Radiology course Abdomen Clinical cases GASTROINTESTINAL Right lower

Radiology course Abdomen Clinical cases GASTROINTESTINAL

Right lower quadrant abdominal pain and fever CASE 1 • Patient presenting with fever and significant tenderness at the right lower quadrant. • Acute abdominal pain • No trauma

Case 1 • First study? – – – X – ray abdomen CT abdomen and pelvis with contrast CT abdomen and pelvis without contrast US abdomen MRI abdomen and pelvis without and with contrast

Right lower quadrant abdominal pain and fever • No free air • No bowel distension • Still pain • Second study? – MRI w/o contrast – US – CT w/o contrast Case courtesy of Dr Jeremy Jones, Radiopaedia. org

Right lower quadrant abdominal pain and fever Abdominal US Case courtesy of Dr M Osama Yonso, Radiopaedia. org

Right lower quadrant abdominal pain and fever Contrast CT Coronal Axial Case courtesy of Jack Ren, Radiopaedia. org

Right lower quadrant abdominal pain and fever

Left lower quadrant abdominal pain CASE 2 • Patient presenting with significant pain at the left lower quadrant. • Acute abdominal pain • No fever

Left lower quadrant abdominal pain • Non-specific bowel gas • No obstruction • No perforation • Second study? – MRI w/o contrast – US – CT w/o contrast Case courtesy of Dr Jeremy Jones, Radiopaedia. org

Left lower quadrant abdominal pain Contrast CT Coronal Axial Case courtesy of Dr Jeremy Jones, Radiopaedia. org

Left lower quadrant abdominal pain MRI T 2 Fat Sat T 1 Case courtesy of Dr Roberto Schubert, Radiopaedia. org

Left lower quadrant abdominal pain

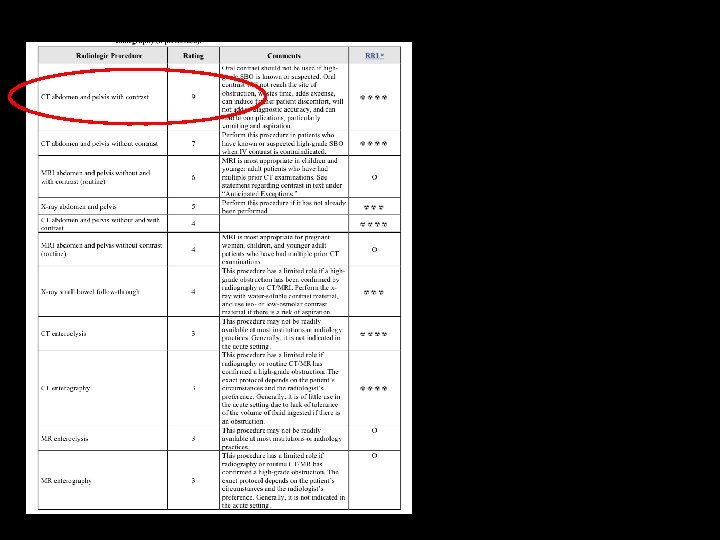
Suspect of Inflammatory Bowel Disease • Patient presenting with chronic pain at the right lower quadrant. • Recurrent diarrhea • Weight loss

Suspect of Inflammatory Bowel Disease • First study? – – – X – ray abdomen CT abdomen and pelvis with contrast CT abdomen and pelvis without contrast US abdomen MRI abdomen and pelvis without and with contrast

Suspect of Inflammatory Bowel Disease
 CT Enterography Coronal Axial Case courtesy of Dr Dalia")
Inflammatory Bowel Disease (Crohn Disease) CT Enterography Coronal Axial Case courtesy of Dr Dalia Ibrahim, Radiopaedia. org

CT Enterography Technique/Procedure Actual procedure will vary depending on institutional protocol/guidelines but this is a typical examination: -Abstain from all food and drink 4 -6 hours before the exam. -Patients drink about 1. 5 - 2 L of oral contrast over 40 -60 minutes before the exam. - Administration of intravenous contrast injection at a rate 4 ml/sec. CT scanning is ideally performed on a multi-detector computed tomography (MDCT) scanner about 45 -65 seconds after contrast material injection in a single (venous) phase with patient in prone position if possible - Data interpretation with the use of axial and coronal reformatted images for proper evaluation.

Crohn Disease MR Enterography Coronal T 1 C+ fat sat Coronal MIP dynamic contrast Case courtesy of Dr Dalia Ibrahim, Radiopaedia. org

Crohn Disease MR Enterography Coronal T 1 C+ fat sat Coronal MIP dynamic contrast Case courtesy of Dr Dalia Ibrahim, Radiopaedia. org

MR Enterography Technique/Procedure Actual procedure will vary depending on institutional protocol/guidelines but this is a typical examination: -patients should abstain from all food and drinks for 4 -6 h prior to the study. -patients drink about 1 -1. 5 L of a 2. 5% mannitol solution at regular intervals over a period of approximately 40 min prior to the study. -this solution acts as a hyperosmolar agent which draw fluid into the bowel and (biphasic) appears as low signal intensity on T 1 -weighted images and high signal intensity on T 2 weighted images. - scanning is ideally performed on a 1. 5 -T MRI scanner, using a phased array surface coil, either in the supine or prone position
 Contrast CT Coronal section Case courtesy of Dr Frank")
Inflammatory Bowel Disease (Ulcerative Colitis) Contrast CT Coronal section Case courtesy of Dr Frank Gaillard, Radiopaedia. org

Ulcerative Colitis Contrast CT Axial Case courtesy of Dr Frank Gaillard, Radiopaedia. org

Inflammatory Bowel Disease Differential Diagnosis - BOWEL INVOLVED CD: small bowel 70 -80%, only 15 -20% have only colonic involvement UC: rectal involvement 95%, with terminal ileum only involved in pancolitis (backwash ileitis) - DISTRIBUTION CD: skip lesions typical UC: continuous disease from rectum up - COLONIC WALL fat halo sign seen in 61% of chronic UC cases, but only in 8% of CD bowel wall is thicker in CD than in UC (when colon involved) serosal surface smooth in UC (95%), irregular in CD (80%) - PERIANAL INVOLVEMENT UC: although rectal involvement is very common, perianal complication are not as frequently seen CD: common, seen in 82% of patients stranding of ischiorectal fossa/perirectal fat (73%) fistulas/sinus tracts (22%) Courtesy of Radiopaedia. org

Right upper quadrant abdominal pain • Patient presenting typical abdominal pain • Increased amylase and lipase • Acute abdominal pain • No trauma

Right upper quadrant abdominal pain • First study? – – – X – ray abdomen CT abdomen and pelvis with contrast CT abdomen and pelvis without contrast US abdomen MRI abdomen and pelvis without and with contrast

Right upper quadrant abdominal pain
 US Power Doppler Case courtesy of Dr")
Right upper quadrant abdominal pain (Acute Pancreatitis) US Power Doppler Case courtesy of Dr Maulik S Patel, Radiopaedia. org
 Contrast CT Case courtesy of Dr Frank")
Right upper quadrant abdominal pain (Acute Pancreatitis) Contrast CT Case courtesy of Dr Frank Gaillard, Radiopaedia. org Case courtesy of Dr Hani Salam, Radiopaedia. org

Acute Pancreatitis MRI Axial Coronal SSH Case courtesy of Dr Hani Salam, Radiopaedia. org

Right upper quadrant abdominal pain • Patient presenting with fever and significant tenderness at the right upper quadrant. • Acute abdominal pain • No trauma

Right upper quadrant abdominal pain • First study? – – – X – ray abdomen CT abdomen and pelvis with contrast CT abdomen and pelvis without contrast US abdomen MRI abdomen and pelvis without and with contrast Symptoms: • Acute abdominal pain • No trauma • Fever Murphy +++ ?
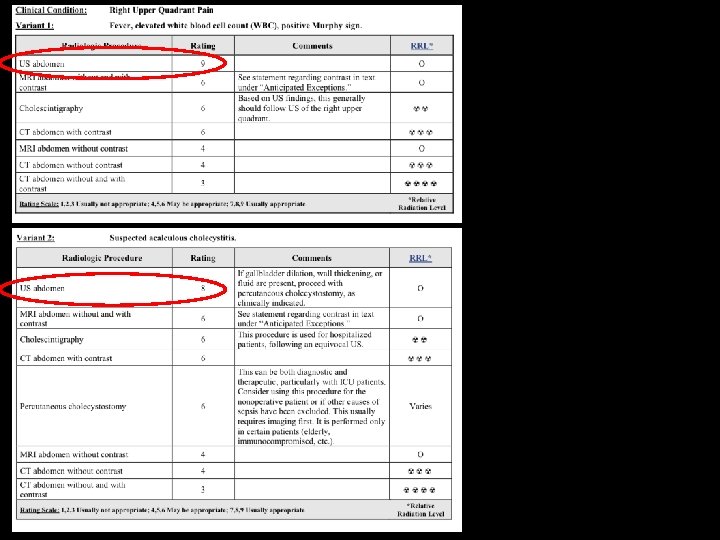

Case courtesy of Dr M Osama Yonso, Radiopaedia. org. From the article Acute acalculous cholecystitis

calculous cholecystitis

Radiologic signs • • Approximately 90 -95% of cases are due to calculus obstruction of the gallbladder neck or cystic duct, leading to increased intraluminal pressure and distention. Inflammation may result from chemical injury of the mucosa by bile salts and/or superimposed infection. Ultrasound (US) is the preferred initial modality in the investigation of right upper quadrant pain. It is more sensitive than HIDA scintigraphy 4 and CT in the diagnosis of acute cholecystitis, and more readily available. The most sensitive US finding in acute cholecystitis is the presence of cholelithiasis in combination with the ecographic murphy sign. Both gallbladder wall thickening (>3 mm) and pericholecystic fluid are secondary findings. Other less specific findings include gallbladder distension and sludge. Every effort should be made to demonstrate the obstructing stone in the gallbladder neck or cystic duct.

And…. If Murphy - - or the gallbladder is normal ? Differential diagnosis for acute cholecystitis includes: • • • choledocholithiasis pancreatitis peptic ulcer disease acute hepatitis liver abscess

pancreatitis

Abscess

Peptic ulcer

Acute hepatitis starry night sign

obstruction CASE • Patient presenting with abdominal pain, distension and failure of passage of flatus and stool and nausea. • No trauma Eventually • Vomiting • peritonism • sepsis and shock

Case • First study? – – – X – ray abdomen CT abdomen and pelvis with contrast CT abdomen and pelvis without contrast US abdomen MRI abdomen and pelvis without and with contrast

X – ray abdomen Case courtesy of Dr Frank Gaillard, Radiopaedia. org Case courtesy of Dr Varun Babu, Radiopaedia. org

• Second study? – – – X – ray abdomen with contrast CT abdomen and pelvis without contrast US abdomen MRI abdomen and pelvis without and with contrast
 accounts for 80% all mechanical intestinal obstruction. It has a")
Small bowel obstruction (SBO) accounts for 80% all mechanical intestinal obstruction. It has a mortality rate of 5. 5%. Causes can be divided into: • Congenital • Acquired causes may be extrinsic causing compression, intrinsic or luminal. In the developed countries, adhesions are by far the most common cause, accounting for ~75% of obstructions while in developing countries incarcerated hernias are much more common accounting for 80% of obstructions.

Ischemia

Caecal tumor

Femoral Hernia
 are often impressive on imaging, on account of the ability")
Large bowel obstruction (LBO) are often impressive on imaging, on account of the ability of the large bowel to massively distend. This condition requires prompt diagnosis and treatment. Large bowel obstructions are far less common than small bowel obstructions, accounting for only 20% of all bowel obstructions. Large bowel obstructions is age-dependant the most common cause is colonic cancer (50 -60%), typically in the sigmoid The second most common cause in adults is acute diverticulitis (involving the sigmoid colon). Together, obstructing tumours and acute diverticulitis account for 90% of all causes of large bowel obstruction.

faecoloma


Bowel cancer

Trauma chiuso Blunt Abdominal Trauma CASE 1 Signs and syntoms: • Patient presenting inconscious. • the anesthesiologist is not here, is pulling out the others or…. you have all the hospital behind, waiting…. looking and…. judging… • The only words writen are: “road accident” …. (good luck!) • • Dynamics? Speed? point of impact? A photo with whatsapp…. ?

Yea! A photo…here is it! choose

Do not trust about smoth impacts… Think bad always

And now…. • First study? – – – X – ray abdomen CT abdomen and pelvis with contrast CT abdomen and pelvis without contrast US abdomen MRI abdomen and pelvis without and with contrast Don’t worry…. there is the TRIAGE !! • US Fast DONE • X-ray DONE Do not trust if negative… maybe they made them……early?
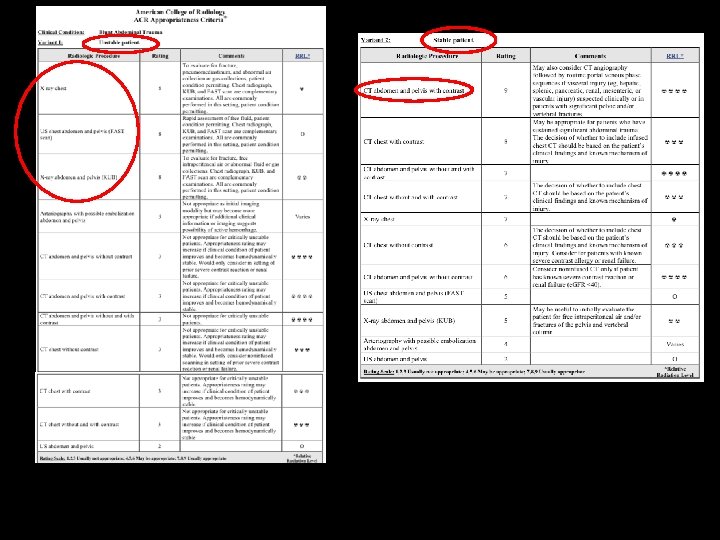

ABDOMINAL TC Abdominal trauma is responsible for 10%. The findings to look for in abdominal trauma are the following: • • Hemoperitoneum Contrast blush consistent with active extravasation Laceration: Linear shaped hypodense areas Hematomas: oval or round shaped areas Contusions: vague ill-defined hypodense areas that are less well perfused Pneumoperitoneum Devascularization of organs or parts of organs Nowadays there is a trend towards non-operative management of blunt abdominal trauma. More than 50% of splenic injury, 80% of liver injury and virtually all renal injurys are managed non-operatively, because patients proved to have better outcomes on the long term related to visceral salvage. www. radiologyassistant. nl CT in trauma

Laceration, no bleeding www. radiologyassistant. nl CT in trauma

Bleeding www. radiologyassistant. nl CT in trauma

Hematoma and bleeding www. radiologyassistant. nl CT in trauma

Renal trauma and spinal fracture www. radiologyassistant. nl CT in trauma

During the CT scan it comes the RX Bleeding? Where? www. radiologyassistant. nl CT in trauma

Thank you http: //www. learningradiology. com/medstudents/22 mustsformedstudents_files/v 3_document. htm http: //www. learningradiology. com/archives 2011/COW%20473 -Scapholunate%20 Disassociation/caseoftheweek 473 page. htm
- Slides: 65