Rapid Acting Insulin Analog Majid Valizadeh M D





 Cumulative incidence")




 Insulin?")



 § Rapid acting analogues")
 Insulin § Onset of action: 0. 5")
 § After SQ injection HRI tends to dissociate from its")



 A chain Gly S 1 S Gln Lys")

 •")













 and additional searching (pharmaceutical companies, experts,")
 values")


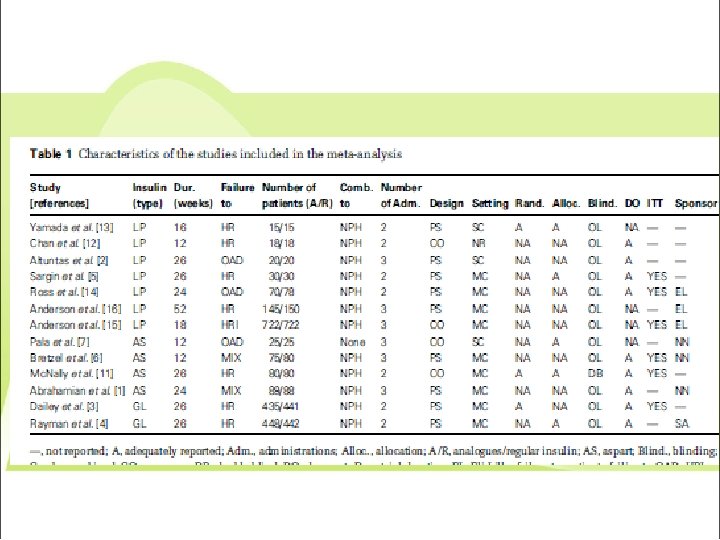
 with a duration >4 weeks comparing short-acting insulin")

 were")


 § Rapid acting analogues")


 after subcutaneous (sc) injection of analog insulins")










: 87– 90.")









- Slides: 83
Rapid Acting Insulin Analog Majid Valizadeh, M. D. Obesity Prevention and Treatment Research Center Research Institute for Endocrine Sciences Shahid Behesti University of Medical Sciences RIES 16 Nov 2017 Tehran, Iran
AGENDA Introduction Why To Use Prandial Insulins? The Importance of Controlling Post Prandial Glucose Prandial Insulins Different Types of Prandial Insulins Mechanism of Action of Insulin Glulisine Comparison between different types of SAI (short acting insulin) efficacy / side effects / patient preference Summary & Conclusion
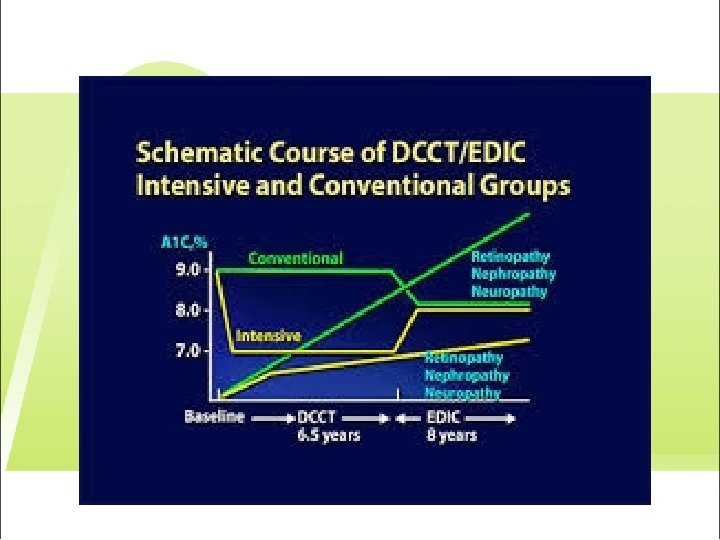
Introduction § Better glycemic control leads to reduction in development and progression of long term diabetes complications. § T 1 DM § T 2 DM
DCCT/EDIC study in T 1 DM Microvascular complications % of patients who progressed 18 * p=0. 006 ** p=0. 002 *** p<0. 001 *66% 16 Conventional 14 Intensive 12 10 8 **53% ***76% ***74% ***77% ***86% 6 4 2 0 e py ia ion thy ma ativ era a e r ess thy inur h r p d e t f m g i o e r l u o n o e o i r a t r alb lar Las ep p inop e nonp r worse tive re icro acu M a M 3 -st no ret r r o e e Sev opathy rolif P from retin DCCT/EDIC Group. JAMA 2002; 287: 2563 A i lbum ia nur
DCCT/EDIC study in T 1 DM Macrovascular complications (any predefined CV outcome) Cumulative incidence Intensive treatment reduced CV risk by 42% (p=0. 02) 10% decrease in Hb. A 1 c= 20% reduction in CV events (p=0. 01) 0. 12 Conventional 0. 10 0. 08 Intensive 0. 06 0. 04 0. 02 0. 00 0 2 Number at risk Intensive treatment Conventional treatment 4 6 8 10 12 14 Years since entry 705 714 683 688 16 629 618 Nathan. N Engl J Med 2005; 353: 2643– 53. 18 20 113 92
Kumamoto study in T 2 DM Microvascular complications Primary prevention cohort 7 Event rate 6 68% Conventional Intensive 74% 5 4 3 2 100% 1 0 h h ed 4 n i 4 2 / 2 g sta y g/ m m su ath 0 00 p op 3 3 e t > > -s tin E E A A >2 re U U Shichiri. Diabetes Care 2000; 23 (Suppl. 2): B 21– 9
UKPDS in T 2 DM Macrovascular complications s nt ete i o b -p dia d en to d y An late re d I an l M l ta ata Fa n-f no ke tro d an l s l ta ata Fa n-f no or D n io PV at m t pu fro m A ath de rt a He 0 Decrease in risk per 1% reduction in Hb. A 1 c 5 10 15 20 25 30 p<0. 0001 21% p<0. 0001 14% p=0. 035 12% p=0. 021 16% 35 40 45 50 p<0. 0001 43% p-value reflects contribution of glycaemia to multivariate model Stratton. BMJ 2000; 321: 405– 412 e r lu i fa
Hb A 1 c as indicator of Glycemic control § Estimation of mean blood glucose during recent 6 -12 weeks § Preprandial § post prandial
Relative contribution of FBG & PPBG to Hb. A 1 c Relative contribution of FBG vs PPBG (%) The relative contribution of PPBG is predominant in subjects with moderate diabetes, whereas the contribution of FBG increases as diabetes worsens. 60 Postprandial Fasting 40 20 0 <7. 3– 8. 4 8. 5– 9. 2 9. 3– 10. 2 Hb. A 1 c (%) Monnier L, et al. Diabetes Care 2003; 26: 881– 5. >10. 2
Why Prandial (SA) Insulin?
Objectives of insulin therapy § The primary objective of insulin therapy is to mimick normal insulin profile § Combinations of ‘basal’ and ‘prandial’ insulins in a ‘basal– bolus’ insulin regimen are normally administered to individuals with T 1 DM or advanced T 2 DM. § Multiple Daily Injection
Ideal Insulin Replacement Therapy in Diabetes Combinations of ‘basal’ and ‘prandial’ insulin in a ‘basal–bolus’ insulin regimen are essential to maintain glycemic control Insulin (m. U/l) Endogenous insulin secretion 45 Breakfast Lunch Dinner Ideal basal insulin Ideal prandial insulin 30 15 0 06. 00 12. 00 18. 00 Time (hours) 24. 00 Kruszynska YT, et al. Diabetologia 1987; 30: 16– 21. 06. 00
Which Prandial Insulin?
Different Types of Prandial Insulins § Human Regular Insulin (HRI) § Rapid acting analogues ü Insulin Lispro (LIS) ü Insulin Aspart (ASP) ü Insulin Glulisine (GLU)
Pharmacokinetic Properties of HRI Human Regular (unmodified) Insulin § Onset of action: 0. 5 -1 hr § Peak activity: 2 -4 hrs § Duration of activity: 6 -8 hrs Med Clin North Am 1998
Human Regular Insulin (HRI) § After SQ injection HRI tends to dissociate from its normal hexameric form, first into dimers and then monomers. ü Only dimeric & monomeric forms can pass through the endothelium. § The resulting delay in the onset and duration of action, limits effectiveness in controlling postprandial glucose. § Dose dependent pharmacokinetics, pharmacokinetics with prolonged onset, peak, duration of action with higher doses Med Clin North Am 1998
Limitations of HRI § Slow onset of action § Requires administration 30– 45 min before a meal § Dose dependent pharmacokinetics § Mismatch between injection and postprandial peak § Risk of interprandial hypoglycaemia Wittlin SD, et al. In: Leahy JL, Cefalu WT, eds. Insulin Therapy: 2002: 73– 85.
Short acting insulin analog
Structure of insulin aspart molecule Insulin aspart is a biosynthetically modified analogue of human insulin A single proline amino acid at position 28 of the insulin B-chain has been replaced with an aspartic acid residue In all other respects, insulin aspart and human insulin are structurally identical • Asp
Molecular structure of insulin GLU (Apidra®) A chain Gly S 1 S Gln Lys Phe 1 Cys 5 S Asn B chain His S Ile Gln 10 15 Pro Lys Thr 25 Gly 20 Leu = substitution 15 Qualitative composition Zinc-free formulation RHI LIS ASP GLU complexing agent x x --- Polysorbate 20 stabilising agent --- x ---- x Trometamol buffering agent --- --- x Components Function Zinc 30 Phe S His Human 3 BLys-29 BGlu-insulin Glu 20 S 5 10 Ala Becker RH. Diabetes Technol Ther 2007; 9: 109– 21.
RA-insulins uptake from subcutaneous tissue T T T T R-format Hexamers T-format Dimer No added zinc Polysorbate 20 (Tween 20) Capillary Brange J, et al. Diabetes Care 1990: 13; 923– 54. Becker RH. Diabetes Technol Ther 2007; 9: 109– 21. T T Phenol T T ( ) T T ) Zn 2+ atoms T T RA-insulin analogue: GLU T T T Phenolic residues ( Structures T T RA-insulin analogues: LIS ASP Zn 2+ T Monomer
Dissociation of insulin after subcutaneous injection • Subcutaneous tissue • Molar concentration (Mol/l) • Diffusion • Capillary membrane • Adapted from Brange et al. Diabetes Care 1990; 13: 923 -54
Rapid Analogues Insulin vs. Regular Insulin Onset Peak Duration Rapid-acting insulin analogues • Insulin aspart • Insulin glulisine • Insulin lispro 5 - 15 min 1 -2 h 3 -4 h Short-acting insulin • Insulin regular 30 - 60 min 2 -4 h 6 -8 h
Pharmacodynamic profile of insulin aspart in healthy subjects • 16 • 15 • Regular human insulin 6 IU • 14 • Regular human insulin 12 IU • 13 • Regular human insulin 24 IU • GIR (mg/kg/min) • 12 • Insulin aspart 6 U • 11 • At all doses the early pharmacodynamic activity of insulin aspart was higher than with regular human insulin • Insulin aspart was associated with significantly less late pharmacodynamic activity (represented by AUCGIR 6 -12 h and AUCGIR 4 -12 h) and a shorter tail than regular human insulin • Insulin aspart provides comparable overall pharmacodynamic activity to regular human insulin • Insulin aspart 12 U • 10 • Insulin aspart 24 U • 9 • 8 • 7 • 6 • 5 • 4 • 3 • 2 • 1 • 0 • 2 • 4 • 6 • 8 • Time from dosing (hours) • Nosek et al. Diabetes Obes Metab 2013; 15: 77– 83 • 10 • 12
GLU vs. HRI in T 1 DM More Rapid Absorption 160 Insulin glulisine Insulin (µU/ml) 140 RHI 120 INS-AUC 2 h; p<0. 05 vs. HRI 100 80 0. 3 U/kg 0. 15 U/kg 0. 075 U/kg 60 40 N=18 T 1 DM subjects 20 0 0 2 4 6 Time (hours) 8 10 INS-AUC= insulin infusion rate - area under the curve Becker RH, et al. Diabetes Care, published online August 3, 2007.
GLU vs. HRI in T 2 DM longer pre- and post-meal dosing window Insulin GLU with a full 35 minutes dosing window offers flexibility tailored to fit a patient’s lifestyle.
Clinical study
Asparte vs. HRI
Similar glucose excursions for post-meal insulin aspart and pre-meal human insulin in T 1 DM • Plasma glucose (mmol/L) • 15 • 14 • HI(– 15 min) • 13 • HI(0 min) • 12 • Insulin aspart (0 min) • 11 • Insulin aspart (+15 min) • 10 • n=20 • 9 • 8 • 7 • 6 • 0 • – 30 • Test meal • Brunner et al. Diabet Med 2000; 17: 371– 5 • 60 • 90 • 120 • 150 • 180 • 210 • 240 • 270 • Randomised, double-blind, double-dummy, four-period crossover study, 20 patients with type 1 diabetes
Glulisine vs. HRI Pharmacodynamic & Efficacy
GLU vs. HRI in T 1 DM Significantly greater improvement in PPBG & Hb. A 1 c N=860 with T 1 DM; insulin glargine=basal insulin Pre-meal insulin glulisine Post-meal insulin glulisine Pre-meal RHI 180 162 144 * * po 7. 7 7. 5 7. 4 * * 7. 3 *p<0. 01 vs RHI and post-meal insulin glulisine tim e 7. 6 ed B st -d in ne r er in n ch ed 2 h Pr un ch 2 - h po st -l lu n st e- Pr ak fa re -b st po 2 h Pr e- br ea k fa s t 126 Pre-meal insulin glulisine Post-meal insulin glulisine Pre-meal RHI 7. 8 Mean Hb. A 1 c (%) Blood glucose (mg/d. L) Seven-point SMBG profile at study endpoint 7. 2 Baseline *p=0. 0001 vs RHI p<0. 05 vs post-meal insulin glulisine Garg SK, et al. Endocr Pract 2005; 11: 11– 7. Week 8 Week 12
GLU vs. HRI in T 2 DM Significantly greater improvement in Hb. A 1 c 7. 6 7. 5 Insulin glulisine RHI Hb. A 1 c (%) 7. 4 7. 3 N=876 with. T 2 DM 7. 2 NPH=basal insulin 7. 1 BMI=34. 5 kg/m 2 * 7. 0 6. 9 Baseline * 12 weeks *p<0. 05 26 weeks Similar incidence of symptomatic hypoglycaemia Dailey G, et al. Diabetes Care 2004; 27: 2363– 8.
Methods: Patients previously on >6 months’ continuous insulin treatment aged 18 years in a randomized, multinational, controlled, open-label, parallel group, 26 -week study received twice-daily NPH insulin and either glulisine (0– 15 min before breakfast and dinner; n = 448) or RHI (30– 45 min before breakfast and dinner; n = 442) at least twice daily.
ØPostprandially, glulisine lowered plasma glucose significantly more versus RHI at 2 h (14. 14 mmol/L versus 15. 28 mmol/L; p = 0. 0025) and excursions at 1 h (3. 99 versus 4. 59; p = 0. 0151) and 2 h (4. 87 versus 6. 03; p = 0. 0002). Ø No between-group differences occurred in the frequencies and monthly rates of all symptomatic hypoglycaemia; v Nocturnal hypoglycaemia from Month 4 to treatment end was less frequent with glulisine versus RHI (9. 1% versus 14. 5%; p = 0. 029).
GLU vs. HRI in T 2 DM Significantly less nocturnal hypoglycemia Insulin GLU helps physicians reassure their patients around hypoglycemia. Rayman G, et al. Diabetes Res Clin Pract 2007; 76(2): 304 -312.
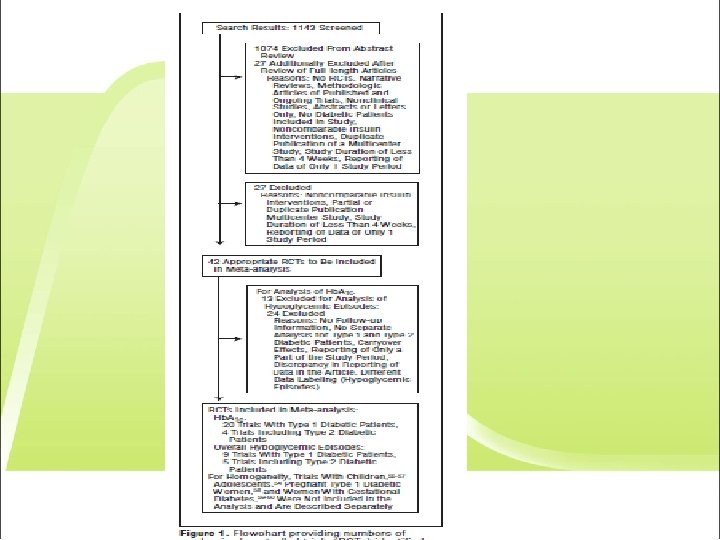
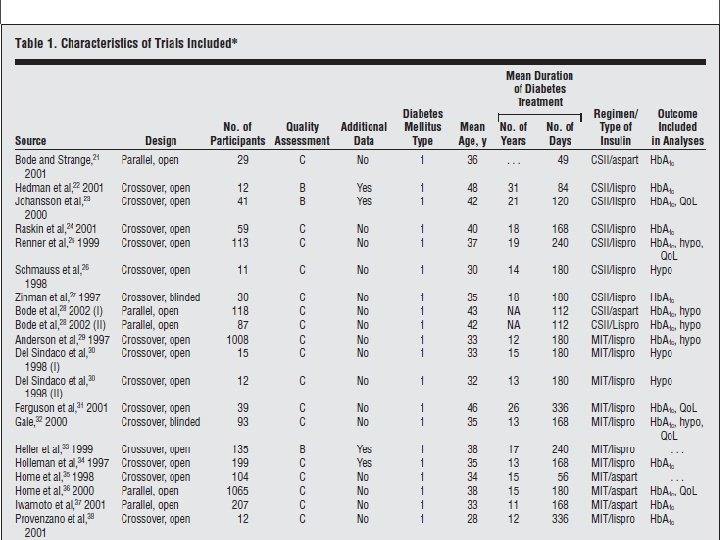
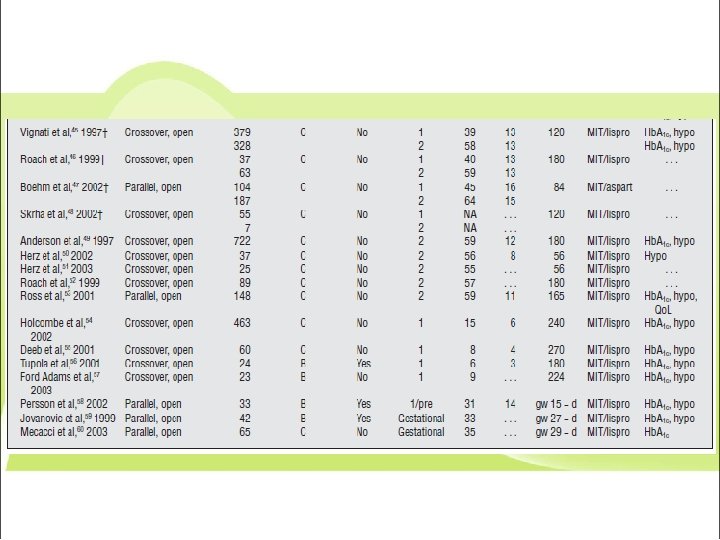
Methods: Electronic searches (Cochrane Library, MEDLINE, and EMBASE) and additional searching (pharmaceutical companies, experts, approval agencies, abstracts of diabetology meetings) were performed. Two reviewers independently screened randomized controlled trials to determine inclusion ARCH INTERN MED/VOL 165, JUNE 27, 2005
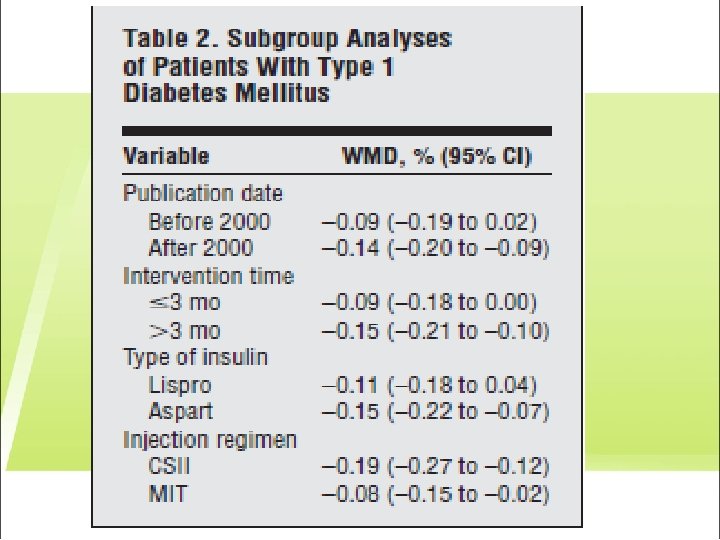
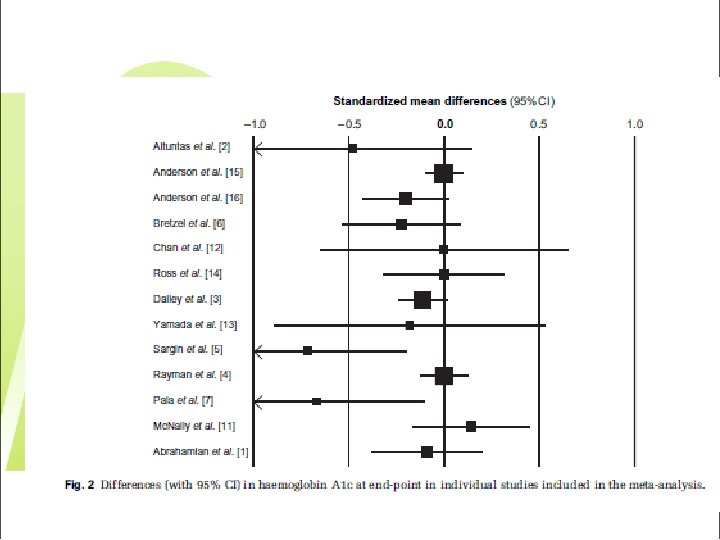
Differences in hemoglobin A 1 c (Hb. A 1 c) values
Differences in overall hypoglycemic event rate.
Conclusion: Our analysis suggests only a minor benefit to hemoglobin A 1 c values in adult patients with type 1 diabetes mellitus but no benefit in the remaining population with type 2 or gestational diabetes from SAI analogue treatment.
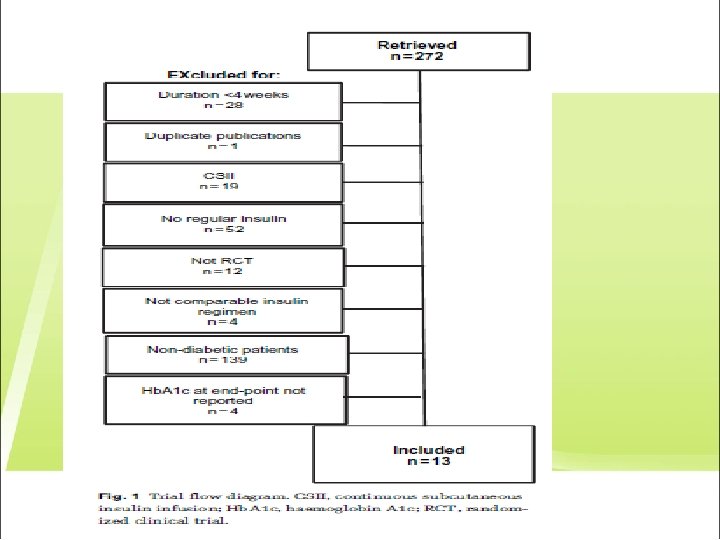
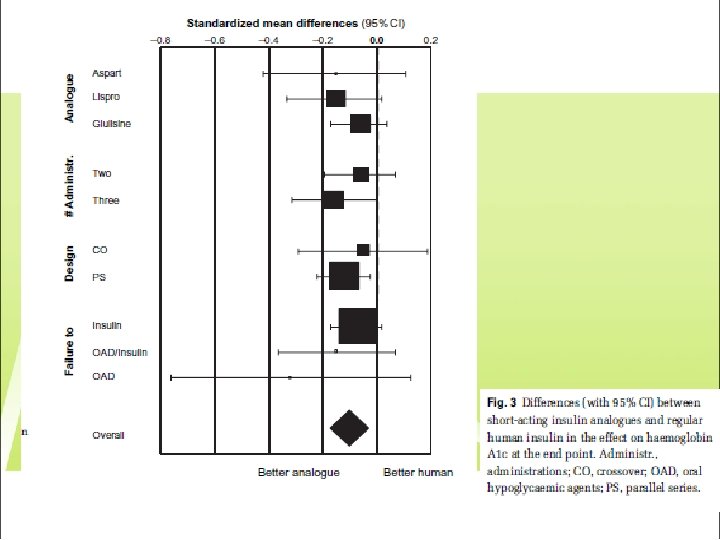
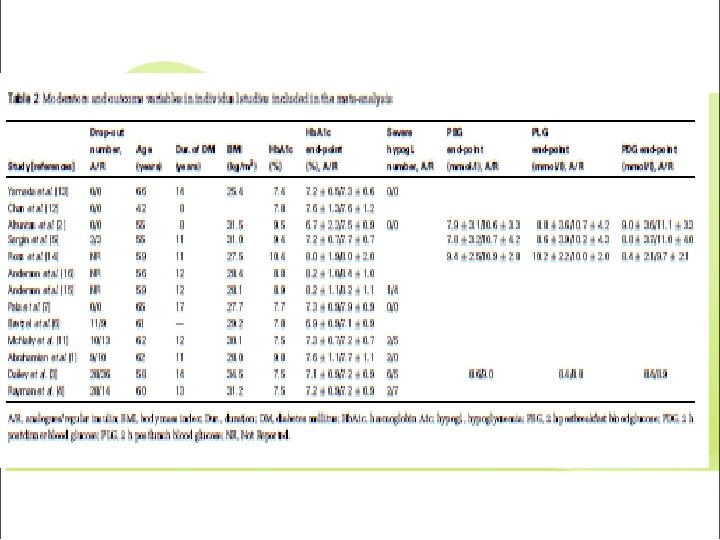
Method: All randomized controlled trials (RCTs) with a duration >4 weeks comparing short-acting insulin analogues (lispro, aspart or glulisine) with HRI in type 2 diabetic patients were retrieved; data on Hb. A 1 c and postprandial glucose et end-point and incidence of severe hypoglycaemia were extracted and meta-analysed. • Diabetes, Obesity and Metabolism, 11, 2009, 53– 59
Hypoglycemia: The number of patients experiencing at least one episode of severe hypoglycaemia (13 and 21 for short-acting analogues and regular human insulin, respectively) was reported in five trials only [1, 3, 4, 11, 15]. Combining those studies, the MH-OR for this event with short-acting analogues, in comparison with human insulin, was 0. 61 (0. 25– 1. 45).
Method: Data on severe hypoglycaemia (number of patients with at least one event) were extracted, while mild hypoglycaemic episodes were not considered because of the heterogeneity of diagnostic definitions across trials.
Conclusion: In type 2 diabetic patients, short-acting insulin analogues provide a better control of Hb. A 1 c and postprandial glucose than regular human insulin, without any significant reduction of the risk of severe hypoglycaemia.
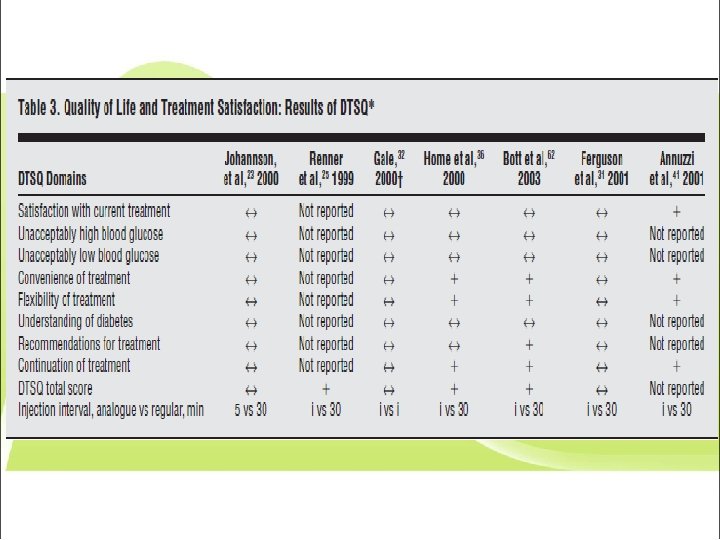
Take Home Message ØIn comparisons between different type of short insulin especially human and analog: ØGlycemic control: Ø Minor benefit/ No clinically important difference ØHypoglycemic episodes Ø No difference ØQuality of life and treatment satisfaction Ø In favor of analouges (due to flexibility
Different Types of Prandial Insulins § Human Regular Insulin (HRI) § Rapid acting analogues ü Insulin Lispro (LIS) ü Insulin Aspart (ASP) ü Insulin Glulisine (GLU)
Take Home Message Insulin treatment has always been as much an art as a science. § The proper use of insulin analogues allows people with diabetes greater flexibility in the timing of meals, snacks, and exercise, which in turn enhances their ability to lead normal lives. § When choosing between insulin analogues and HRI, not only should their differences in glycemic control and treatment flexibility be considered, but also their cost of treatment, type of diet and patients’ preferences.
Thanks for your attention
Pharmacokinetics (serum insulin levels) after subcutaneous (sc) injection of analog insulins
Meal-time glucose excursions for insulin lispro, insulin aspart and insulin glulisine when compared separately in people with type 1 diabetes with unmodified human insulin
Insulin aspart: rapid dissociation into monomers • B 29 Lys • B 21’ Glu • B 30 Thr • B 22’ Arg • B 28 Pro/Asp • 3. 7 Å • B 23’ Gly • B 27 Thr • Hexamer • Dimer • Reproduced with permission from Brange J, Vølund A. Adv Drug Delivery Rev 1999; 35: 307– 35. • Monomer
Glulisine in Special Population
Journal of Renal Nutrition, 2014
GLU vs. HRI in T 2 DM and Severe Renal Insufficiency Journal of Renal Nutrition, 2014
GLU vs. HRI in T 2 DM and Severe Renal Insufficiency Journal of Renal Nutrition, 2014
GLU vs. HRI in T 2 DM and Severe Renal Insufficiency Journal of Renal Nutrition, 2014
• Glulisine vs. Aspart
Insulin GLU vs. insulin ASP Earlier effect on postprandial glucose levels Apidra® reduces blood glucose levels more rapidly vs. insulin Aspart. Boli GB, et al. Diabetes Obes Metab 2011; 13: 251 -257.
Insulin GLU vs. insulin ASP Longer dosing window Apidra® offers flexibility tailored to fit a patient’s lifestyle.
Urakami T, et al. J Diabetes Investig. 2015; 6(1): 87– 90.
Switching from other RA-insulin analogs to Gl. U in T 1 DM Measurements: Study population: §N=26 T 1 DM Japanese children aged 12. 5 ± 5. 5 yrs §Basal–bolus insulin therapy: §∆ mean SMBG just before, and 1– 1. 5 h after breakfast and supper ü 18 MDI, 8 CSII üASP or LIS as bolus insulin üGlargine as basal insulin for MDI üfor the 1 -month period at baseline, and at 6 months after using GLU. §None were obese §none had vascular complications or metabolic-syndrome factors. Protocol §∆ Hb. A 1 c, frequency of hypoglycemia , % overweight & daily insulin requirement for the same time periods. §ASP or LIS was switched to GLU §Glargine was continued as before Urakami T, et al. J Diabetes Investig. 2015 Jan; 6(1): 87– 90.
Switching from LIS or ASP to Gl. U in T 1 DM EFFICACY Urakami T, et al. J Diabetes Investig. 2015; 6(1): 87– 90.
Switching from LIS or ASP to Gl. U in T 1 DM SAFETY Urakami T, et al. J Diabetes Investig. 2015; 6(1): 87– 90.
How to use Glulisine?
The most precise and flexible prandial coverage is possible with “basal-plus/bolus” therapy Hb. A 1 c > target FPG on target PPG > target Hb. A 1 c > target FBG > target Basal insulin Basal plus Basal bolus Basal plus Basal + 2 prandial Basal + 1 prandial once daily (treat-to-target) Lifestyle ± Metformin ± 2 nd/3 rd Drug Hb. A 1 c > target Progressive deterioration of -cell function Raccah et al. Diabetes Metab Res Rev 2007; 23: 257. Basal + 3 prandial
Dosing and Titration • 80
Summary: GLU vs. RHI Apidra® is rapidly absorbed and has a faster onset of action than RHI. Apidra® has a longer defined dosing window vs. RHI- a full 35 minutes. Apidra® is associated with less nocturnal hypoglycemia in people with T 2 DM compared with RHI. Apidra® is associated with reduced incidence of cardiovascular complications in people with T 2 DM vs. RHI in clinical practice. • 81
Summary: GLU vs. ASP Apidra® has an earlier effect on postprandial glucose levels than insulin Aspart. Apidra® provides equal efficacy and safety, whether it is administered pre- or post-meal. • 82
® Apidra is an ideal partner for Lantus ®