Radiation Therapy Oncology Group RTOG SemiAnnual Meeting Tampa
 Semi-Annual Meeting Tampa, Florida February 3, 2007")
 Disparities Project Michael L. Steinberg, MD, FACR Principal")































 18 11 Accepted Navigation Declined Navigation")
















 accepted navigation 62 (57.")

 n Race n Education n Religion n")
 on 8 of 9 metrics using")

 on 3 of 5 scales: Physical")
 Refused navigation: 17.")



 Patients")










 Disparities Project at Centinela Freeman Regional")
- Slides: 74
Radiation Therapy Oncology Group (RTOG) Semi-Annual Meeting Tampa, Florida February 3, 2007
Urban Latino African American Cancer (ULAAC) Disparities Project Michael L. Steinberg, MD, FACR Principal Investigator David Huang, MD Co-Investigator Nicole Harada, CCRC, CCRP Clinical Trials Coordinator/Data Manager
Component Updates n Administrative n Navigation n Clinical Trials n Telesynergy/Telemedicine n Quality Assurance n Publications, Articles, and Presentations n Work in Progress
Administrative Component
Our Partners n Centinela Freeman Regional Medical Center n n RAND Corporation n Allen Fremont, MD, Ph. D Nell Forge, Ph. D , Co-Investigator USC Norris Comprehensive Cancer Center n n Michael L. Steinberg, MD, FACR, Principal Investigator David Khan, MD, Co-Investigator David Huang, MD, Co-Investigator Oscar Streeter, MD , Co-Investigator UCSF Comprehensive Cancer Center n Mack Roach, MD , Co-Investigator
Infrastructure Project Staff: Debbie Karaman, MPH, Community Health Educator n Erika Cobb, Program Administrative Assistant n Herschel Knapp, Ph. D, MSSW n Nicole Harada, Clinical Trials Coordinator n Susan Richardson, RN, Oncology Nurse n Keith Andre, MA, Project Administrator n
Community Liaison n Community Advisory Board n n Investigators’ Meeting n n Meets two times per year Medical Advisory Board n Meets 6 times per year
Navigation Component
Our Patients
Abnormal Results Patient Navigation Rehabilitation Diagnosis Treatment Conclude Navigation Abnormal Finding Outreach Resolution Cancer Diagnosis Cancer Disparities Research Partnership (CDRP) Patient Navigation Model Freeman, et. al. , Cancer Practice, 1995.
Patient Navigator Training Program n The 9 -hour navigator training course emphasizes: n Investigating and implementing resources for patients in a timely fashion n Listening compassionately and non-judgmentally n Completing appropriate records of all interactions on behalf of patient n Empowering patients to self-advocate in the healthcare realm
Training Program
Active Navigators
Reasons for Navigator Attrition
Gender of Active Navigators
Ethnicity of Active Navigators
Cancer Survivor Status of Active Patient Navigators
Patient Data
Patients Offered Navigation By Project Year
Ethnicity of Patients Offered Navigation
Percentage of each Ethnicity Accepting Navigation * Small sample size
Percentage of Patients Accepting Navigation By Ethnicity
Measuring the Effectiveness of Barrier Solution Identification n Patient-specific barriers to care identified during the patient intake conducted by a navigator n Records are maintained and audited to determine number of days to barrier solution identification n Barrier solution includes assigning a navigator (psychosocial barriers) and identifying community resources (functional barriers)
Premise n n n Barriers to care increase the likelihood that the patient will not be able to comply with treatment and followup regimens Barriers to care increase the likelihood that the patient will not participate in a clinical trial Addressing barriers to care will increase compliance and likelihood of clinical trials participation
6 Most Common Barriers
Barriers to Care: Chart Audit PT ID# Dx Barriers 009 Colon 1. Transportat ion 2. Financial Navigator Assigned Date of Review Date closed Days open Resources Did ULAAC Identified staff assist Navigator? 131 04/29/05 04/30/05 2 Taxi voucher program No 131 04/29/05 04/30/05 2 Beckstrand Cancer Foundation No
Mean Number of Days to Barrier Solution Identification
Percentage of Barriers Solutions Identified in One Day
Clinical Trials
Trials Open for Accrual Name of Trial Name of Sponsor Prostate Patient Profiles Project (P 4) Louis Warschaw Prostate Cancer Center @ Cedars Sinai RTOG 0413 National Cancer Institute RTOG 0232 National Cancer Institute NCIC CTG MA. 20 National Cancer Institute of Canada RTOG 0123 NCI RTOG 0214 NCI SWOG S 0424 NCI
Trials Closed to Accrual Name of Trial Name of Sponsor RTOG 0321 National Cancer Institute RTOG 98 -04 National Cancer Institute RTOG 0315 National Cancer Institute 2003 -02 DCIS CYTYC Surgical
Patients Accrued to Trial
Accrual to Trial by Ethnicity
Clinical Trial Accrual/Navigation 29 Patients (31 Enrollments) 18 11 Accepted Navigation Declined Navigation
Telesynergy/Telemedicine
Telesynergy Telemedicine
Telesynergy Usage n Tumor Boards n Meetings with partners and mentoring institutions n Meetings with CDRP sites
Quality Assurance
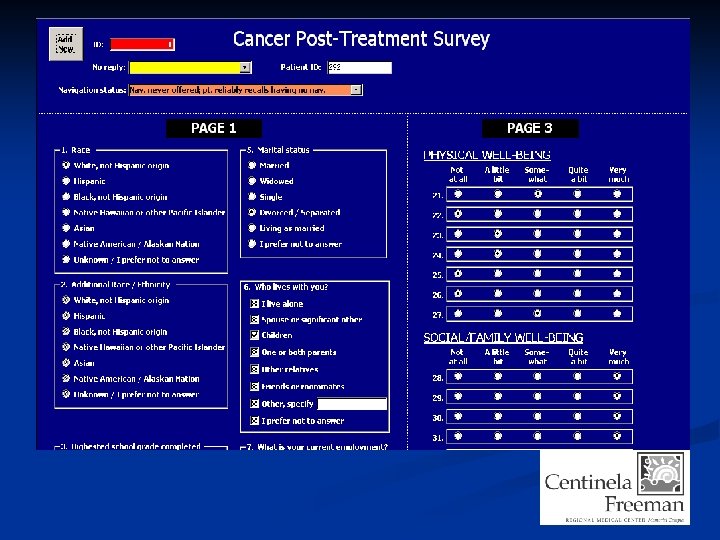
Instruments *Patient Satisfaction Survey n *Cancer Post Treatment Survey n *Clinical Trial Questionnaire n Rand Process Instrument – In Process n
Patient Satisfaction Survey 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. The patient navigator was courteous. The patient navigator was sensitive. The patient navigator was respectful. The patient navigator was friendly. The patient navigator was thorough. I valued working with the navigator. The education materials I received were helpful. Support services referrals met my needs. I received financial information (if needed). I would recommend this service to others. Response: 5 point Likert Scale Strongly Agree = 5, Strongly Disagree = 1 N/A option offered on each question
Sample method Each month, 10% of patients are randomly selected for telephone navigator service satisfaction survey.
Q: Does the navigator’s cancer history predict patient satisfaction? In other words: Do you have to have had cancer in order to provide effective cancer navigation?
Navigators without a hx. of CA outperformed navigators w/ CA hx. on 60% of patient satisfaction metrics.
Statistically Significant Differences Individual ANOVA test revealed a statistically significant difference on question 7 (only).
Overall patient satisfaction exceeds 90% with navigator services regardless of navigator’s cancer history (p =. 953). Note: 5 -point Likert scale scores presented as satisfaction percentages
Final Question on Survey Would you like to continue with the Patient Navigator Program? I would like to continue working with my navigator. I would like to have a different navigator assigned to me. I would like to discontinue receiving navigation.
94. 7% of patients surveyed chose to continue navigation. Navigator’s CA hx. does not predict patient satisfaction (X 2: p =. 329. )
Provisional Findings Overall, there is no statistically significant difference in patient satisfaction when comparing navigators who have had cancer to navigators who have not had cancer. In other words: All helping hands are good hands and 95% of patients were satisfied and wished to continue navigation
Further analysis pending accumulating n Correlative analyses to explore navigator / patient metrics: Navigator characteristics: age, gender, education, race / ethnicity, marital status, number of patients Patient post-tx metrics: navigated vs. not-navigated, age, gender, race / ethnicity, education, religion, marital status, income, geography, treatment satisfaction, wellbeing metrics: physical, social, emotional, functional, spiritual).
Cancer Post-Treatment Survey Compares patients who accepted / refused navigation services at four levels: n Reason(s) for refusing navigation n Demographics n Treatment satisfaction scale n FACIT (Functional Assessment of Chronic Illness Therapy) instrument
Sample characteristics 107 patients were offered navigation 45 (42. 1%) accepted navigation 62 (57. 9%) refused navigation
Reasons for refusing navigation 85% 68% 47% 44% 42% 23% 13% 8% I am an independent person I have a supportive family I am a private person I have supportive friend(s) I am a spiritual / religious person Navigation seemed unnecessary I was unclear on what the navigator would do The role of the navigator seemed intrusive to me
Demographics No significant differences (p >. 05) n Race n Education n Religion n Marital status n Living conditions n Income
Treatment Satisfaction No significant differences (p >. 05) on 8 of 9 metrics using a 1 – 4 Likert scale (1 = never, 4 = always): During my cancer treatment, I had good communication with my care providers. Accepted navigation: 2. 85 Refused navigation: 2. 54 } (p =. 037)
FACIT instrument Patient self-evaluation multi-scale instrument Measures 5 areas of well being using 5 point Likert scales (1 = not at all, 5 = very much) n n n Physical 7 questions Social / Family 7 questions Emotional 6 questions Functional 7 questions Spiritual 12 questions
FACIT Scores No significant differences (p >. 05) on 3 of 5 scales: Physical n Social / Family n Spiritual n
FACIT Scores Emotional Well-Being Accepted navigation: 20. 65 (p =. 025) Refused navigation: 17. 91 } Functional Well-Being Accepted navigation: 21. 85 Refused navigation: 17. 13 } (p =. 012)
Do Navigators Make a Difference in Acceptance of Clinical Trials? n Challenges: n Small n n the reality of the number of patients eligible for clinical trial in a community hospital n process change required to ensured the early presence of a navigator in CT discussions
Do Navigators Make a Difference in Acceptance of Clinical Trials? n Preliminary impressions suggest that early inclusion of a navigator in discussions with patients about clinical trials is associated with an increase rate of participation
Do Navigators Make a Difference in Acceptance of Clinical Trials? n Of patients eligible for a trial who have a navigator present at CT discussions n n 80% accept 20% decline n n n = 5 Only 1*/9 pts who declined had navigator input * perception of non coverage by insurance (managed care)
"Will get closer follow-up" as primary reason for patient accepting CT (navigator observation) Patients who accepted CT with a navigator present at CT discussions gave as stated reason for acceptance n Of eligible patients who do not have a navigator present at CT discussions: n q 0% give “Will get closer follow up” as their primary reason for participating
Presentations, Articles, and Publications
Publications n Lay Patient Navigator Program Implementation For Equal Access To Cancer Care And Clinical Trials: Essential Steps And Initial Challenges Cancer, Volume 107, Issue 11 , Pages 2669 – 2677 n Preliminary results and evaluation of Mammo. Site® balloon brachytherapy for partial breast irradiation for pure ductal carcinoma in situ: A phase II clinical study n In press, The American Journal of Surgery
Presentations n “National Leadership Summit on Eliminating Racial Disparities in Health” n n January 9 -11, 2006 Washington, D. C. “Prophylactic Post-Operative Antibiotics for Prostate Brachytherapy” n Presented at the 2006 Prostate Cancer Symposium at ASCO in 2006
Presentations n Preliminary results and evaluation of Mammo. Site® balloon brachytherapy for partial breast irradiation for pure ductal carcinoma in situ: A phase II clinical study n n Developing a Lay Patient Navigator Program Addressing Barriers to Care and Participation in Clinical Trials n n Presented at the American Society of Breast Surgeons Meeting, April 2006 Presented at the Cancer REACH 2010 Conference, May 2006 Using Telesynergy® to Improve Access to Clinical Trials at an Underserved Community Based Hospital n Submitted to ASTRO, November 2006
Presentations n The Use of Lay Patient Navigators to Improve Quality of Care and Accrual to Clinical Trials for Radiation Oncology Patients Who Are Minorities or of Low Socioeconomic Status n n Do Navigators Make a Difference in Acceptance of Clinical Trials? n n Presented at ASTRO 2006, Philadelphia, PA, Nov. 5 -9, 2006 Presented at ASTRO 2006, Philadelphia, PA, Nov. 5 -9, 2006 Disparity in Cancer Treatment and Outcome n Presented at Mid-Winter Oncology Meeting, Los Angeles, Ca. Jan 23, 2007
Poster Presentations n A Lay Patient Navigator Program as Part of a Clinical Trials Infrastructure in a Community Hospital Serving Minority and Low Income Patients n Poster Presentation at the Cancer Health Disparities Summit 2006, Bethesda, MD, July 17 -19, 2006 n Lay patient navigator program for equal access to cancer care and clinical trials n Poster presentation at ASTRO Health Services/Outcomes Research In Radiation Oncology, San Diego, CA September 15, 2006
Work in Progress
Work in Progress n Spanish Support Group: n n Susan B. Komen Foundation Grant: n n To provide comfort, support, and education for Latinos undergoing cancer treatment in the community To train monolingual Latino navigators for the Breast Center at Centinela Campus, to help Spanish-speaking women access resources for treatment, to establish continuity of care, and to promote annual screening NCCCP: n To establish a comprehensive cancer center of excellence and to incorporate navigation in medical oncologists’, pathologists’, and surgeons’ medical practices to facilitate pre-treatment barrier reduction
Work in Progress n Relocation of ULAAC Office to Centinela Campus: n n Telesynergy/Telemedicine: n n To capture oncology patients for navigation and to help them access resources for treatment To relocate to Centinela Campus for better utilization HRSA Nursing Workforce Grant: n To train nurses of all discipline to close the shortage gap. Also to encourage professional nurses to enhance and refine their training and education
Disparity is about Poverty and Lack of Infrastructure designed to Deal With the Indigent Patient’s Needs
Contact Us Urban Latino African American Cancer (ULAAC) Disparities Project at Centinela Freeman Regional Medical Center, Memorial Campus 333 North Prairie Avenue Inglewood, CA 90301 Telephone: (310) 674 -7050, extension 4661 Fax: (310) 671 -8299 Email: mls@cccma. com Principal Investigator: Michael L. Steinberg, MD, FACR