Raynauds Phenomenon Jorge Mera MD Presbyterian Hospital Dallas

Raynaud’s Phenomenon Jorge Mera, MD Presbyterian Hospital Dallas May 19, 2005

Clinical Case n A 26 YOHF with a 6 year Hx of SLE complicated with lupus nephritis on chronic hemodialysis, presented with severe Raynaud’s Phenomenon (RP) involving mainly her upper extremities. Despite standard treatment for 3 weeks she worsened, being aggravated by severe pain and ischemic ulcers of her fingertips, and the need to posture her hands downward to decrease the pain

Clinical Case
? What is the")
Questions n n n n n What is Raynaud's Phenomenon (RP)? What is the incidence of RP? What is the pathogenesis of RP? What is the difference between primary and secondary RP? What are the most frequent causes of secondary RP Why doesn't every patient with RP develop critical ischemia What lab test should you order in a patient with RP? How do you treat critical ischemia?

RAYNAUDS PHENOMENON n n Definition: – It is an exaggerated vascular response to cold temperature or emotional stress History: – Raynaud's Syndrome was described in 1862 by Maurice Raynaud. He thought it was a vasculopathy was related to an exaggerated response of the CNS. – In 1930 Sr. Thomas Lewis proposed RP was due to a “local fault” since it did not get cured with sympathectomy.

RAYNAUDS PHENOMENON n n More common – – – In women Younger age groups Family members of patients with RP Affected areas – – – Hands are the most common Toes Ears Face Knees nipples

Incidence n Incidence: – The incidence of RP varies according to the type of center reporting. Populations studies show an incidence of 4 - 9 % in women and 3 – 6 % in men. – In population studies, most cases (90 %) are due to Raynaud's Disease or Primary Raynaud's Phenomenon n The only prospective study to determine the incidence and natural history of RP in a community- based cohort study was reported by Suter et al. using the Framingham Heart Study Offspring Cohort; n They Followed 641 men and 717 women during a 7 year period

Incidence, persistence and remission of RP in women and men Baseline prevalent RP Incident RP Persistent RP Remitted RP Women Men P 78/717 (10. 9) 14/639 (2. 2) 28/78 (35. 9) 50/78 (64. 1) 50/641 (7. 8) 9/591 (1. 5) 18/50 (36. 0) 32/50 (64) 0. 05 Suter et al. Arthritis and Rheumatism 2005: 52(4); 1259 -63 0. 4 0. 2 0. 1

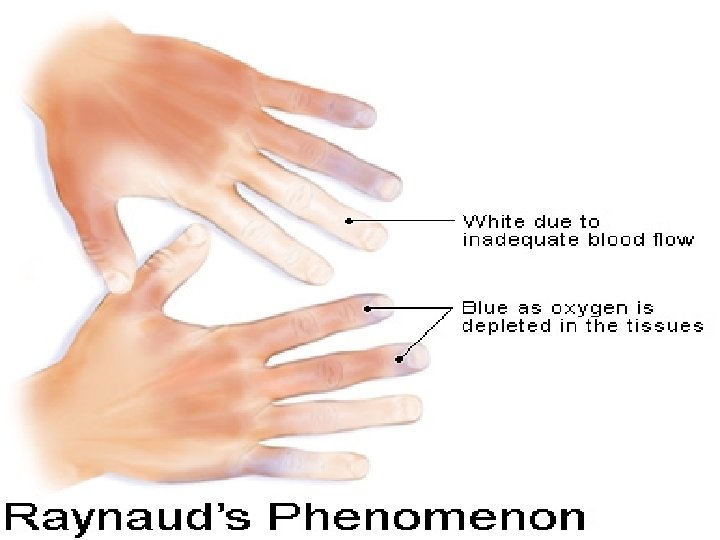
Clinical Manifestations n n Most commonly affects the hands Typical symptom – Distinct, episodic, sudden and reversible onset of cold fingers (or toes) with sharply demarcated color changes of n Skin pallor (White attack) and / or Cyanotic skin (blue attack) n Blushing of the skin upon recovery n Erythema of reperfusion (RECOVERY PHASE) n – With or without pain ISCHEMIC PHASE Lasts 15 – 20’

Clinical Manifestations n n Begins in a single finger and spreads to other digits symmetrically in both hands. The most frequently involved digits are – – – n Index finger Middle finger Ring finger The Thumb is often spared

Clinical Manifestations n n n Cyanosis occurs when blood flow is delayed in the capillary vessels and the stagnant blood becomes deoxygenated. Although it may be associated with numbness and dysesthesias it is not associated with ischemic events. The lack of pain and the ability to demonstrate a healthy capillary refill on pressure is evidence that nutritional flow is till present. Skin pallor with sharp demarcation, especially if accompanied by pain suggests complete closure of the digital arteries and coetaneous vessels. Severe critical ischemia include – Numbness and intense pain of the whole digit, hand or distal limb – Posturing of the involve hand downward

Active Raynaud's Phenomenon Wigley, F. M. N Engl J Med 2002; 347: 1001 -1008

Raynaud’s phenomenon, blanching of hands

Raynaud’s phenomenon: hands

Scleroderma: Raynaud’s phenomenon, cyanosis of the hands


Triggers n n Cold exposure Temperature shift Body chill Stimulation of the sympathetic nervous system – Emotional stress

PATHOGENESIS

CUTANEOUS CIRCULATION n Cutaneous circulation is critical for thermoregulation – Blood flow can vary from 250 ml/min at room temperature to 6000 ml/min during exercise (60% of Cardiac Output) n Regulated – Sympathetic system – Local factors

CUTANEOUS CIRCULATION n Most of the skin has – Sympathetic vasoconstriction fiber – Sympathetic vasodilatation fibers n The palms, soles and lips only have – Sympathetic vasoconstriction fiber
 Vasodilator Sensory afferent (+) ? CGRP, NKA,")
CUTANEOUS CIRCULATION NO Sympathetic Local Temperature (+) Vasodilator Sensory afferent (+) ? CGRP, NKA, SP Internal Temperature Skin Temperature Cutaneous arteriole NE, NPY Sympathetic Vasoconstrictor (-)

CUTANEOUS CIRCULATION n n n The skin is generally in a vasoconstriction “mode”. And the vasodilatation is only stimulated during exercise or intense heat The vasoconstriction occurs by stimulation of Alfa-2 adrenergic receptors The receptors can be subdivided in Alpha 2 A, 2 B or 2 C

Vasoconstriction Secondary to Cold Norepinephrine Alfa-2 C adrenergic receptor Alfa-2 A, 2 B adrenergic receptor Alfa 2 A, B Alfa-2 C adrenergic receptor Cold Temperature

Smooth Muscle Cell Contraction in an Arteriole
")
Vasoconstriction Secondary to Stress Alpha-2 (A, B, )

Vascular Response to Cold tttttttttt ttt

Why do Some Patients Develop Critical Ischemia? n Thermoregulatory flow. Corresponds to 80 – 90 % of flow. Sympathetic regulation of A-V shunts n Nutritional flow (constitutive), ischemia occurs when it is compromised THE TWO COMPONENTS OF DIGITAL BLOOD FLOW

PATHOGENESIS OF RAYNAUDS IN SYSTEMIC SCLEROSIS n Vascular injury – – Microcirculation Small and medium blood vessels n Genetic Factors n Altered angiogenesis – Familial aggregation documented but studies in monozygotic twins are needed n n Diminished expression of Alphav. B 3 integrin (receptor associated with VEGF mediated angiogenesis) Immune mediated – Cytokines (Increased Il-13 that correlates with microvascular injury) – Lymphocytes transendothelial migration (Increased CD 3+, CD 4+ activated T cell migration)

Pathogenesis of Digital Ischemia in RP Secondary to Scleroderma Intimal Proliferation and fibrosis Narrow arteriole lumen (75%) Anti endothelial Ab CD 4 Lymphocytes Ischemia Endothelial Insult Hypoxia Infection Prostacyclin Platelet Activation Nitiric Oxide VASODILATATION Tromboxane Serotonin VASOCONSTRICTION Reperfusion

PATHOGENESIS: Summary n In primary RP, abnormal vasoconstriction of digital arteries and cutaneous arterioles due to a local defect in normal vascular responses is thought to underlie the primary form of this disorder, evidence suggests the defect is an increase in alpha-2 adrenergic responses in the digital and cutaneous vessels. This increased response could be due to – Increased sympathetic activity – Increased sensitivity to adrenergic stimuli – Increased number of alpha-receptors in the vessel wall n In secondary RP, the defect may vary depending upon the underlying insult to the normal physiology of the digital and cutaneous arteries.
 n Secondary or associated to other medical disorders n")
Classification n Primary: (Raynaud's disease) n Secondary or associated to other medical disorders n Undefined – Non specific symptoms – Non definite lab abnormalities

RAYNAUDS PHENOMENON n It is manifested clinically by sharply demarcated color changes of the skin of the digits. n Rarely causes ischemia lesions on Primary Disease n Ischemic lesions in Secondary Raynaud's is not uncommon

Causes of secondary Raynaud’s phenomenon n n Connective tissue diseases – Scleroderma, systemic lupus erythematosus, MCTD, undifferentiated CTD, Sjogren’s syndrome, dermatomyositis Occlusive arterial disease – Atherosclerosis, anti-phospholipid antibody syndrome, Buerger’s disease Vascular injury – Frostbite, vibratory trauma Drugs and toxins – Beta blockers, vinyl chloride, bleomycin, ergot, amphetamines, cocaine Hyperviscosity/cold-reacting proteins – Paraproteinemia, polycythemia, cryoglobulinemia, cryofibrinogenemia, cold agglutinins

Diagnosis n n History of a characteristic attack Or 3 out of the 4 following symptoms – Unusual cold sensitivity – Unusual digital color changes – Positive response for blanching in comparison with a color chart and in response to the question “What is the palest your fingers ever get? ” – A positive response for blanching in comparison with actual photographs displaying digital blanching

Diagnostic Criteria n Definite RP: Repeated episodes of biphasic color changes upon exposure to cold n Possible RP: Uniphasic color changes plus numbness or paresthesia upon exposure to cold n No RP: No color changes upon exposure to cold Brennan et al. Br J Rheumatol 1993; 32: 357

Differential Diagnosis n Normal response to cold. Skin mottling may be present but – The recovery phase is immediate – There is no sharp demarcation of color changes in skin n Acrocyanosis – Permanent bluish discoloration in hands nose and ears
 n n n Symmetric episodic vasospastic attacks")
Criteria for Primary Raynaud's Phenomenon (Raynaud's Disease) n n n Symmetric episodic vasospastic attacks precipitated by cold or emotional stress Absence of tissue necrosis or gangrene No history or physical findings suggestive or secondary RP Normal ESR and serologic findings (ANA) Normal nail fold capillaroscopy Wigley, F. M. N Engl J Med 2002; 347: 1001 -1008
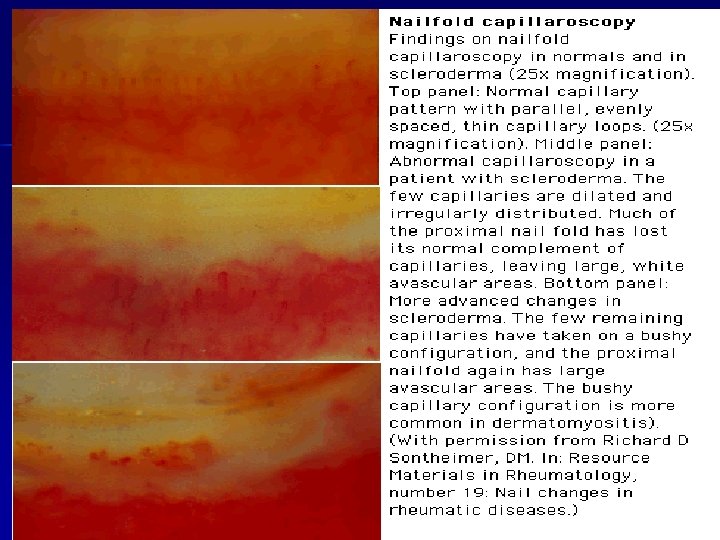

Nail-Fold Capillaries in a Patient with the CREST Syndrome (Calcinosis Cutis, Raynaud's Phenomenon, Esophageal Dysfunction, Sclerodactyly, and Telangiectasia), or Limited Scleroderma Wigley, F. M. N Engl J Med 2002; 347: 1001 -1008

Clues for the Diagnosis of Secondary RP Age of Onset > 40 n Male gender n Signs of tissue ischemia (ulcers) n Asymmetric attacks n RP associated with signs or symptoms of another disease n Abnormal laboratory parameters n

Progression to CTD n Primary 13 % CTD (The majority evolve to CREST or Systemic Sclerosis) n + ANA is a predictor for evolving from RP to CTD

Scleroderma: digital pitting scars

CREST syndrome: calcinosis cutis, fingers

Scleroderma: calcinosis, hands

CREST Syndrome n n Calcinosis Raynaud’s Esophageal dysfunction Telangiectasias

Evaluation n Negative Hx, Physical Exam and Nail capillaroscopy: No need for further testing n If above is abnormal – – – ANA Anti-centromere Complement Cryoglobulins Anti-Phospholipids antibodies TSH

TREATMENT

Treatment n Multiple treatment modalities appear effective n 10 - 40 % respond to placebo n Measure – Frequency – Severity – Digital ulcer healing or appearance

Treatment n General Measures – – Eliminate unfounded misconceptions Manage anxiety Avoid sudden cold exposure Keep the whole body warm (remember chills can precipitate an attack even if the hands are warm) – Avoid smoking – Avoid medications that cause vasoconstriction n n n B-blockers Nasal decongestants Caffeine ? Herbs containing ephedra Amphetamines Cocaine Behavioral therapy ?

Pharmacologic Treatment of Raynaud's Phenomenon
 (+-) Cisaprost (prostacyclin analog)")
Treatment n Oral Prostaglandins – – Misoprostol (oral PGE 1) (+-) Cisaprost (prostacyclin analog) (+) Beraprost (prostacyclin analog) (+-) Iloprost (–) n Anticoagulation n Sympathetic block – ASA ? – Heparin in critical ischemia (+-) – If associated with APLS

Management of Raynaud's Phenomenon Education/Prevention Avoid cold exposure Avoid vasoconstrictor meds Good skin care Aspirin 81 mg Asses Severity of Raynaud's Phenomenon Mild: Few attacks occurring only during cold exposure Moderate: Severe: Multiple symptomatic Episodes of RP occurring wo critical ischemia X episodes of recurrent ischemia or digital gangrene Monitor Clinically Consider VD therapy in Winter months Critical ischemia with evidence of macro vascular disease Initiate Vasodilator therapy: Ca Channel blockers YES NO Hospitalization Pain Control High Dose VD therapy Consider Sympathetic Block Prostacyclin Infusion Treat infection Pain control Local wound care Maximize VD therapy

Approach to the Diagnosis of Raynaud's Phenomenon

Clinical Case n LABS: – – – – – d. SDNA: 1: 1280 (ref. negative) C 3: 46. 7 mg/dl (ref: 86. 0 -185. 0) C 4: < 10 mg/d. L(ref. 20. 0 -59. 0). Lupus Anticoagulant: Negative Cryoglobulins: Negative. HIV: Negative RPR: Negative Hep C ab: Negative AFLA: Negative n Chest radiograph: n TEE: Within normal limits – Mild Pulmonary congestion

HOSPITAL COURSE: Second day n Working diagnoses: – Refractory Severe Raynaud's Phenomenon secondary to SLE with digital ischemia n Rescue treatment: – Epoprostenol 0. 5 ng/kg/min IV via central line; subsequently increased to 2 ng/kg/min. n Results: – Significant improvement after three days of infusion with documented regression of the ischemic changes in her digits.

60 minutes after Epoprostenol infusion

 Who’s on")
Double Blind Randomized Study: Margaritas vs Placebo for RDS (Resident Depression Syndrome) Who’s on the Placebo Arm?
- Slides: 60