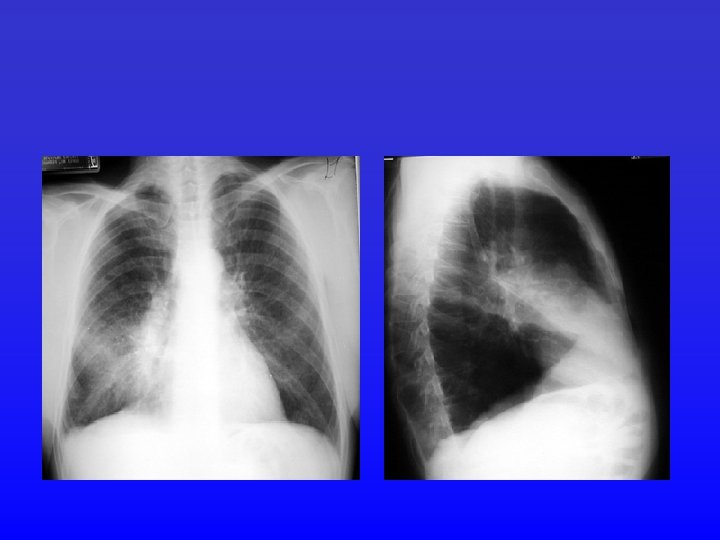
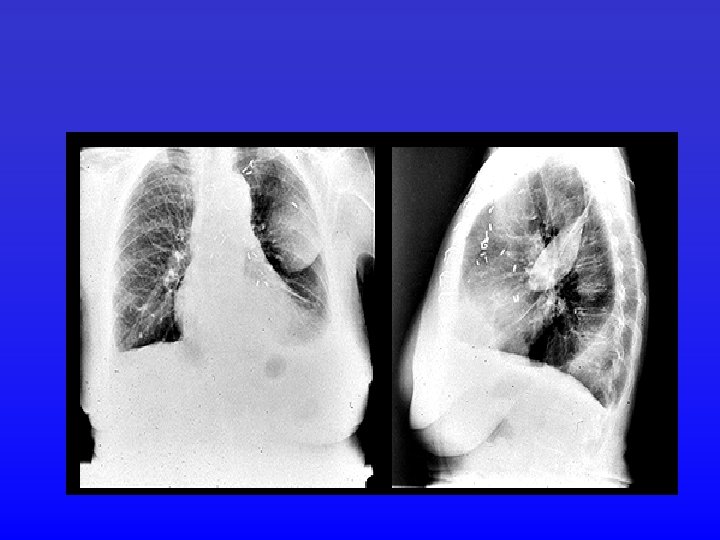
Lateral CXR

Apical Lordotic Chest

Decubitus Positioning

Approaching the CXR • • • Name, date, type of film Type of film Patient positioning / rotation Inspiration Penetration – White is underpenetrated – Black is overpenetrated

Approaching the CXR • The systematic approach 1. Tubes / Hardware 2. Bones 3. Soft tissues 4. Pleura and diaphragm 5. Trachea and mediastinum 6. Lung parenchyma

Rotation

Rotation

Inspiration

Penetration

Scanning the xray

Scanning the xray

# 1 - Hardware

#1 - Hardware

#1 - Hardware

#1 - Hardware

2. Osseous Structures in the Chest

2. Osseous Structures of the Chest

3. Soft Tissues

4. Pleura and Diaphragm

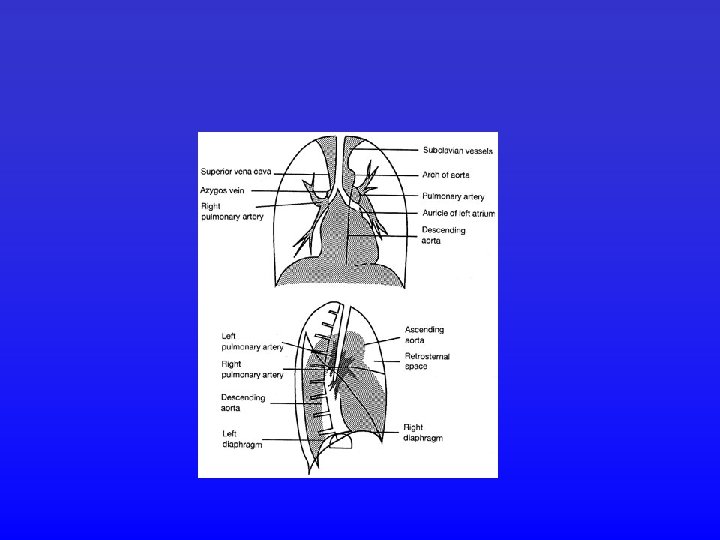
5. Mediastinal Anatomy

5. Mediastinal Anatomy

5. Mediastinal Compartments

6. Parenchymal Anatomy

Lateral View Anterior View

6. Parenchymal Anatomy

Left Lung Right Lung

Lobes • Right upper lobe:
 • Right middle lobe:")
Lobes (continued) • Right middle lobe:
 • Right lower lobe:")
Lobes (continued) • Right lower lobe:
 • Left lower lobe:")
Lobes (continued) • Left lower lobe:
 • Left upper lobe with Lingula:")
Lobes (continued) • Left upper lobe with Lingula:
 • Lingula:")
Lobes (continued) • Lingula:
 • Left upper lobe - upper division:")
Lobes (continued) • Left upper lobe - upper division:

Pneumonia

Atelectasis Loss of volume mass Minor fissure Elevation of diaphragm Minor fissue

Minor fissure Major fissure

Pneumothorax • Collection of air in pleural cavity • Primary and secondary causes • Upright position air rises and separates the lung from the chest wall creating a line. Don’t be fooled by skin folds, clothing and bullae. • In the supine position air moves anteriorly. The lung will not be clearly separated from the chest wall.

PTX

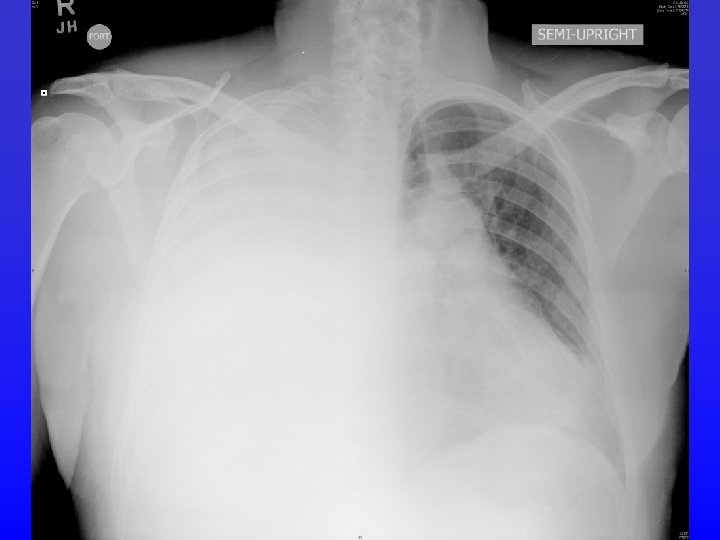
Pneumothorax in the Supine Patient Enlarged hemithorax Mediastinal shift hyperlucent Deep sulcus sign Sharper cardiac border

Tension

Pneumothorax

Bat-winged appearance Enlarged heart

CHF Perihilar infiltrates/enlarge PA Pleural effusions

Kerley B lines


Effusions

- Slides: 57