RADIOLOGI BLOK KDS I RADIOLOGI THORAXABDOMEN NORMAL Tujuan

RADIOLOGI BLOK KDS I RADIOLOGI THORAX-ABDOMEN NORMAL
")
Tujuan Instruksional Umum Pada akhir praktikum mahasiswa diharapkan mampu : Mengidentifikasi anatomi radiologi (imaging) pada foto polos thorax normal. Mengidentifikasi anatomi radiologi (imaging) pada foto polos abdomen normal
")
Tujuan Instruksional Khusus Pada akhir praktikum mahasiswa diharapkan mampu : Mengidentifikasi anatomi radiologi (imaging) pada foto polos thorax normal. Posisi Simetrisasi Inspirasi Kondisi Mengidentifikasi anatomi radiologi (imaging) pada foto polos abdomen Posisi Organ-organ dalam rongga abdomen (dinding abdomen, hepar, renal out line, sistema tulang) Distribusi udara pada saluran pencernaan
. Mahasiswa harus sudah")
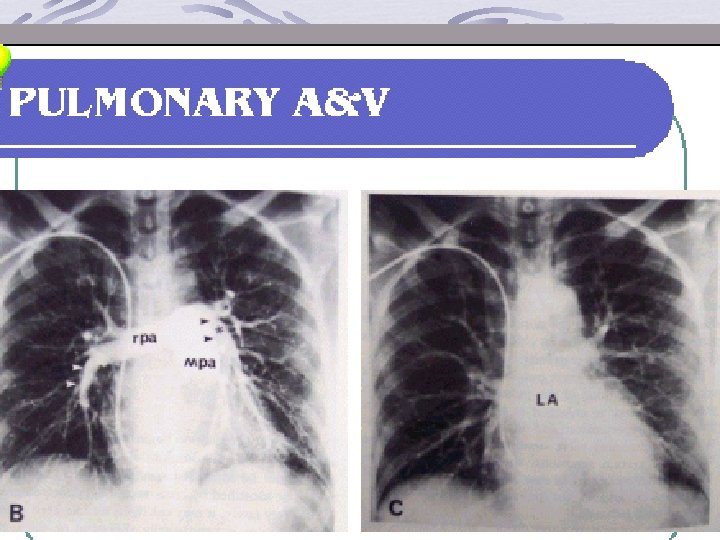
THORAX NORMAL Anatomi thorax normal identik gambaran radiologi (Imaging Thorax normal). Mahasiswa harus sudah menguasai anatomi thorax (jantung-paru-vaskularisasi & organ yang terlibat). Gambaran normal thorax kelainan

RIBS - HEART
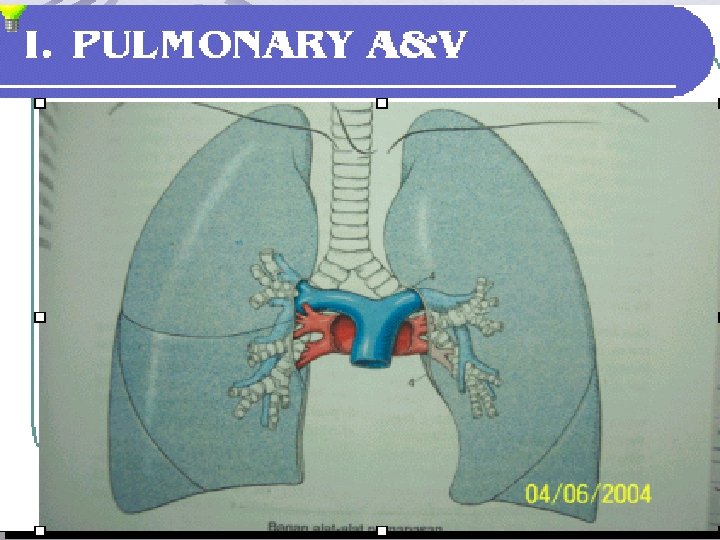

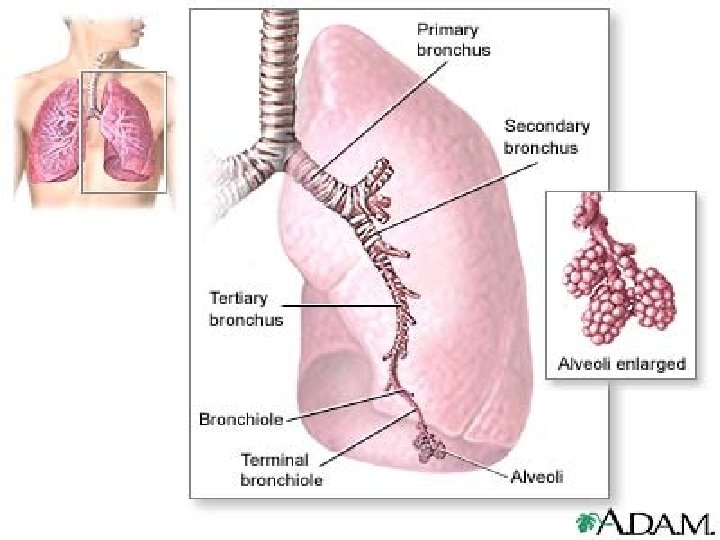
Anatomi Paru-Paru

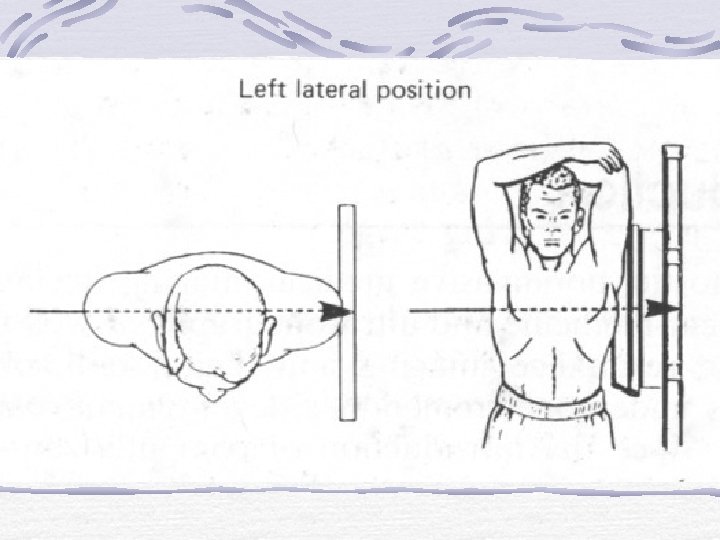
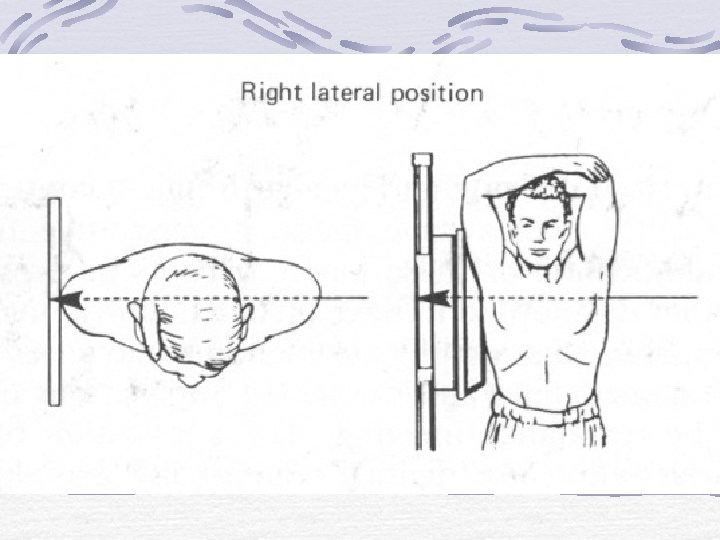
Anatomi Thorax, Lateral kiri

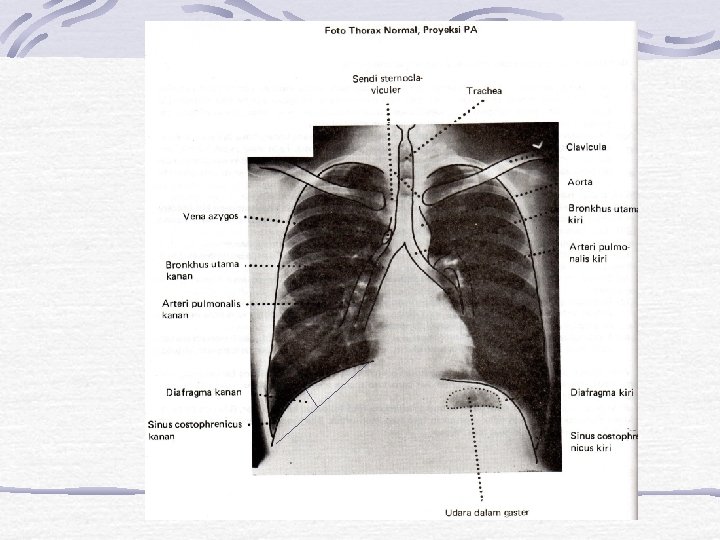
Anatomi Thorax, PA

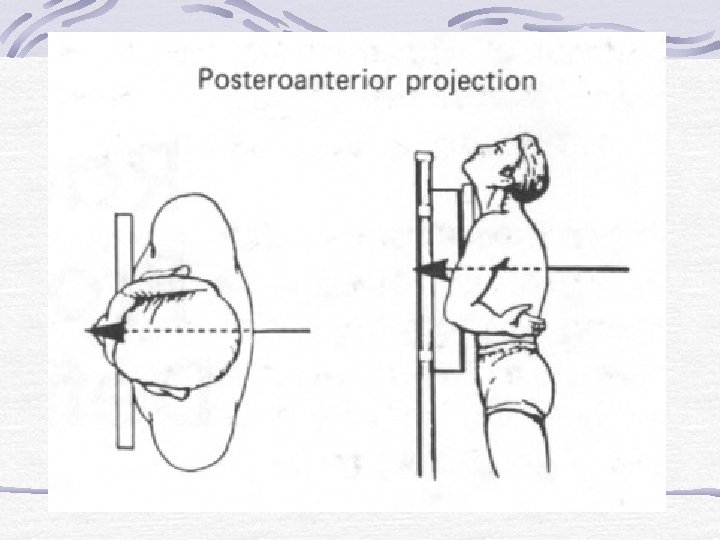
Gambaran Thorax Normal Posisi Posteroanterior & Lateral Pada Foto thorax normal, hal-hal yang perlu diperhatikan adalah : 1. Posisi 2. Simetrisasi 3. Inspirasi 4. Kondisi

Gambaran Thorax Normal Hal-Hal yang Harus diperhatikan : 1. Posisi 2. Simetrisasi 3. Inspirasi 4. Kondisi
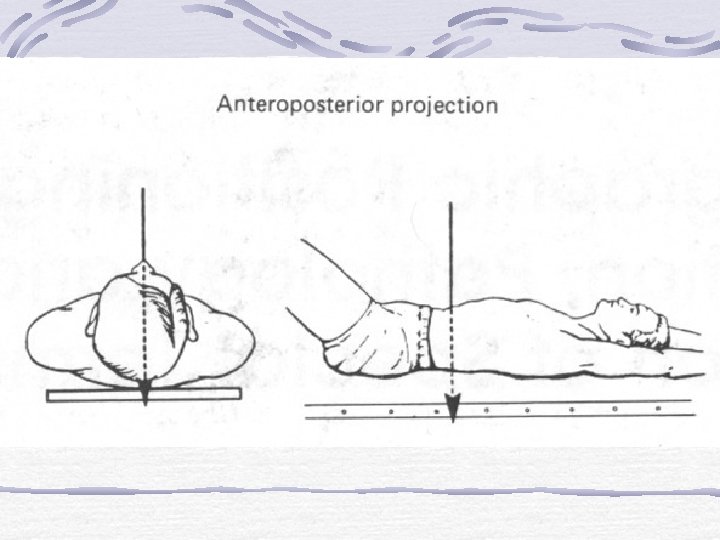
 AP (berbaring) DASAR PENILAIAN : 1. SCAPULA (DILUAR PARENKIM")
FAKTOR POSISI INTERPRETASI PA (berdiri) AP (berbaring) DASAR PENILAIAN : 1. SCAPULA (DILUAR PARENKIM PARU) 2. CLAVICULA (curam) 3. UDARA FUNDUS GASTER (MEGENBLASE)

PA AP

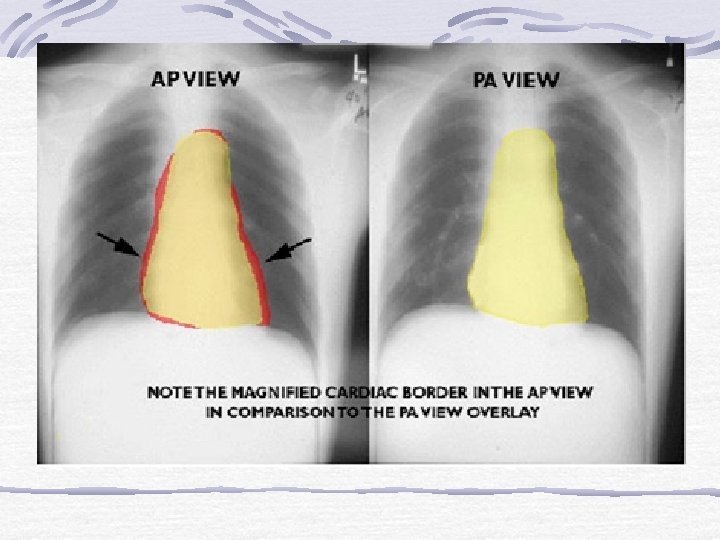
AP versus PA The Effect of Magnification l In a PA film, the heart is closer to the film and thus less magnified n l The standard chest x-ray is a PA film In an AP film, the heart is farther from the film and is more magnified n Portable chest x-rays are almost always done AP

AP versus PA The Effect of Magnification AP portable film makes the heart look larger than it does… On this PA film done on the same patient an hour later
 CARA : JARAK YANG SAMA")
FAKTOR SIMETRISASI Jarak ujung clavicula dengan processus spinosus (simetris/tidak) CARA : JARAK YANG SAMA ANTARA PROCESSUS SPINOSUS KE SENDI STERNOKLAVIKULA KANAN DAN KIRI

Rotation If the spinous process of the vertebral body is equidistant from the medial ends of each clavicle, there is no rotation
, the patient is")
If spinous process appears closer to the right clavicle (red arrow), the patient is rotated toward their own left side If spinous process appears closer to the left clavicle (red arrow), the patient is rotated toward their own right side

Pitfall Due to Marked Rotation Severe rotation may make the pulmonary arteries appear larger on the side farther from the film

FAKTOR INSPIRASI DASAR PENILAIAN : PENAMPAKAN DIAFRAGMA PATOKAN : VT X / COSTA BELAKANG 10 /COSTA DEPAN 6 INTERPRETASI : CUKUP KURANG TERLALU DALAM

Inspiration l l About 10 posterior ribs visible is an excellent inspiration In many hospitalized patients 9 posterior ribs is an adequate inspiration

Anterior vs. Posterior Ribs Anterior ribs will be Posterior visible but ribs are harder those that to see. They are most run more apparent on or less at a the chest x 45 degree ray. They angle run more How to tell the difference betweendownward or less toward the anterior and the posterior ribs horizontally. feet.

10 Ten posterior ribs showing is an excellent inspiration

Pitfall Due to Poor Inspiration 8 About 8 posterior ribs are showing Poor inspiration will crowd lung markings and make it appear as though the patient has airspace disease

Same patient 8 9 About 8 posterior ribs are 9 -10 posterior ribs are showing Better inspiration and the “disease” at the lung bases has cleared

KONDISI FOTO THORAX DINILAI DARI : 1. 2. 3. KONDISI PULMO KESELURUHAN (LUSENSI PARENKIM PARU) VERTEBRA THORAKALIS TAMPAK I-IV (< VT II KURANG, > VT VI KERAS) PROCESSUS SPINOSUS TAMPAK 3 ATAU 4 INTERPRETASI : KERAS (TERLALU HITAM/LUSENS) CUKUP KURANG (TERLALU PUTIH/OPAQUE)

kondisi You should be able to just see thoracic spine through the heart.

TERPOTONG ATAU TIDAK DASAR PENILAIAN: SUPERIOR: TAMPAK VERTEBRA CERVIKALIS VI/VII INFERIOR: SINUS COSTOPHRENICUS DAN DIAFRAGMA SAMPING KANAN DAN KIRI: AXILLA TAMPAK
 IDENTITAS REGISTRASI NAMA, UMUR, NO. REGISTER, TANGGAL")
IDENTITAS SISI MARKER (L ATAU R) IDENTITAS REGISTRASI NAMA, UMUR, NO. REGISTER, TANGGAL FOTO LAYAK / TIDAK ?

Hal-hal yang harus diperhatikan dalam Pembacaan Foto Polos Thorax a. Jaringan lunak, tulang b. Corakan bronkhovaskuler c. Parenkim paru Keadaan hilus d. Sinus costofrenikus e. Diafragma f. Cor : CTR

SISTEMA TULANG DAN JARINGAN LUNAK LOKASI DAN GAMBARAN SISTEMA TULANG : COSTA, CLAVICULA SCAPULA LOKASI DAN GAMBARAN JARINGAN LUNAK MAMMAE, normal: sistem tulang intak

KEDUA APEKS PARU PENILAIAN : TENTUKAN LOKASI APEKS PARU GAMBARAN APEKS INTERPRETASI APEKS TENANG/ BERSIH APEKS TERDAPAT INFILTRAT ( UKURAN DAN BENTUK, DENSITAS)

KEDUA APEKS PARU APEKS TENANG TERDAPAT PENINGKATAN DENS DI APEKS KANAN

CORAKAN BRONKHOVASKULER CARA PENILAIAN BAGI PARU DARI TEPI MENJADI 3, LIHAT BAGIAN 1/3 LATERAL NORMAL : CORAKAN BRONKHOVASKULER TIDAK MELEBIHI 2/3 MEDIAL (1/3 LATERAL TAMPAK BERSIH) INTERPRETASI: NORMAL /MENINGKAT

CORAKAN BRONKHOVASKULER NORMAL MENINGKAT

PARENKIM PARU GAMBARAN PARENKIM PARU APABILA TERDAPAT INFILTRAT: TENTUKAN : LOKASI, UKURAN, JUMLAH, BENTUK

PARENKIM PARU

SINUS COSTOPHRENICUS INTERPRETASI LANCIP ATAU TUMPUL NORMAL : LANCIP BILA TUMPUL PASTIKAN ADA KELAINAN ATAU TERPOTONG

SINUS COSTOPHRENICUS TERPOTONG EFUSI PLEURA

Normal R costophrenic angle. Blunted L costophrenic angle When 200 -300 cc of fluid accumulate in pleural space, the usually acute costophrenic angle (sulcus), as seen on the right in this person, becomes blunted (as seen on the left in this person)
 Selisih <3 cm)/ atau")
DIAFRAGMA NORMAL : Kanan lebih tinggi dari kiri (jantung menekan) Selisih <3 cm)/ atau sebagai patokan tidak lebih dari 2 vertebra Licin

JANTUNG LOKASI BENTUK JANTUNG CTR : NORMAL < 0, 5 UNTUK BERDIRI /PA

Cardio-thoracic Ratio One of the easiest observations to make is the cardio-thoracic ratio which is the widest diameter of the heart compared to the widest internal diameter of the rib cage CTR= (a+b) /c = < 50% a b c

Enlarged or not? Yes

Enlarged or not? Yes

Enlarged or not? No

Contoh Pembacaan Foto Thorax Normal Foto Thorax PA, errect, simetris, inspirasi dan kondisi cukup Tidak ada soft tissue swelling Sistema tulang intak tampak kedua apex paru tenang tampak corakan bronkhovaskuler di kedua lapangan paru normal sinus costophrenicus kanan-kiri lancip Diafragma kanan dan kiri licin Cor : CTR kurang dari 0, 56 Kesan : Paru dan cor dalam batas normal

Abdomen Normal Hal-hal yang harus diperhatikan pada Foto Polos Abdomen, adalah : Gambaran udara Usus Gambaran jaringan lunak (soft tissue) Gambaran organ-organ intra abdominal Hepar Lien Renal Tract Urinarius dan Genitalia
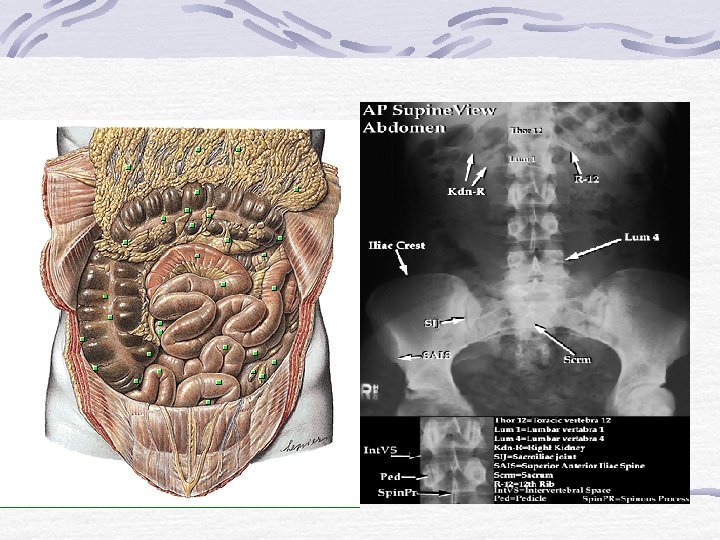

Gambaran Soft Tissue & Organ-organ Intra abdominal Soft tissue Preperitoneal fat line Psoas line Organ-organ Intra abdominal Hepar Lien Renal

FOTO POLOS ABDOMEN A Normal plain film of the abdomen. The lower margins of the posterior portion of the liver, the hepatic angle (H), and the lower part of the spleen (S) are delineated by a fat shadow. Both kidneys (K) and the psoas muscle shadows (arrowheads) are outlined by a fat shadow. The properitoneal fat stripe is also shown bilaterally (arrows). B Diagram of normal abdominal plain film.

Gambaran Foto Polos Abdomen

FOTO POLOS ABDOMEN Normal Gas Pattern Gas in stomach Gas in a few loops of small bowel D = 2. 5 CM Gas in rectum or sigmoid ALMOST ALWAYS

FOTO POLOS ABDOMEN Always air/fluid level in stomach A few air/fluid levels in small bowel Erect Abdomen

Gambaran Udara usus
 udara")
Gambaran Foto Polos Abdomen Neonatus udara di lambung (10 -15 menit setelah kelahiran) udara di proksimal usus halus 30 -60 menit setelah kelahiran udara di bagian distal usus halus 6 jam setelah kelahiran udara di colon dan rektum 24 jam setelah lahir. Gambaran soft tissue dan organ-organ intra abdominal minimal
 perifer dan usus besar (foto abdomen dengan kontras)")
Gambaran Udara pada usus halus (sentral) perifer dan usus besar (foto abdomen dengan kontras)

Contoh Pembacaan Foto Abdomen. Normal Foto Polos Abdomen, AP, Supine, kondisi cukup tampak preperitoneal fat line jelas Psoas line tegas dan simetris Renal out line jelas Tampak udara usus (+), tak tampak gambaran distensi usus Sistema tulang baik Kesan : Tak tampak kelainan pada abdomen
- Slides: 71