REABSORPTION IN THE LOOP OF HENLE The thin

REABSORPTION IN THE LOOP OF HENLE The thin descending limb: It has low permeability to solutes but is highly permeable to H 2 O that is reabsorbed from the tubular fluid and its osmolality increases as it flows through the thin descending limb.
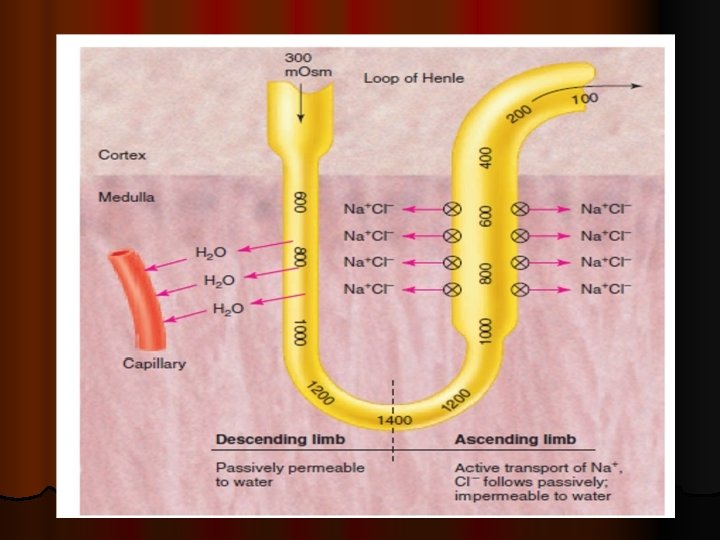

REABSORPTION IN THE LOOP OF HENLE l The ascending limb , can be divided into two regions: The thin& thick ascending limbs. l The thin ascending limb of juxtamedullary nephrons is impermeable to water but highly permeable to Na and Cl ions that diffuse passively from lumen to medullary interstitial space.

REABSORPTION IN THE LOOP OF HENLE l The thick ascending limb: l The water permeability of the thick ascending limb is negligible. It actively transports Na ions, while Cl &K ions transport is Na-co-transport. Therefore, the osmolality and the concentration of Na&Cl of the tubular fluid decreases. The tubular fluid that leaves the loop of Henle is hypotonic.

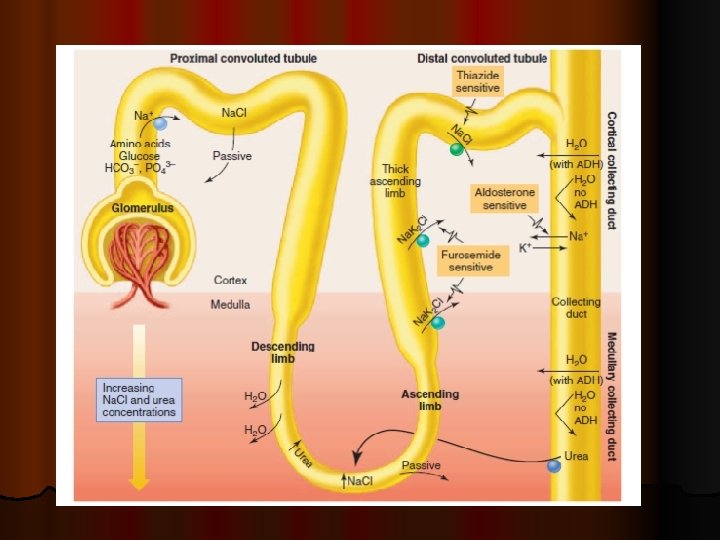
Functions of loop of Henle l 1 -It has an important role in the mechanisms for both urinary concentration and urinary dilution. l 2 -Reabsorption of 15 -20% of the filtered water. l 3 - Reabsorption of 25% of the filtered Na. l 4 - Reabsorption of Cl.

Functions of distal tubules &collecting ducts 1 -Active reabsorption of 8 -10% of the filtered Na &active secretion of K &H ions, it is under control of aldosterone hormone. l 2 -Reabsorption of up to 15% of the filtered water (facultative H 2 O reabsorption) which is under the control of ADH. l 3 - Reabsorption of urea from the inner medullary part of the collecting duct. l

RENAL MECHANISM FOR CONCENTRATING &DILUTING URINE l One of the important functions of the kidney is to control the osmolality and osmotic pressure of the body fluids. l The DCT&CD are impermeable to H 2 O when the ADH is not present in the circulating body fluids.

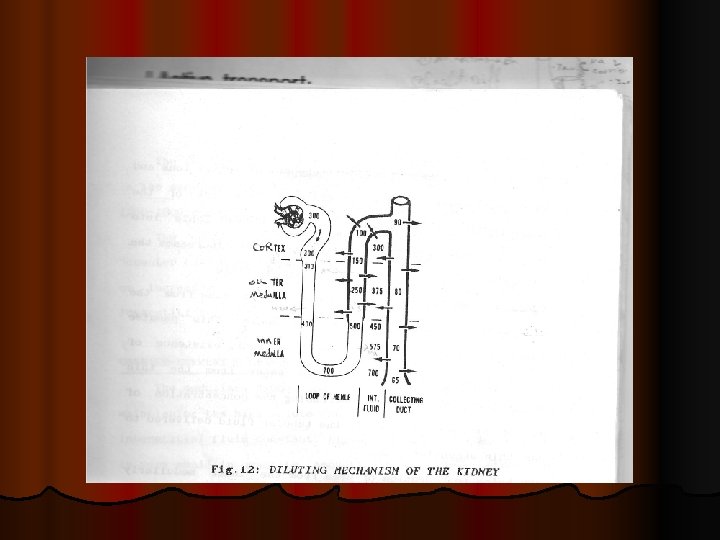
RENAL MECHANISM FOR CONCENTRATING &DILUTING URINE l -At the thick portion of the loop of Henle, and the first segment of the DT (diluting segment) there is active absorption of Na+ &secondary active absorption of Cl-. The osmolality of the fluid in ascending limb of the loop of Henle decreases progressively to about 100 m. Osm/Kg H 2 O.

RENAL MECHANISM FOR CONCENTRATING &DILUTING URINE l -In the DT &CD there is an active absorption of Na &passive absorption of Cl ion. l The osmolality of the tubular fluid decreases as little as 65 -70 m. Osm/Kg water.

RENAL MECHANISM FOR CONCENTRATING &DILUTING URINE l -The process for excreting dilute urine is absorbing solutes from the distal segments of the tubules, while H 2 O fails to be reabsorbed.

CONCENTRATING MECHANISM OF THE KIDNEY l The counter –current multiplier mechanism l In order to secrete the excess of electrolytes, or in inadequate water supply, the kidney excretes concentrated urine, so that excess solutes are excreted with a little loss of H 2 O from the body.

CONCENTRATING MECHANISM OF THE KIDNEY l The kidneys have a special mechanism for concentrating the urine called the counter current mechanism, The counter current mechanism depends on a special anatomical arrangement of the loop of Henle and the vasa recta. In human 1/3 to 1/5 of the nephrons are juxtamedullary nephrons, they have their loop of Henle dipping in the medulla. Parallel to these loops are loops of peritubular capillaries or vasa recta.

CONCENTRATING MECHANISM OF THE KIDNEY A counter current system is a system in which the inflow runs parallel, counter to, and adjacent to the outflow. When the ADH is high, the epithelium of the DCT and the CD becomes highly permeable to H 2 O and H 2 O is reabsorbed into the highly concentrated medullary interstitial fluid. l The first step in concentration of urine is to create the hyperosmolality of the medullary interstitial fluid. Four different soluteconcentrating mechanisms are responsible for this hyperosmolality. l

CONCENTRATING MECHANISM OF THE KIDNEY l 1 -The principal cause is active transport of Na ions &secondary active transport of Cl ions out of the thick portion of the ascending limb of loop of Henle into the outer medullary interstitial fluid. This increases the osmolality of the medullary interstitial fluid.

CONCENTRATING MECHANISM OF THE KIDNEY l 2 -Passive reabsorption of Na &Cl ions from the thin ascending limb of the loop of Henle this process depends on the prior presence of the medullary gradient to reabsorb H 2 O from the thin descending limb, so, increasing the concentration of Na&Cl ions in the tubular fluid delivered to the thin ascending limb.

CONCENTRATING MECHANISM OF THE KIDNEY l 3 -ADH helps reabsorption of urea from inner medullary part of the CD. This part becomes moderately permeable to urea and highly permeable to H 20 that is rapidly reabsorbed and this greatly increases urea concentration. urea diffuses by concentration gradient through the CD into the medullary interstitium its concentration is increased & increases the inner medullary fluid osmolality.

CONCENTRATING MECHANISM OF THE KIDNEY l 4 -Active reabsorption of Na from the CD into the medullary interstitial fluid associated with passive absorption of Cl. l The net result of these four mechanisms is an increase in the osmolality of the medullary interstitial fluid to 1200 -1300 m. Osm/kg H 20 in the pelvic tip of the medulla.

COUNTER-CURRENT EXCHANGE MECHANISM l The medullary blood flow has two characteristics for maintaining the high solute concentration in the medullary interstitial fluid constant

COUNTER-CURRENT EXCHANGE MECHANISM l 1 -The medullary blood flow is very small in quantity, because of this very sluggish(slow)blood flow, removal of solutes in minimized. l 2 -The vasa recta functions as a counter-current exchanger that prevents washout of solutes from the medulla.
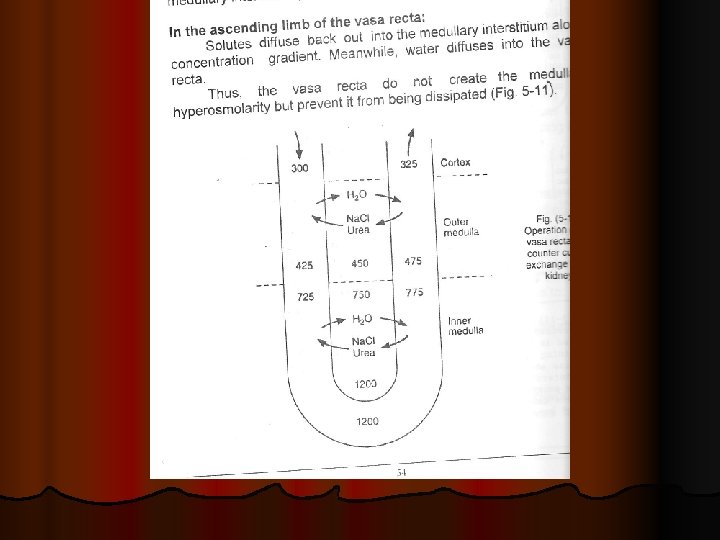

COUNTER-CURRENT EXCHANGE MECHANISM l As blood flows down the descending limb in the vasa-recta its osmolality is slightly lower than the osmolality of the medullary interstitial fluid, so, Na, Cl&urea diffuse from interstitial fluid into the blood , while H 20 diffuses out into the interstitum.

COUNTER-CURRENT EXCHANGE MECHANISM l The osmolality of the blood in the vasa recta increases to 1200 m. Osm/Kg H 2 O at its tip. Then, as blood flows back up in ascending limb, the osmolality of the blood is slightly higher than the osmolality of the medullary interstitial fluid, so Na, Cl &urea diffuse back out of the blood into the interstitium and H 20 diffuses back into blood. Thus, the blood of vasa-recta removes a little amount of solutes from the interstitial fluid

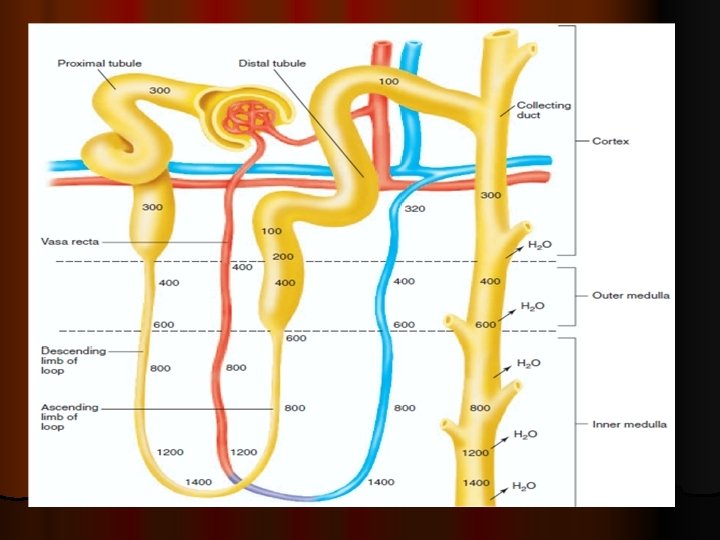
Osmolar concentration changes of the tubular fluid l 1 -In the PCT: Proportionate amount of H 2 O & solutes are absorbed by PCT it is highly permeable to both. The osmolality is equal to that of glomerular filtrate=300 m. Osm/Kg. H 2 O.

Osmolar concentration changes of the tubular fluid 2 -In the loop of Henle: The osmolality rises rapidly because of the counter-current mechanism and is multiplied. In the descending limb water is reabsorbed and the osmolality of the tubular fluid increases, it reached 1200 m. Osm/Kg H 2 O in the tip portion of the loop of henle. l In the diluting segment (thick ascending limb of loop of Henle and early part of DT) the osmolality falls because of low permeability to water &high permeability to actively absorbed solutes it reaches 100 m. Osm/Kg H 2 O. l l

Osmolar concentration changes of the tubular fluid l 2 -In the DCT&CD: The osmolality depends on the presence of ADH, in absence of ADH, very little water is absorbed, the osmolality is less than 100 m. Osm/Kg H 2 O because of the active absorption of solutes from this epithelium. In the presence of ADH the CD is highly permeable to water most of the water is reabsorbed producing very concentrated urine.
- Slides: 29