RADIOTHERAPY IN BREAST CANCER PART 1 CONSERVATION GNTHER
 GÜNTHER GRUBER Institut für Radio-Onkologie guenther. gruber")
RADIOTHERAPY IN BREAST CANCER (PART 1: CONSERVATION) GÜNTHER GRUBER Institut für Radio-Onkologie guenther. gruber @ ksa. ch

AIMS OF RT • Breast conservation • Local control • Overall survival • Reduction of side effects
 • RT after mastectomy • Complications • New")
TOPICS • Breast conserving therapy (BCT) • RT after mastectomy • Complications • New trends

BREAST CONSERVATION NON-INVASIVE CANCER RT in LCIS ?
 contralateral")
BREAST CONSERVATION NON-INVASIVE CANCER RT in LCIS ? ÞNo solid data multicentricity (-88%) contralateral pos. biopsies (-59%) 10 -35% progression to invasive cancer after 20 – 25 years follow-up

BREAST CONSERVATION NON-INVASIVE CANCER RT in DCIS ?

BREAST CONSERVATION NON-INVASIVE CANCER RT in DCIS ? Omission of RT ?

BREAST CONSERVATION DCIS Omission of RT after breast conserving surgery for DCIS low risk = Diagnosis 2002 SEER data; Katz et al. ; J Clin Oncol, 2005 G 1, up to 2 cm G 2, up to 1 cm high risk = > 2 cm or G 3

BREAST CONSERVATION DCIS VAN NUYS PROGNOSTIC INDEX SIZE -15 mm 16 -40 mm >40 mm G low w/o necrosis low with necrosis high RR 10+mm 1 -9 mm <1 mm New: AGE >60 yrs 40 – 60 yrs <40 yrs 1 2 3

BREAST CONSERVATION DCIS LOCAL CONTROL: Multivariate analysis Silverstein, 2002 G Van Nuys series Age Size RR

BREAST CONSERVATION DCIS Prospective study for omission of RT in ‚good risk‘ (mammo-2. 5 cm; G 1/2; RR 10+mm) 12 % LR at 5 years ! Stopped early with 158 pts (/200) J Wong et al. , J Clin Oncol 2006

BREAST CONSERVATION DCIS Omission of RT in ‚good risk‘ tamoxifen RTOG 9804 tamoxifen + RT

BREAST CONSERVATION DCIS LOCAL CONTROL: Multivariate analysis Silverstein, 2002 RT G Van Nuys series Age Size RR

Randomised studies in DCIS with or without radiotherapy Local control – Efficacy of RT Trial n f-up Op Op+RT HR p NSABP B 17 818 5 yr 16% 7% 0. 43 <0. 001 EORTC 10853 1010 10 yr 26% 15% 0. 53 <0. 0001 UKCCCR 1701 5 yr 14% 6% 0. 38 <0. 001 Risk reduction in all subgroups (to various degrees) RT with 50 Gy => As expected: no difference in overall survival!

Randomised studies in DCIS with or without radiotherapy Local control – Efficacy of RT

BREAST CONSERVATION DCIS – Impact of boost?
 Omlin et")
BREAST CONSERVATION DCIS – Impact of boost? …in young women (-45 years) Omlin et al. Lancet Oncol, 2006 median: 60 Gy (± 1) median 60 Gy (± 1) median: 50 Gy median 50 Gy (± 1) keine RT
 Gruber et")
BREAST CONSERVATION DCIS – Impact of boost? …in young women (-45 years) Gruber et al. , unpublished median: 60 Gy (± 1) Mastectomy median: 50 Gy (± 1) no RT

BREAST CONSERVATION For which pts. with DCIS radiotherapy can be omitted after breast conserving surgery? Evidence-based medicine (3 published studies + 1 as abstract): NO OMISSION OF RT! Probably yes: clinging or micropapillary growth? ; RR ≥ 10 mm? (CAVE: young patients! VAN NUYS: >=10 mm; <40 yrs: n=15!) Interdisciplinarity is very important !

BREAST CONSERVATION INVASIVE CANCER • BCT vs mastectomy ?
 20 yrs – Results p=0.")
BREAST CONSERVATION % Milan I Trial (Mastectomy vs BCT) 20 yrs – Results p=0. 8 p=1. 0 Veronesi et al. , NEJM 2002
 20 yrs – Results p=0. 95")
BREAST CONSERVATION % NSABP-06 Trial (Mastectomy vs BCT) 20 yrs – Results p=0. 95 p=0. 74 Fisher et al. , NEJM 2002

BREAST CONSERVATION CONCLUSION • BCT + Mastectomy equivalent !

BREAST CONSERVATION INVASIVE CANCER • BCT vs mastectomy ? • Breast conserving surgery: Omission of RT ?

BREAST CONSERVATION Local relapse: BC surgery +/- RT Studies Median Follow-up NSABP B-06 125 months Scottish Cancer Trial 68 months UppsalaÖrebro Study Group 106 months Ontario Cancer Inst. Milano III Op LR w/o RT LR with RT Lumpectomy Segmentectomy 35% 9% 24% 6% 22% 7% 91 months Lumpectomy 35% 11% 109 months Quadrantectomy 22% 5%

BREAST CONSERVATION EBCTCG 2000 RT metaanalysis, Lancet 12/05 % N 0 N+/N? n=6097 n=1214 p<0. 00001 p=0. 006 p<0. 00001 p<0. 01

BREAST CONSERVATION

BREAST CONSERVATION CONCLUSION • BCT + Mastectomy equivalent ! • BC surgery: No omission of RT !

BREAST CONSERVATION INVASIVE CANCER • BCT vs mastectomy ? • Breast conserving surgery: Omission of RT ? • Omission of RT in ‚low risk‘ ?

BREAST CONSERVATION BC surgery +/- RT Swedish Breast Cancer Group, EJC 2003 median tu-size: 12 mm; n=1187; median F-up: 8 J 14% 4%

BREAST CONSERVATION BC surgery +/- RT, p. T 1 a/p. T 1 b p. N 0 16. 5 p<0. 0001 9. 3 p=0. 01 2. 8 NSABP B-21, n=1009; JCO 2002

BREAST CONSERVATION Local relapse rates, p. T 1 a/p. T 1 b p. N 0 Age 70+ ? Therapy, -ies n LR TAM RT TAM+RT 43 59 57 3 (7%) 5 (8%) 0 RT vs. TAM => HR 1. 06 (0. 25 -4. 46) ! NSABP B-21, n=1009 JCO, 2002
, >70")
BREAST CONSERVATION … in T 1, N 0, R 0, ER+ (in 97%), >70 yrs CALGB, RTOG, ECOG (Hughes et al. NEJM, 9/2004) n=636 (75+ years: 55%) median F-up: 5 J LOCAL RELAPSE with tamoxifen and RT 4% 1% p<0. 001
")
BREAST CONSERVATION T 1/T 2, >50 yrs: 769 randomised (of 1572 ‚eligible‘ pts. ) 5 yrs LR -2 cm, R 0, HR+ n=611 Tam + WB-RT 3. 2% 0. 4% (p<0. 001) -1 cm, R 0, HR+ n=263 Tam + WB-RT Files et al. , NEJM 2004 2. 6% 0% (p=0. 02)
")
BREAST CONSERVATION T 1/T 2, >50 yrs: 769 randomised (of 1572 ‚eligible‘ pts. ) 5 yrs LR + 3 J -2 cm, R 0, HR+ n=611 Tam + WB-RT x 5! 3. 2% 0. 4% (p<0. 001) -1 cm, R 0, HR+ n=263 Tam + WB-RT Files et al. , NEJM 2004 8 yrs LR 2. 6% 0% (p=0. 02) 15. 2% 3. 6%
")
BREAST CONSERVATION T 1/T 2, >50 yrs: 769 randomised (of 1572 ‚eligible‘ pts. ) 5 yrs LR + 3 J -2 cm, R 0, HR+ n=611 Tam + WB-RT x 5! 3. 2% 0. 4% (p<0. 001) -1 cm, R 0, HR+ n=263 Tam + WB-RT Files et al. , NEJM 2004 8 yrs LR 2. 6% 0% (p=0. 02) (B 21) 15. 2% (16. 5%) 3. 6% ( 2. 8%)

BREAST CONSERVATION postmenop. , T <3 cm, N 0, ER+ and/or PR+ ABCSG 8 (8 A) (Pötter et al. ASTRO, OEGRO, ECCO 13, 11/2005) n=826 (60+ years: about two thirds) median F-up: 42 mo LOCAL RELAPSE 5 yrs with Tamoxifen/AI and RT 4. 5% 0. 6% p=0. 001

BREAST CONSERVATION „low risk“ – studies summary Follow up still too short ! No subgroup of pts. which does not profit from RT! IMPORTANT: Trade-offs ! If overall survival > 5 yrs: RT !

BREAST CONSERVATION CONCLUSION • BCT + Mastectomy equivalent ! • BC surgery: No omission of RT ! • No omission of RT in ‚low risk‘ !

BREAST CONSERVATION INVASIVE CANCER • BCT vs mastectomy ? • Breast conserving surgery: Omission of RT ? • Omission of RT in ‚low risk‘ ? • PBI for ‚low risk‘ ?

BREAST CONSERVATION

BREAST CONSERVATION RATIONALE for PBI small RT volume offers the possibility for higher single doses => Shorter treatment time (4 -5 days vs 5 weeks) Socio-economic aspects small RT volume has likely less long-term complications RT of whole breast necessary ?

BREAST CONSERVATION PROBLEMS for PBI ‚ Never change a winning team ! ‘ (whole breast irradiation) Less experience ! Target volume ? Residual tumor cells ? Patient selection ?

BREAST CONSERVATION Local relapse out of ‚tu bearing quadrant‘ RANDOMISED STUDIES TRIAL NSABP-B 06 MAILAND UPPSALA ONTARIO f-up 125 39 64 43 Modified after Baglan et al. , 2001 OP 2. 7% 1. 5% 3. 5% OP+RT 3. 8% 0% 1. 0%

BREAST CONSERVATION Intraoperative Radiotherapy in Phase III
 in Phase III Most data in the literature")
BREAST CONSERVATION Interstitial Brachytherapy (i. BT) in Phase III Most data in the literature are based on i. BT !

BREAST CONSERVATION
 in Phase III In USA very frequent !")
BREAST CONSERVATION Brachytherapy-Ballon (Mammosite ®) in Phase III In USA very frequent !
 Registry Trial; n=1449; Median f-up: 14 mo 2 yrs")
BREAST CONSERVATION Brachytherapy-Ballon (Mammosite ®) Registry Trial; n=1449; Median f-up: 14 mo 2 yrs local failure: 1. 2% (isolated LF 0. 8%) 2 yrs axillary failure: 1. 0% (isolated AF 0. 6%) Good/excellent cosmesis 6 mo 12 mo 18 mo 24 mo 95. 1% 93. 7% 91. 3% 93. 5% Vicini F et al. ASCO; 2006 36 mo 90. 4%
 percutaneous RT in Phase III Few data !")
BREAST CONSERVATION 3 D (IMRT; protons) percutaneous RT in Phase III Few data !
, f-up: 65")
BREAST CONSERVATION PBI only William Beaumont Hospital n=199 (92% p. T 1), f-up: 65 mo HDR: 32 Gy / 8 fx / 4 d LDR: 50 Gy, 0. 52 Gy/h, 96 h actuarial LR (5 J) WB-RT: 1% PBI as good as WB-RT ! Vicini et al. , 2003
; 1982 -87; n = 708; Breast")
BREAST CONSERVATION PBI only Manchester Trial (Phase III); 1982 -87; n = 708; Breast + LN (4 MV; 40 Gy/15 fx) 11% Randomisation LOCAL REL. PBI (10 Me. V; 40 -42. 5 Gy/8 fx) 20% • no axillary diss. • no systemic therapy • no microscopic resection margin determination • in 42% no Tumor size determination
 no standard ! Phase III")
BREAST CONSERVATION „low risk“ – PBI? Summary (So far) no standard ! Phase III studies ongoing ! Anyway, only for ‚low risk‘ ! Expertise ?

BREAST CONSERVATION CONCLUSION • BCT + Mastectomy equivalent ! • BC surgery: No omission of RT ! • No omission of RT in ‚low risk‘ ! • The target is the whole breast !

BREAST CONSERVATION INVASIVE CANCER • BCT vs mastectomy ? • Breast conserving surgery: Omission of RT ? • Omission of RT in ‚low risk‘ ? • PBI for ‚low risk‘ ? • Altered fractionation?

BREAST CONSERVATION altered fractionation Stage I/II n=1234 R 42. 5 Gy/2. 65 Gy 22 days n=622 50 Gy/2 Gy 35 days n=612 median f-up : 69 months Whelan et al. , JNCI 94, 2002

BREAST CONSERVATION altered fractionation LRFS 100% 95% Whelan et al. , JNCI 94, 2002 DFS

BREAST CONSERVATION altered fractionation T 1 -3 N 0 -1 n=1410 R 42. 9 Gy/3. 3 Gy 5 wks n=466 39 Gy/3 Gy 5 wks n=474 median f-up : 9. 7 years Owen et al. , Lancet Oncol, 2006 50 Gy/2 Gy 5 wks n=470

BREAST CONSERVATION altered fractionation Owen et al. , Lancet Oncol, 2006

BREAST CONSERVATION altered fractionation HR LR 5 yrs 10 yrs 50 Gy 1 7. 9% 12. 1% 42. 9 Gy 0. 86 7. 1% 9. 6% 39 Gy 1. 33 9. 1% 14. 8% => alpha/beta is 4 (95%CI 1 -7. 8); 41. 6 Gy/3. 2 Gy = 50 Gy/2 Gy! Owen et al. , Lancet Oncol, 2006

BREAST CONSERVATION CONCLUSION • BCT + Mastectomy equivalent ! • BC surgery: No omission of RT ! • No omission of RT in ‚low risk‘ ! • The target is the whole breast ! • There are equivalent schedules !

BREAST CONSERVATION INVASIVE CANCER • BCT vs mastectomy ? • Breast conserving surgery: Omission of RT ? • Omission of RT in ‚low risk‘ ? • PBI for ‚low risk‘ ? • Altered fractionation? • Increase of dose (boost) ?

BREAST CONSERVATION Local recurrences after BCS + RT BOOST versus NO BOOST no boost H. R. • Lyon 5 y 4. 5 % 3. 6 % (10 Gy) 0. 80 p = 0. 044 n = 1024 • French M. C. 5 y 6. 8 % 3. 6 % (16 Gy) 0. 53 p = 0. 13 n = 664 • EORTC 10801 5 y 6. 8 % n = 5569 3. 4 % (15 Gy) 0. 59 p = 0. 0001
 p=0. 002 51 -60 J")
BREAST CONSERVATION BREAST-RT +/- BOOST - 40 J (n=449) p=0. 002 51 -60 J (n=1803) p=0. 07 Bartelink et al. , NEJM 2001 41 -50 J (n=1334) p=0. 02 > 60 J (n=1732) p=0. 11

BREAST CONSERVATION Breast pain – randomised study p<0. 01 * RT * no RT Whelan et al. , Cancer 2000

BREAST CONSERVATION Skin reactions – randomised study p<0. 01 * RT * no RT Whelan et al. , Cancer 2000

BREAST CONSERVATION Breast cosmesis – randomised study no RT RT Whelan et al. , Cancer 2000

BREAST CONSERVATION Global score by boost treatment 100% 86% 80 71% Excellent/Good 60 Fair/Poor 40 20 29% 14% 0 No boost Boost

BREAST CONSERVATION

BREAST CONSERVATION CONCLUSION • BCT + Mastectomy equivalent ! • BC surgery: No omission of RT ! • No omission of RT in ‚low risk‘ ! • The target is the whole breast ! • There are equivalent schedules ! • Boost efficient (! <50 yrs !)

RT – BREAST CANCER ‚TIMING‘

RT – BREAST CANCER ‚TIMING‘

RT – BREAST CANCER ‚TIMING‘ RT – HT In vitro Ø, Radioresistence , by Tamoxifen In vivo Only 2 studies (Labrie et al. ; Cancer Res. 1999; Int J Cancer 2003)

RT – BREAST CANCER ‚TIMING‘ RT – HT ZR-75 -1 human breast cancer cells (s. c. into nude mice) => average tumor-area 20 mm 2; Strata: tumor size R RT 15 x 2 Gy EM-800 300 ug/d (SERM) 24 mice RT 15 x 2 Gy 24 mice EM-800 300 ug/d (SERM) Day 1 21 156 CR: 62% (arm A) vs. 22% (arm B) ARM A ARM B

RT – BREAST CANCER ‚TIMING‘ RT – Tamoxifen: simultaneous vs sequential Journal of Clinical Oncology, Vol 23, No 1, 2005 * 3 (small) retrospective studies z. B. Ahn et al, 2005 OS LRFS

RT – BREAST CANCER ‚TIMING‘ RT – Tamoxifen: simultaneous vs sequential Lokalrezidiv Bentzen, S. M. et al. JCO; 23: 6266 -6267 2005

RT – BREAST CANCER ‚TIMING‘ RT – 6 x. CMF: ‚RT first‘ vs , CMF first‘ Breast conservation; n=244 DFS No significant difference! Bellon, J. R. et al. JCO; 23: 1934 -1940; 2005

RT – BREAST CANCER ‚TIMING‘ RT – 6 x. CMF: ‚RT first‘ vs , CMF first‘ Breast conservation; n=244 DFS DMFS No significant difference! Bellon, J. R. et al. JCO; 23: 1934 -1940; 2005

RT – BREAST CANCER ‚TIMING‘ RT – 6 x. CMF: ‚RT first‘ vs , CMF first‘ Breast conservation; n=244 DFS DMFS OS No significant difference! Bellon, J. R. et al. JCO; 23: 1934 -1940; 2005

RT – BREAST CANCER ‚TIMING‘ ‚Ch. T => RT‘ vs , sim. Ch. T/RT‘ Ch. T= mitoxantrone, 5 -FU, cyclophosphamide; 6 cycles RT= 50 Gy/2 Gy; +/- boost ARCOSEIN III trial (n=214 for late toxicity) ! No difference in acute toxicity ! (skin, esophagus, infections, neutropenia) ! No statistical difference in grade 2 or higher breast edema, lymphedema, pain ! ! sim. Ch. T/RT: Significant more breast atrophy, subcutaneous fibrosis, teleangiectasia, skin pigmentation ! Toledano et al. ; Int J Radiat Oncol Biol Phys; 2006

RT – BREAST CANCER ‚TIMING‘ RT – Herceptin ®

RT – BREAST CANCER ‚TIMING‘ RT – Herceptin ® N 9831: AC->T->H vs AC->TH->H RT (after BCS or Mx 4+LN sim to H allowed) 1460 available for adverse events analyses median f-up: 1. 5 yrs Skin reaction (p=0. 78); pneumonitis (p=0. 78), dyspnea (p=0. 87) Cough (p=0. 54); dysphagea (p=0. 26); neutropenia (p=0. 16) Þ Concurrent H-RT is not associated with acute RT adverse events Þ Further follow up is needed for late adverse events Halyard MY et al. ASCO; 2006

RT – BREAST CANCER ‚TIMING‘ How to combine RT with systemic therapies ? Individual HT: simultaneous possible Ch. T: In most centers: Ch. T -> RT simultaneous RCh. T possible but more side effects! => Not recommended Herc: simultaneous possible

BREAST CONSERVATION TECHNIQUE / RT APPLICATION

BREAST CONSERVATION

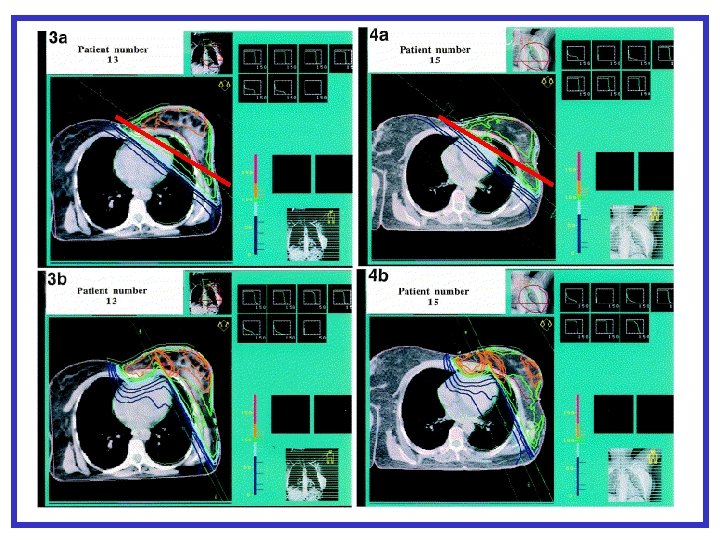
BREAST CONSERVATION Planning-CT and 3 D-Planning

BREAST CONSERVATION

BREAST CONSERVATION

BREAST CONSERVATION Hurkmans et al. , 2001 HEART 42 mm
 Intensity modulated beam (IMB)")
BREAST CONSERVATION IMRT „Open“ homogeneous beam (OB) Intensity modulated beam (IMB)

BREAST CONSERVATION IMRT

BREAST CONSERVATION IMRT

BREAST CONSERVATION IMRT n=306 R Standard 2 D 3 D IMRT 5 yrs – Differences in breast appearence (Photos) 60% 48% p=0. 06 (Qo. L no difference) Yarnold et al. , ECCO 13; 2005

BREAST CONSERVATION 6 MV + 12 e Lomax et al. IMRT Protons IMRT IJROBP 2003

BREAST CONSERVATION ‚Organ‘motion, n=20 ‚motion‘ within 1 fraction: 1. 3 +/- 0. 4 mm ‘motion’ between 2 fractions: 2. 6 +/- 1. 3 mm Kron et al. , ESTRO 2004

BREAST CONSERVATION SCHLUSSFOLGERUNG

RT – BREAST CANCER RE-IRRADIATION
- Slides: 99