Rapid Sequence Intubation Delon F P Brennen MD

Rapid Sequence Intubation Delon F. P. Brennen, MD MPH Pediatric Emergency Medicine Morehouse School of Medicine

Outline • Definition • Indications • Method

Definition • The induction of a state of unconsciousness with complete neuromuscular paralysis to achieve intubation without interposed mechanical ventilation in efforts to facilitate the procedure and minimize risks of gastric aspiration

Indications • Failure of airway maintenance/protection - lost or diminished gag reflex • Failure of oxygenation/ventilation - asthma, aspiration, pneumonia • Anticipated clinical course - multiple trauma, head injured - intoxication, air transport
 • Preparation: T-10 mins – Positioning • • • Preoxygenation: T-5")
Method (6 P’s) • Preparation: T-10 mins – Positioning • • • Preoxygenation: T-5 mins Premedication: T-3 mins Paralysis: T-1 min Placement of tube: T-0 mins Post management

Preparation • Evaluate – LEMON • • • Equipment Check Positioning Drug Selection IV’s, monitor, oximetry Ancillary Staff Anticipate alternative airway maneuver

LEMON • LEMON – L-Look – E-Evaluate – M-Mallampati – O-Obstruction – N-Neck mobility



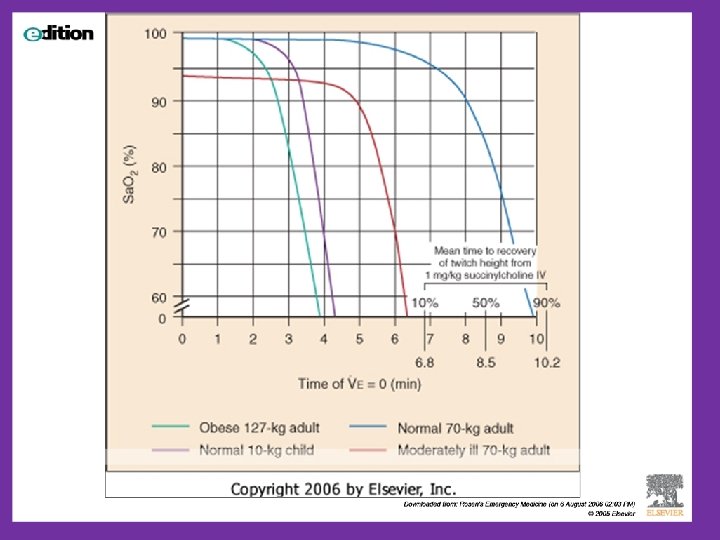
Preoxygenation • 100% O 2 for 5 minutes or 5 vital capacity breaths can theoretically permit 3 -5 minutes of apnea before desaturation to less than 90% occurs • NOT Positive Pressure Ventilation – If possible

Premedication • Goal – blunt the patient’s physiologic responses to intubation • Which are ? – bradycardia – hypoxemia – cough/gag reflex – increases in intracranial, intraocular, and intragastric pressures

Premedication • • Lidocaine Opioid Atropine Defasciculating doses “priming”

Lidocaine • Thought to blunt the rise in ICP associated with airway manipulation and the use of depolarizing neuromuscular blocking agents • Dose: – 1. 5 - 3 mg/kg (3 mins prior to intubation)

Atropine • Minimize vagal effects, bradycardia, secretions – Infants and children < 8 yrs may develop profound bradycardia during intubation • 0. 02 mg/kg (minimum 0. 1 mg IV, max 1 mg) 3 minutes prior to intubation
 • Attenuates")
Defasciculating Doses • Decreases muscle fasiculations caused by the depolarizing agents (succinylcholine) • Attenuates rise in intracranial pressure • Agents - non-depolarizing blocking agents (vecuronium, pancuronium, etc. ) – Usually 1/10 of standard dose

Sedation • Sedative agents administered at doses capable of producing unconsciousness with little or no cardiovascular effects • No ideal agent exists • Sedation should nearly always be used when paralyzing the patient

Sedation • • • Barbiturates/hypnotics Non-barbiturate Neuroleptics Opiates Benzodiazepines
, Methohexital (Brevital) • Short onset - 10 -20 secs, •")
Barbiturates/Hypnotics • Thiopental (Pentothal), Methohexital (Brevital) • Short onset - 10 -20 secs, • Duration - 5 -10 mins • May reduce ICP, cerebro-protective • Histamine release, hypotension, bronchospasm
 – nonbarbiturate hypnotic • Rapid onset, short duration • •")
Barbiturates/Hypnotics • Etomidate (Amidate) – nonbarbiturate hypnotic • Rapid onset, short duration • • Decreases ICP/IOP Minimal hemodynamic effects No histamine release Increases seizure threshold

Etomidate • No malignant hyperthermia reported • Watch for myoclonus, vomiting • May decrease cortisol synthesis (adrenal insufficiency) • Dose 0. 3 mg/kg IV
 – sedative hypnotic • Extremely rapid onset (10 sec), •")
Barbiturates/Hypnotics • Propofol (Diprivan) – sedative hypnotic • Extremely rapid onset (10 sec), • Duration of 10 -15 minutes • Decreases ICP, Can cause profound hypotension • Dose 1 -3 mg/kg IV for induction • Dose: 100 -200 mcg/kg/min for maintenance

• Ketamine – dissociative anesthetic, not a sedative • Rapid onset (1 -2 mins), short duration (~15 mins) • Potent bronchodilator, useful in asthmatics • Increases ICP, IOP, IGP, (beware in head injuries) • Increases bronchial secretions • “Emergence” phenomenon – rarely in children <10 yrs , common in adults • Dose: 1 -2 mg/kg

Opiates
, long duration - 30 min – Does not")
Fentanyl • Rapid onset (<1 min), long duration - 30 min – Does not release histamine • May decrease tachycardia and hypertension associated with intubation • Seizures and chest wall rigidity – Can be reversed with Naloxone • Dose: 2 -10 mcg/kg IV
 minutes and duration (2 -6) hours •")
Morphine Sulfate • Longer onset (3 -5) minutes and duration (2 -6) hours • May not blunt the rise in ICP, hypertension and tachycardia as well as fentanyl • Histamine release • Dose 0. 1 -0. 2 mg/kg IV

Benzodiazepines

Benzodiazepines • • • Midazolam, Diazepam, Lorazepam Provide excellent amnesia and sedation Broad dose-response relationship Reversed with Flumazenil Doses required are higher for RSI than for general sedation
 min than the barbiturate/hypnotic agents • Considered short-acting")
Midazolam • Slower onset (3 -5) min than the barbiturate/hypnotic agents • Considered short-acting (30 -60 min) • Does not increase ICP • Causes respiratory and cardiovascular depression • Dose: 0. 1 -0. 4 mg/kg IV

Diazepam and Lorazepam • Moderate/long acting agents • Longer onset time than midazolam • May be more beneficial post-intubation for sedation

Paralysis

Neuromuscular Blocking Agents • Chemical paralysis facilitates intubation by allowing visualization of the vocal cords and optimizing intubating condition • Only CONTRAINDICATION is anticipated difficult airway – Mallampati Class (I-IV) – Thyromental Distance

Depolarizing Agents • Exert their affect by binding with acetylcholine receptors at the neuromuscular junction, causing sustained depolarization of the muscle cell

Nondepolarizing • Bind to acetylcholine receptors in a competitive, non-stimulatory manner, no receptor depolarization • Histamine release • Reversed with edrophonium or neostigmine • Caution with myasthenia gravis
 • Nondepolarizing Agents – Pancuronium (Pavulon) –")
Agents • Depolarizing agents – Succinylcholine (Anectine) • Nondepolarizing Agents – Pancuronium (Pavulon) – Vecuronium (Norcuron) – Atracurium (Tracrium) – Rocuronium (Zemuron) – Mivacurium (Mivacron)

Succinylcholine • Gold standard for >50 years • Stimulates nicotinic/muscarinic cholinergic receptors • Onset 45 secs, duration 8 -10 mins • Dose: Children 2. 0 mg/kg IV – (adults 1. 5 mg/kg IV) • Inactivated by pseudocholinesterase

Succinylcholine cont • Prolonged paralysis seen with: – Pregnancy – Liver disease – Malignancies – Cytotoxic drugs – Certain antibiotics – Cholinesterase inhibitors – Organophosphate poisoning

Succinylcholine • Adverse reactions – Muscle fasiculations – Hyperkalemia – Bradycardia – Prolonged neuromuscular blockade – Trismus – Malignant hyperthermia

Depolarizing Agents • Muscle fasiculations – Thought to increase ICP/IOP/IGP – Causes muscle pain – Minimized by “priming” dose of non-depolarizing NMB • Hyperkalemia – Average increase in potassium of 0. 5 -1 m. Eq/L – Burns, crush injuries, spinal cord injuries, neuromuscular disorders, chronic renal failure

Depolarizing agents • Bradycardia – Most common in kids <10 yrs 2 o higher vagal tone – Especially w/ repeated doses of succinylcholine – Premedicate with atropine

Depolarizing Agents • Malignant hyperthermia – From excessive calcium influx through open channels – Genetic predisposition – Rapid rise in temperature, rhabdomyolysis, muscle rigidity, DIC – 60% mortality – Treatment: IV Dantrolene
 – Usually in children – Unknown cause –")
Depolarizing Agents • Trismus (Masseter spasm) – Usually in children – Unknown cause – Treat with a nondepolarizing NMB
 • Long-acting agent (45 -90 min) •")
Pancuronium • Slow onset (1 -5 min) • Long-acting agent (45 -90 min) • Renal excretion • Vagolytic tachyarrythmias common • Dose: 0. 10 -0. 15 mg/kg IV

Vecuronium • Onset of 1 -4 min • Duration of 30 -60 min • Hypotension may occur from loss of venous return and sympathetic blockade • Mostly biliary excretion • Dose 0. 1 mg/kg – “priming dose” 0. 01 mg/kg
 • Duration 30")
Rocuronium • Shortest onset of the nondepolarizing agents (1 -3 min) • Duration 30 -45 min • Tachycardia can occur • Dose: 0. 6 -1. 2 mg/kg (1 mg/kg)

Placement of Tube • Allow medications to work and assure complete neuromuscular blockade of the patient • Maintain Sellick maneuver until cuff inflated • Ventilate with bag-valve mask if unsuccessful • Additional doses of sedatives/NMB may be necessary • Confirm tube placement

Post Intubation Management • Secure tube • Continuous pulse oximetry • Reassess vital signs frequently • Obtain chest x-ray, ABG • Restrain (physical/chemical)patient • Consider long term sedation

Questions? ? Thank You!
- Slides: 48