RCA qi cch org tw https qi cch

 討論 • RCA is a promising approach with considerable face")
 討論 • The first step in securing improvement is likely")
 討論 • Fourth, healthcare must focus increasingly on aggregated analysis")
 討論 • Finally, healthcare needs to do more to detect")
 討論 • • • RCA is a promising incident investigation")




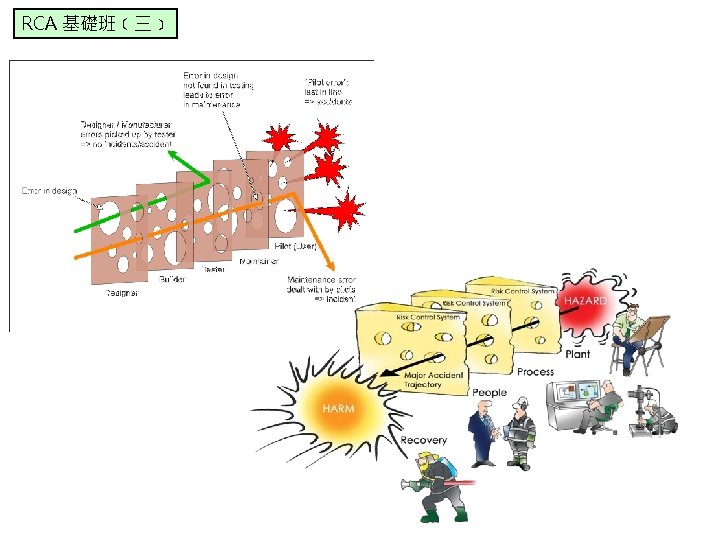
 Error producing conditions “Sharp end” (Active failures")



- Slides: 29
RCA 基礎班﹝三﹞ qi. cch. org. tw 遠端收集資料模組 • 屏障分析 https: //qi. cch. org. tw/zh-tw/fd/rca_barrier • 事件及促成因素關聯圖(ECF) • https: //qi. cch. org. tw/zh-tw/fd/rca_ecf https: //qi. cch. org. tw/zh-tw/fd/rca/flowchart-for-root-cause-analysis
RCA 基礎班﹝三﹞ Discussion (1) 討論 • RCA is a promising approach with considerable face validity as a way of producing learning from things that have gone wrong. But it has consistently failed to deliver benefits on the scale or quality needed. The eight problems we have discussed here mean that, too often, RCA results in the tombstone effect: though its purpose is to guard against a similar incident in the future, it may instead function primarily as a procedural ritual, leaving behind a memorial that does little more than allow a claim that something has been done. Incident investigation clearly will continue to play an important role in making healthcare safer, but it must first get better at doing what it does. • RCA是一個有前途的方法藉大量 面對正確性(標靶)當作一種學習, 從已經做錯事情產生。但是無法 在效益規模或品質需要上傳達。 那是因為本文討論的八個問題造 成”樣板(墓碑)效應”(套用一樣 的格式):RCA目的被認為是避免 類似事件未來再發生,功能被替 代而成為一個程序儀式,僅留存 做了一點點的記憶卻允許聲稱已 經做了一些事情。在健康照護更 安全,事件調查清楚將繼續扮演 重要的角色,第一步是要做到「 到位」。 http: //qualitysafety. bmj. com/content/qhc/early/2016/06/23/bmjqs-2016 -005511. full. pdf 2
RCA 基礎班﹝三﹞ Discussion (2) 討論 • The first step in securing improvement is likely to involve the • professionalisation of incident investigation: those conducting it need specialist expertise in underlying theories, ergonomics, human factors and hands-on experience of analytical methods. For these reasons, the establishment of professional investigatory bodies, such as the one shortly to be launched in the UK, are welcome—though the scope, reach and • impact of such bodies will need careful monitoring. Second, the role of patients and relatives in the investigative process needs to be recognised and valued. Such engagement has the potential to generate a unique perspective of the service provided from the end-user's perspective and may • foster dialogue that is informative to both causal analysis and design of risk controls. The psychological and emotional readiness of patients and families involved in the investigative process needs to be considered, along with the maturity and ability of the organisation to facilitate such a process within the appropriate legal framework. Transparency on the agreed level of involvement is paramount from the start and the outcomes of investigations should be available to patients and relatives, though clarity on how this should best be done is not yet available. Third, better • understanding of the role of blame is needed. The dissonance caused by claims of no-blame or even just culture and the reality is a source of confusion and distress in relation to RCAs. To address current confusions, clarity is needed on the distribution of responsibility between bodies investigating incidents (whose prime mandate would be to promote learning) and other bodies (including professional regulators and the law courts), and in what instances the investigative body needs to make referrals. 確保改進的第一步可能涉及事件調查的專業化: 執行此類 作的專業人員需要`具有專業知識的 基礎理論,如人體 程學、人為因素和分析方 法的實踐經驗。 由於這些原因,應建立專業調查機構,例如在 英國將發起專業調查機構,儘管這些機構的範 圍、影響程度需要仔細被監測。 第二,患者和親屬在調查過程中的作用需要得 到承認和重視。這種參與有可能從最終用戶的 角度引導事件的演變,並可能促進對因果分析 和風險的控制時,需要考慮參與調查過程的患 者和家屬的心理和情緒準備情況,以及組織在 法律框架內促進此類過程的成熟度和能力。 第三,需要更好的了解責任。因為無責任甚至 是文化所引起的不和諧,是為現實RCA的混亂 和困擾的根源,為了解決目前的困惑,需要明 確調查事件(其主要任務是促進學習)的機構 與其他機構(包括專業監管機構和法院)之間 的責任分配,以及調查機構需要做哪些事情轉介。 http: //qualitysafety. bmj. com/content/qhc/early/2016/06/23/bmjqs-2016 -005511. full. pdf 3
RCA 基礎班﹝三﹞ Discussion (3) 討論 • Fourth, healthcare must focus increasingly on aggregated analysis of • incidents. Such a bird's eye view of incidents may facilitate prioritisation of interventions, based on the harm associated with incidents and also on the associated risks. Aggregated analyses can be performed at numerous levels of the organisational hierarchy, for example, the micro (within one department) and at the meso level (organisational). At the national level, aggregated analyses offer a way of identifying common themes across similar and apparently more disparate incidents and may also serve as a means of generating actions that require collaborative efforts between healthcare organisations or indeed between industry and healthcare. Such an example could be for instance product redesigning—a solution that may not be identified through the analysis of a single incident within one department but may reveal itself as a recurring theme when analysing multiple incidents across many organisations. Linked to this, healthcare urgently needs to develop and evaluate much better methods for designing risk controls and other improvement actions. One possibility that could be evaluated, for example, is that of a hierarchy of risk controls. More broadly, the use of active surveillance of issues that have already been detected and monitoring of effectiveness of risk controls need to become a routine part of the risk management process following RCAs. Healthcare also needs to markedly improve its capacity to evaluate, curate and share these risk controls. Such an approach would help to address the problem that organisations tend to constantly reinvent risk controls, resulting in waste and the creation of new risks. An easily accessible database with descriptions of risk controls and contexts would enable lessons learnt from one RCA to be shared widely and support a participatory approach to organisational learning. 第四醫療照護業必須專注於逐漸增加的事件分析。以如 此巨觀的方式去檢視事件才可以根據事件本身和相關風 險所造成的危害,進而做出符合優先次序的處理。如此 所累積下來的分析結果可以運用於組織中的各種不同階 層,舉例來說,如微觀方式可運用於單一部門而中觀方 式可運用於機構內。以國家層級來看,這些累積下來的 資料提供了一種可以用來辨識各種類似或甚至不同事件 彼此之間的共同主題,也可以作為需要醫療機構或其他 產業與醫療照顧產業彼此相互協作的行動方案。這樣的 例子可說是產品的重新設計——在一個部門內看起來是 單一獨立事件,但是如果從眾多機構的多次事件累積起 來分析卻發現這是不斷重複發生的問題時,這可能就會 是一個解答。ヰ說回來,醫療產業急需開發及評估更好 的方法來規劃風險控管及品質改善方案。更廣泛地來說, 在做完 RCA 之後,以主動監測的方式,針對ᕬ被辨識出 並監測成效中的問題進行風險控管應ヱ變成是風險管理 事務中的一部分。醫療機構也應ヱ積極地增進自ᕫ評估 策劃及分享這些風險控管的潛力。這樣的方式可以幫助 讓機構中常常不斷製造出來的風險控管——造成浪費及 不斷製造風險的問題給浮現出來。一個有充分說明事件 來龍去脈及ヱ如何風險控管,內容ヲ盡且方便使用的資 料庫可以讓從一個 RCA 事件中學到的教訓能夠廣為分 享及散播,讓參與者能夠達到機構層級的學習效果。 http: //qualitysafety. bmj. com/content/qhc/early/2016/06/23/bmjqs-2016 -005511. full. pdf 4
RCA 基礎班﹝三﹞ Discussion (4) 討論 • Finally, healthcare needs to do more to detect hazards and assess • risks proactively. RCA is essentially retrospective, and depends crucially on an incident being recognised as such, but that may not happen for a variety of reasons: healthcare personnel may have become habituated to particular practices or outcomes, or fear and other negative emotions discourage reporting. Though RCAs were imported from other high-risk industries, the other tools and techniques commonly used in those industries to assess systems and assure their safety before an incident has occurred—such as failure modes and effects analysis (FMEA), hierarchical task analysis and so on—have had far less attention in healthcare 66 FMEA, in particular, may be especially useful for the rigorous proactive risk assessment of a select few but high-priority hazards. 67 For healthcare truly to become a learning system, action is needed on multiple levels. RCAs have dominated for too long as the principal means of generating learning. The time has come to recognise both their opportunities and their limits 最終,醫療照顧者需要正積極主動地 去評估危害和風險。RCA本質上是追 溯性的,並且在很大程度上取决於被 認定的事件本身,但可能不會形成, 可能的原因有醫療人員習慣性地去做 某些特定行為或是害怕有一些負面的 情緒,這些原因都會造成他們不願意 去報告意外發生。雖然RCA是從別的 高危險的產業引進的,還有其他方法 或是 具在意外發生之前被拿來檢測 整個體系的安全性,像是FMEA或是 hierarchical task analysis等等,但 這兩種非法比起RCA還要更少應用在 醫療體系。FMEA對於精確並積極主 動地去評估一些少數但必須積極優先 處理的危害特別有效果。為了讓醫療 真正成為一個學習的系統,需要多層 面的行動。RCA已經是循環學習的主 流太久了,需要去了解RCA的機會與 限制在哪裡。 http: //qualitysafety. bmj. com/content/qhc/early/2016/06/23/bmjqs-2016 -005511. full. pdf 5
RCA 基礎班﹝三﹞ Discussion (5) 討論 • • • RCA is a promising incident investigation technique • borrowed from other high-risk industries, but has failed to live up to its potential in healthcare. A key problem with RCA is its name, which implies a • singular, linear cause. Other problems include the questionable quality of many • RCAs, their susceptibility to political hijack, their tendency to produce poor risk controls, poorly functioning feedback loops, failure to aggregate learning across incidents and confusion about blame and responsibility. Implementation and evaluation of risk controls to • eliminate or minimise identified hazards need to become a more visible feature of the RCA process. To maximise learning, lessons learnt from incidents, • descriptions of implemented risk controls and their effectiveness need to be shared within and across organisations. RCA源自於其他高危險產業的事件調 查 具,但當它應用在醫療產業卻未 發揮其潛力! RCA最主要問題在於它的名字,其暗 示可能為單一或線性事故造成的。 其他問題包含有對各項RCA品質的質 疑,例如易受政治因素影響,產生不 好的危險風險控制和不好的功能回饋, 及無法從事件中獲得全面的學習,指 責與責任會產生混淆。 為了要減少或降低已確認災害所採取 的風險管控措施,是RCA過程中明顯 的特徵。 導入風險管理的事件描述中必須能在 組織內外彼此分享學習事件發生原因, 才能得到最大的學習成果。 http: //qualitysafety. bmj. com/content/qhc/early/2016/06/23/bmjqs-2016 -005511. full. pdf 6
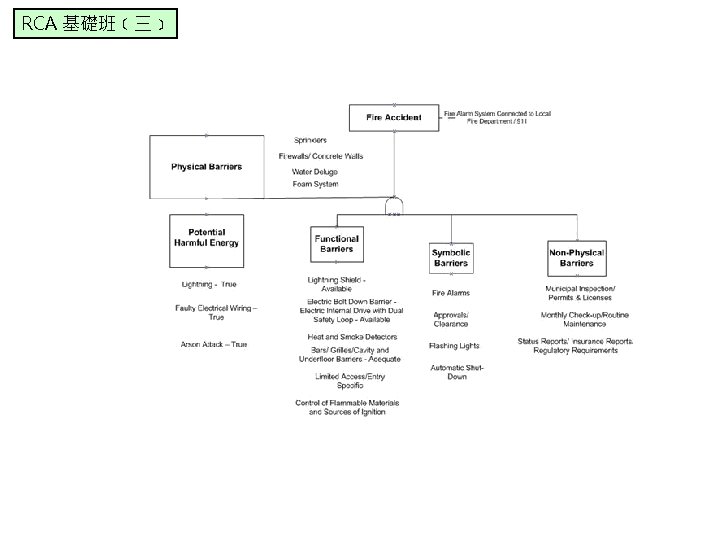
RCA 基礎班﹝三﹞ 屏障分析 Barrier Analysis 18
RCA 基礎班﹝三﹞ 屏障分析 “Blunt end” (latent failures) Error producing conditions “Sharp end” (Active failures eg slips, lapses, mistakes, violations) Patient safety incident Defences 19
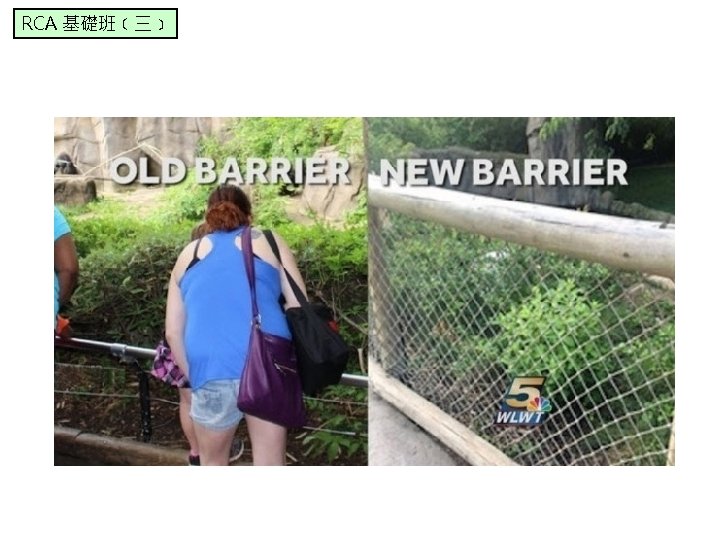
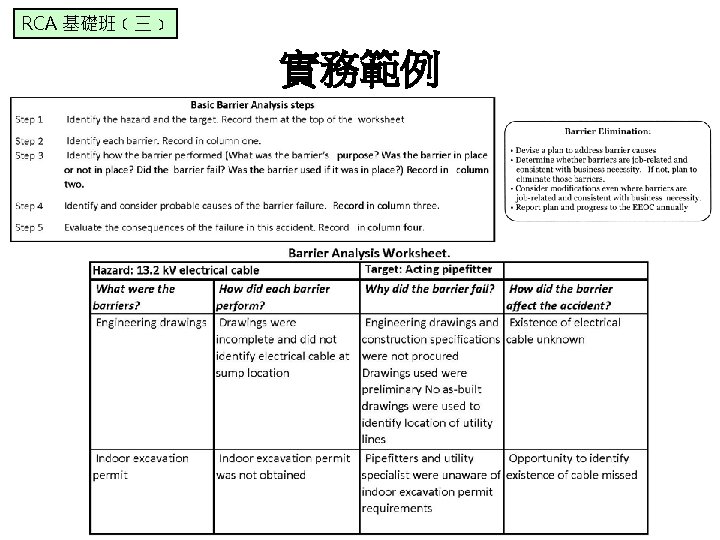
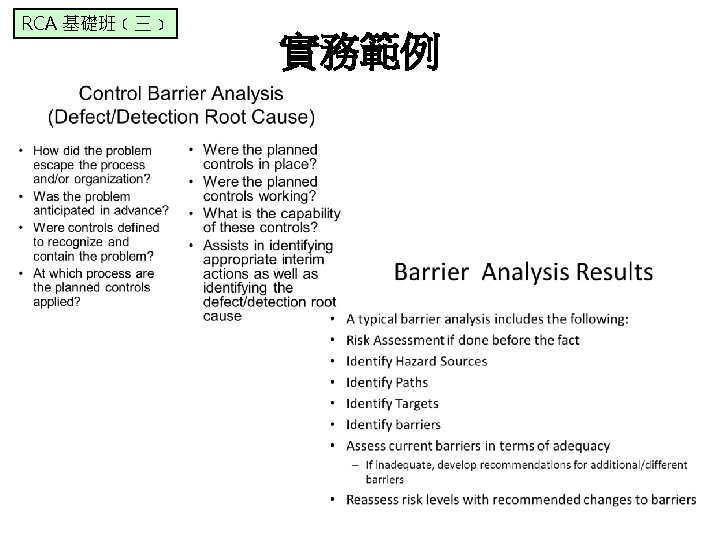
RCA 基礎班﹝三﹞ Barriers faced in trying to reach out to county school systems with youth enrichment activities 實務範例
RCA 基礎班﹝三﹞ 人為因素 Human Factors • • • A behavioral determinant is a reason why someone does or does not do something. In Barrier Analysis, participants are asked a series of questions to identify eight potential determinants (most of which are “barriers”) that can block people from taking action that will improve their own or their children’s lives (e. g. , exclusive breastfeeding to improve a child’s health). The questions can also identify the positive attributes of a behavior that act as “promoters” and can be used to “sell” a behavior during health promotion or other educational efforts. Barrier Analysis was designed using the scientific literature on behavior change. People used to think that knowledge was enough to change behavior, but scientists and program managers realized that many people know what they should do, but they still do not do it. There are many different theoreticians who have contributed to this literature, and thus to Barrier Analysis, but two of the main theories that underpin the method are the Health Belief Model and the Theory of Reasoned Action. http: //barrieranalysis. fh. org/what_is_barrier_analysis. htm 進 階 版
RCA 基礎班﹝三﹞ 計算故障概率 Calculating probability of failure 進 階 版